
Abstract
Background and Purpose:
Throughout the literature, the ureter is described as having three anatomic sites of narrowing at which kidney stones typically become lodged: The ureteropelvic junction (UPJ), the ureteral crossing of the iliac vessels, and the ureterovesical junction (UVJ). There is little evidence to support this notion, however. The purpose of our study is to evaluate whether three peaks in stone distribution corresponding to these anatomic landmarks exist.
Methods:
We retrospectively reviewed the kidneys-ureters-bladder (KUB) films of 622 patients with solitary ureteral calculi referred for shockwave lithotripsy (SWL). Pretreatment KUB films were used to categorize the location of their ureteral stone relative to 1 of 19 levels referenced to the axial skeleton. CT scans of 74 patients were used to determine the location of the UPJ, ureteral crossing of the iliac vessels, and UVJ relative to the 19 levels on KUB radiography. Histograms were then constructed to plot the distribution of stones within the ureter relative to these 19 levels. The effect of sex, stone size and side, and presence of a stent on stone distribution were analyzed.
Results:
There are two peaks in the distribution of stones within the ureter in patients referred for SWL that correspond to the UPJ/proximal ureter and intramural ureter/UVJ. In patients with larger stones (≥100 mm2) or a ureteral stent in place, stones were distributed more proximally (P<0.0001). When comparing sexes, there was a difference in stone distribution that approached significance (P=0.0523), with a greater peak more distally in males compared with females.
Conclusions:
Our review demonstrates a peak in the distribution of stones corresponding to the UPJ/proximal ureter and the intramural ureter/UVJ. We failed to demonstrate a peak in stone distribution corresponding with the ureteral crossing of the iliac vessels.
Introduction
The final site of narrowing, which represents a true reduction in ureteral caliber to 5F to 9F, occurs at the ureterovesical junction (UVJ) where the ureter courses through the bladder wall to the ureteric orifice. 1,6 The intramural ureter, therefore, represents the narrowest portion of the ureter. 6 Diagrams from the 1st edition of Campbell's Urology 7 and the most recent (9th) edition of the Campbell-Walsh Urology 1 textbook illustrate this anatomy pictorially (Fig. 1).
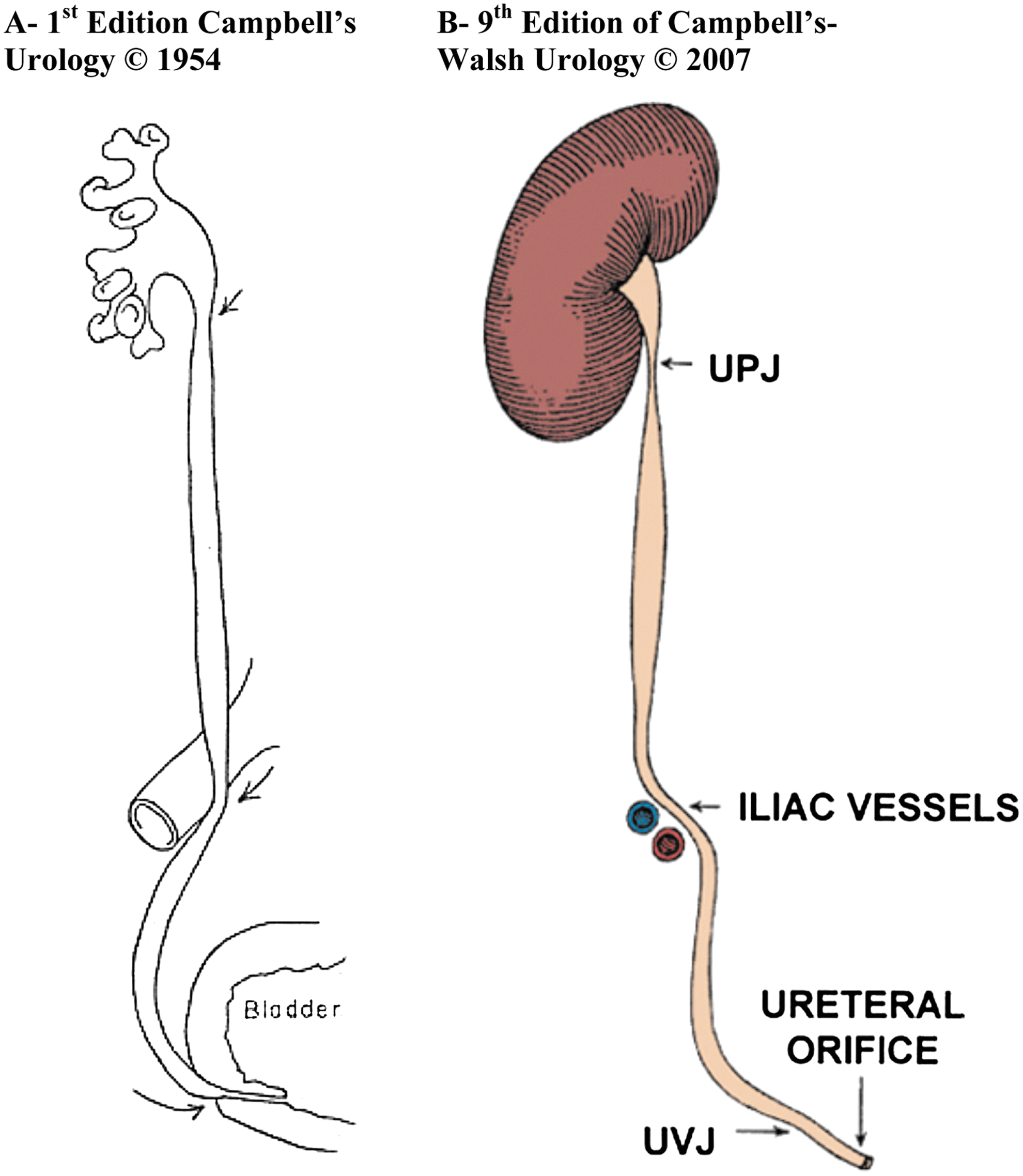
Illustrations A and B both demonstrate the normal functional or anatomic narrowing at the ureteropelvic junction (UPJ), the iliac vessels, and the ureterovesical junction (UVJ). Illustrations reproduced with permission of Elsevier Inc.
The existence of three sites of narrowing within the course of the ureter at which stones become lodged continues to be taught, 1,6 despite any evidence in the literature to support this. Assuming the above statement is correct, one would expect to find three peaks in stone distribution along the course of the ureter corresponding to these sites if the location of stones that have not passed spontaneously were plotted. Based on our clinical experience over the years, in addition to the absence of any anatomic narrowing of the ureter as it crosses anterior to iliac vessels on direct visualization with endoscopy, we questioned the traditional teaching that stones lodge at a point of narrowing in the midureter as it passes over the iliac vessels. The purpose of this study was to test our hypothesis that stones do not tend to lodge at the level of the iliac vessels.
Our group was the first to test this hypothesis when we presented our results at the American Urological Association meeting in 2007 and published an abstract in the Journal of Urology. 8 We now present our expanded review and results.
Methods
Patients referred for shockwave lithotripsy (SWL) at the lithotripsy unit of St. Michael's Hospital in Toronto, Ontario, Canada are entered into a prospectively maintained database called Lithotrack.™ Before treatment, on arrlval at the lithotripsy unit, patients are sent for kidneys-ureters-bladder (KUB) radiography to confirm the presence and location of the calculus. From this database, we were able to identify 622 patients with solitary ureteral calculi who were referred for SWL treatment over a 5-year period. This time frame was selected because all films could be viewed digitally on a PACS system. Patient and stone demographics, including sex, side and size of the stone, and presence of a ureteral stent, were recorded.
During review of the KUB films, calculi were identified and their locations were recorded at one of 19 levels referenced to the axial skeleton projected on the KUB (Fig. 2). The first 12 levels corresponded to the upper, middle, and lower aspects of the first through fourth lumbar vertebrae. Levels 13 through 15 corresponded to the ureteral course from the disc space between the fourth and fifth lumbar vertebrae to the distal aspect of the sacral ala. Levels 16 through 18 corresponded to the ureteral course from the lower aspect of the sacral ala to the ischial spines. Finally, stones located on a line drawn between the ischial spines were assigned to level 19, which is thought by radiologists to represent the UVJ. 9
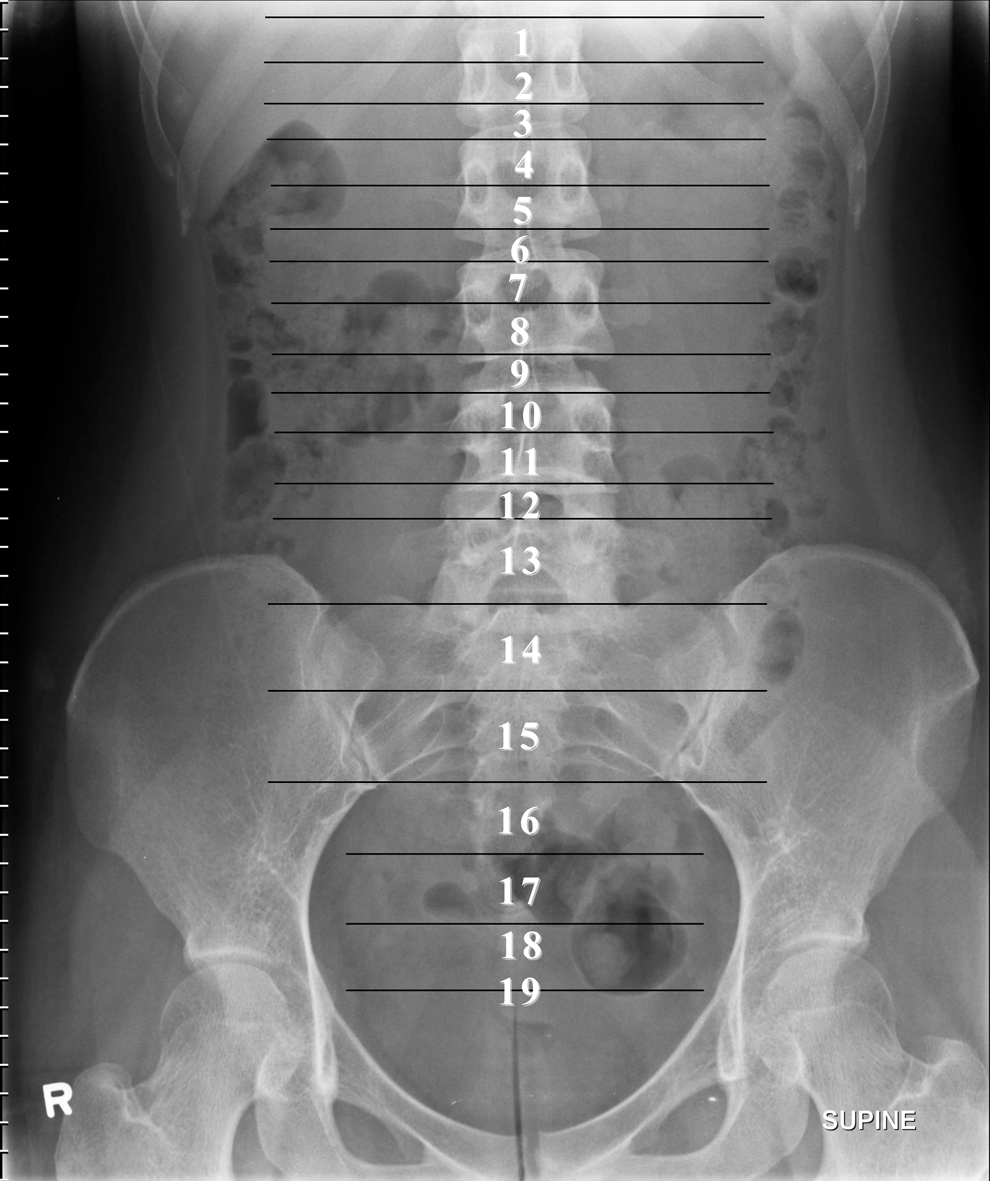
Nineteen anatomic levels referenced to the axial skeleton on kidneys-ureters-bladder radiography.
A stone location histogram was then constructed, based on the KUB radiography of the 622 patients, to determine the frequency of stones residing at each of the 19 locations in the ureter at the time of treatment. Separate histograms were constructed, and the Wilcoxon rank sum test was used to assess for a statistically significant effect of gender, stone side, stone size or presence of a stent on stone location. The chi-square test was used to evaluate for differences in presence of stent based on sex and stone size. The Student t test was used to assess for differences in stone size based on sex. All statistical analysis was performed using SAS software version 9.2 (SAS Institute, Cary, NC).
Of the above cohort, 74 patients had undergone a noncontrast CT scan, at our center, on the day of or within 4 weeks of treatment. The axial and coronal images were correlated with the scout film from these CT scans to determine the location of the UPJ, ureteral crossing of the iliac vessels, and UVJ relative to the 19 levels referenced to the axial skeleton on KUB. Ureteral anatomy histograms were then constructed using the data collected from the CT scans of these 74 patients to delineate the most frequent site of the UPJ, UVJ, and ureteral crossing of the iliac vessels. Subsequently, the knowledge of the anatomic location of the UPJ, UVJ, and ureteral crossing of the iliac vessels on KUB would then allow us to determine if there was a peak in the constructed stone location histogram at these sites.
Results
We identified 622 patients with a solitary ureteral stone referred for SWL treatment at our center. Demographic data are summarized in Table 1. In this cohort, 458 (73.6%) patients were male and 164 (26.4%) patients were female yielding a male to female ratio of 2.8:1, which is typical of our population of stone formers. 10 Stones were situated relatively equally on the left (52.1%) and right side (47.9%) of patients. Pretreatment stent insertion had been performed in 156 (25.1%) patients. In the majority of patients (84.2%) the total stone area was <100 mm2, with the average stone area being 61.30 mm2. Chi-square test showed that females were significantly more likely to have a stent than males (odds ratio (OR) 1.56, confidence interval (CI) 1.19, 2.06, P=0.0018). As would be expected, patients were more likely to have a stent if they had a stone ≥100 mm2 compared with <100 mm2 (OR 2.44, CI 1.89, 3.18, P<0.0001). There was no statistically significant difference in stone area between sexes.
SD=standard deviation.
There were 74 patients who had a CT scan in our hospital within 4 weeks before treatment. We were able to determine the location of the UPJ, ureteral crossing of the iliac vessels, and UVJ relative to the corresponding 19 levels referenced to the axial skeleton on KUB, by correlating the axial and coronal CT images with the scout film in these patients. The UPJ was typically at the lower border of the L2 vertebrae (ie, position 6) on the left and the upper border of the L3 vertebrae (ie, position 7) on the right (Fig. 3a). The ureteral crossing of the iliac vessels was predominantly located at the upper half of the sacroiliac joint (ie, position 14) on both the left and right sides (Fig. 3b). The UVJ was most frequently found to be just above the ischial spines (ie, position 18) (Fig. 3c).

The histogram in Figure 4 represents the stone distribution, expressed as a percentage of the total number of stones, at each of the radiographic levels. There are two peaks in the distribution of stones within the ureter that correspond to the UPJ/proximal ureter and intramural ureter/UVJ (Fig. 4). The first peak occurs at the lower border of the L2 vertebrae and upper border of the L3 vertebrae. The second peak occurs within the true pelvis, just above the ischial spines.

Histogram of stone location distribution in the entire cohort (n=622). KUB=kidneys-ureters-bladder; UPJ=ureteropelvic junction; MU=midureter; IV=iliac vessels; DU=distal ureter; UVJ=ureterovesical junction.
The effect of sex, stone side and size, and stent presence on stone distribution was examined using the Wilcoxon rank sum test. Comparing patients with a stent with those without a ureteral stent showed a statistically significant (P<0.0001) shift in the distribution of stones proximally to the upper ureter (Fig. 5). This is as would be clinically expected, because stones lodged in the upper ureter are often both larger and thought to be less likely to pass spontaneously and therefore are more likely have stent placement. Furthermore, some stones were likely pushed back more proximally during stent insertion. Considering that in these patients with stents the stone location with the stent in place may not represent the original location where the stone became lodged, a histogram of stone distribution was constructed excluding the stented patients. Figure 6 demonstrates the distribution of stones in the cohort of patients without a stent (n=466). Similar to the entire cohort, two peaks in stone distribution are seen within the ureter, which correspond to the UPJ/proximal ureter and intramural ureter/UVJ.
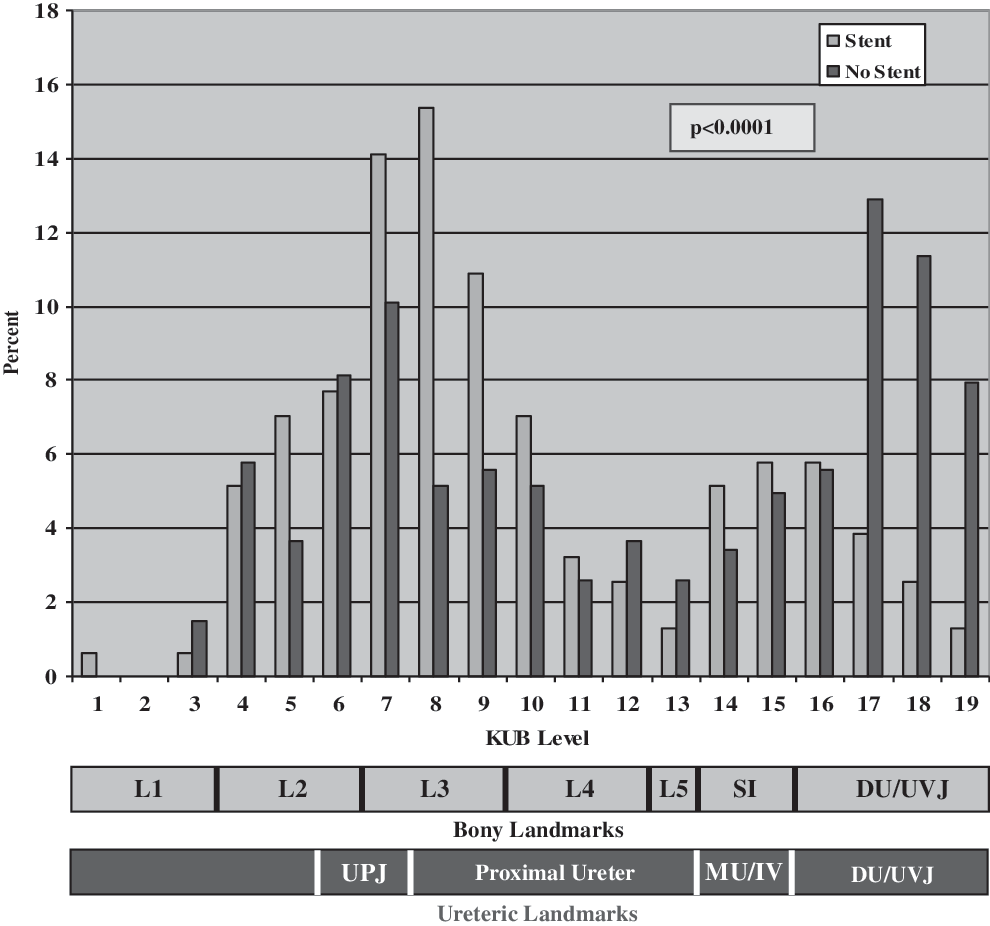
Effect of ureteral stent insertion on stone distribution. KUB=kidneys-ureters-bladder; UPJ=ureteropelvic junction; MU=midureter; IV=iliac vessels; DU=distal ureter; UVJ=ureterovesical junction.
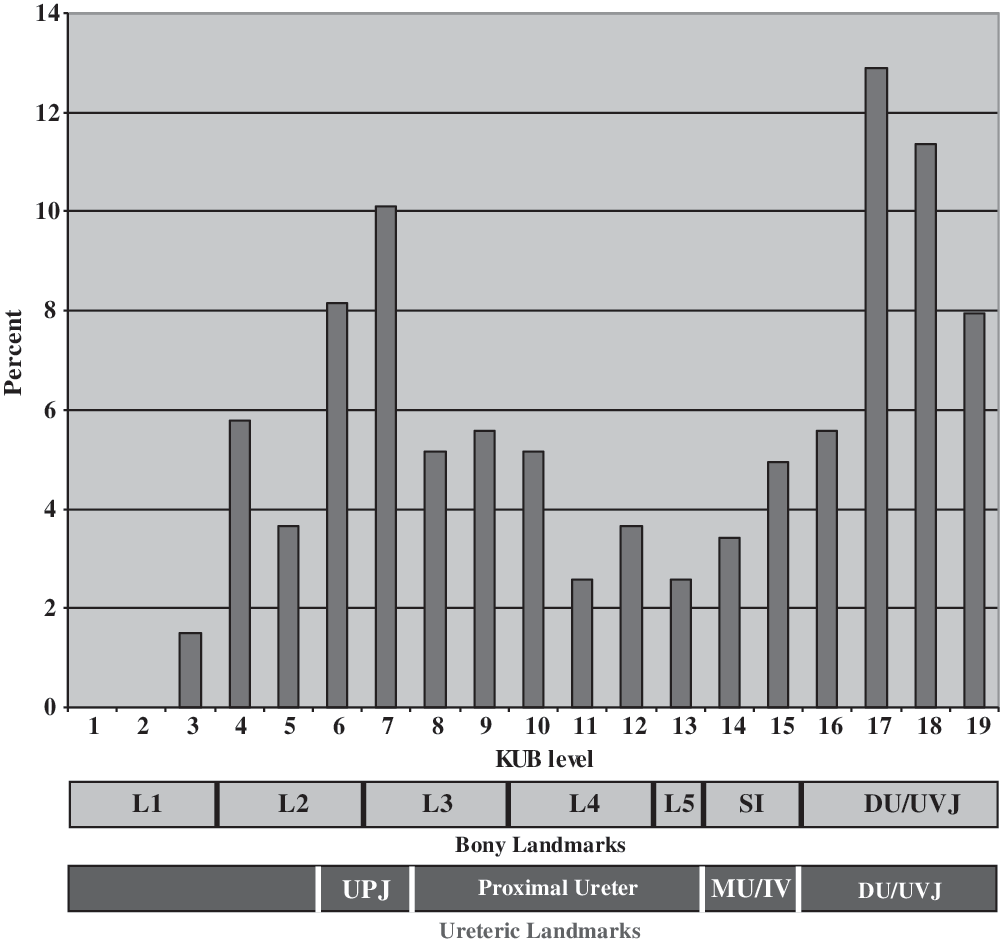
Histogram of stone location distribution in the non-stented patients (n=466). KUB=kidneys-ureters-bladder; UPJ=ureteropelvic junction; MU=midureter; IV=iliac vessels; DU=distal ureter; UVJ=ureterovesical junction.
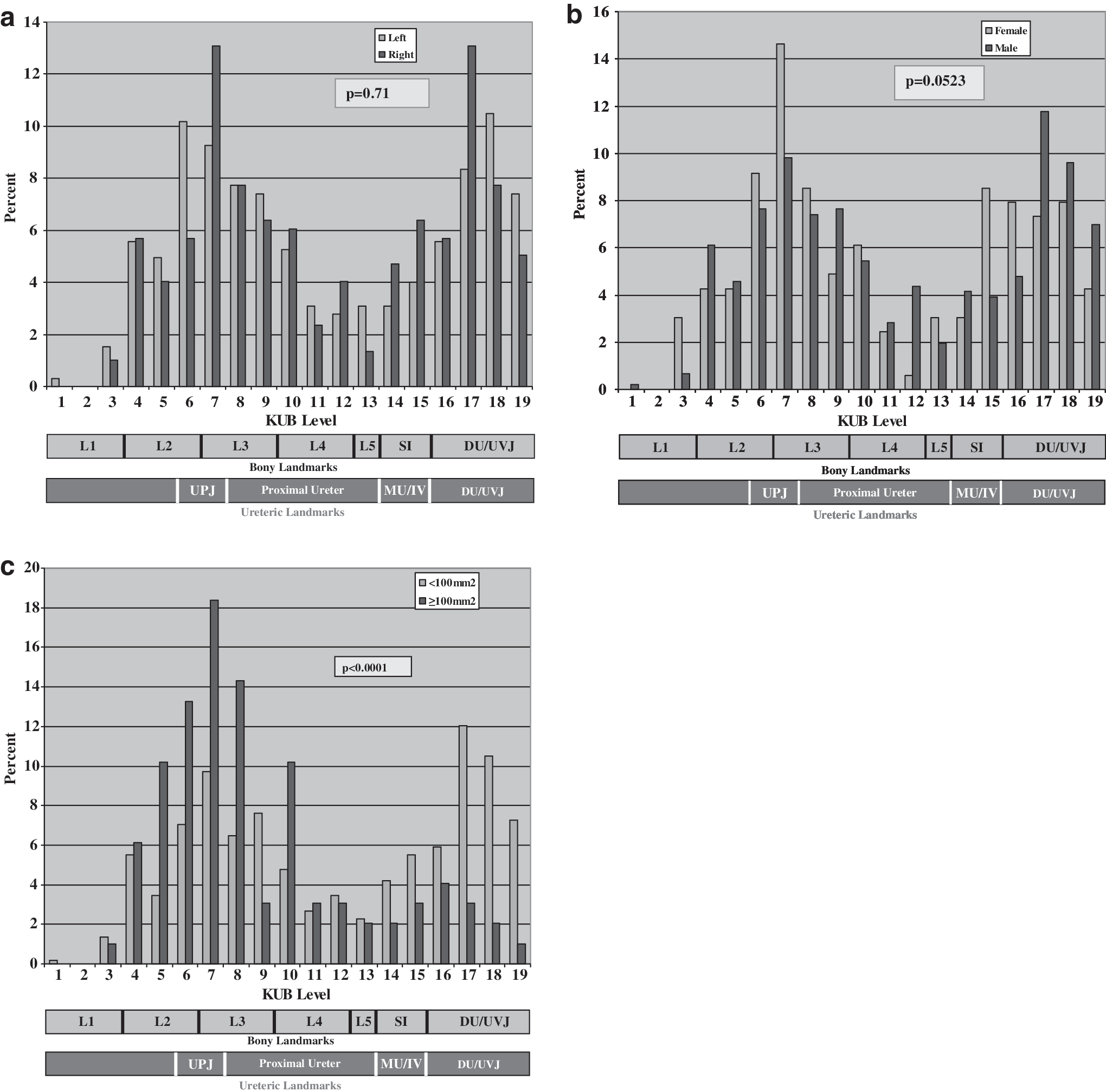
Again, given the significant shift in stone distribution proximally, caused in part at least by the stent insertion itself, in addition to the greater likelihood of a stent in female patients and in patients with large stones (≥100 mm2), the remainder of the statistical analysis, assessing the effect of sex, stone side and size on stone location, was performed using only the cohort of patients without a stent to avoid any confounding related to the stent insertion. Stratification by stone side had no effect on stone distribution with peaks in the region of the UPJ/proximal ureter and intramural ureter/UVJ demonstrated on both sides (Fig. 7a). Comparison of the distribution of stone location between sexes showed a difference that approached significance (P=0.0523). Figure 7b shows the histogram for stone location stratified by sex. There is a greater peak for stones lodging in the distal ureter/UVJ in men vs women and in the proximal ureter/UPJ in women compared with men. As would be expected, stratification of stones by size (<100 mm2 vs ≥100 mm2) showed a statistically significant difference (P<0.0001) in distribution of stone location, with larger stones (≥100 mm2) located more proximally (Fig. 7c).
Discussion
While it has long been taught and is widely reported that three anatomic narrowings exist in the ureter at which stones lodge, 1,3 –6 there is surprisingly no evidence in the literature to support this. It has not been our experience in treating patients with kidney stone disease over many years that stones lodge at the level of the iliac vessels. In this retrospective cohort study of patients presenting for SWL of solitary ureteral calculi, we were able to demonstrate two peaks in the distribution of stones along the course of the ureter. The most cephalad peak occurred adjacent to the lower border of the L2 vertebrae and the upper border of the L3 vertebrae corresponding with the UPJ and upper ureter. The more caudad peak occurred at the level of the intramural ureter and just above the ischial spines at the level associated with the UVJ. This does not support the traditional dogma suggesting a peak in stone distribution over the iliac vessels.
After our initial report in 2007, 8 the same hypothesis was tested in a recently published study by Eisner and associates, 11 who found similar results. They identified the position of the stone in the ureter when patients first presented to the emergency department with colic. This was a retrospective review of 94 consecutive patients who presented to the emergency department with renal colic and were found on CT scan to have a single unilateral renal calculus. Review of these CT scans revealed that at presentation with colic, most stones were either at the UVJ or in the proximal ureter. One drawback to the assessment of stone location based on imaging at the time of initial presentation is that this may not represent the true location where the stone will ultimately lodge. Instead, this may simply represent the location of the stone at one point in time, and a peak in stone location distribution may be missed, because the stones have not had time to migrate to their final location. Presumably, large and medium stones will initially be held up at the UPJ, while smaller stones will make it all the way down to the UVJ before causing significant colic, as was demonstrated by this study. Assuming with time that many of the medium sized stones will migrate beyond to the UPJ, however, and according to traditional teaching then potentially lodge somewhere along the course of the midureter near the iliac vessels, this peak would be missed by examining only the initial acute renal colic presentation.
By reviewing imaging of patients referred for SWL, we are examining a cohort of persons who have failed to pass their stone spontaneously. We think that this cohort better represents the anatomic location where stones do become lodged in the ureter, because the majority of stones will have migrated to their final location in the ureter.
In 74 patients within our cohort, we were able to correlate the findings of pretreatment CT scans with the KUB radiography to determine the most common location of the UPJ, ureteral crossing of the iliac vessels, and the UVJ. The UPJ was found to most commonly lie at the level of the lower border of L2 on the left and the upper border of L3 on the right, which is consistent with the literature. 6 We found the UVJ to be most commonly located just above the ischial spines, which is also similar to previous published reports. 12 This allows us the confidence to suggest that the peaks in stone distribution found on the assigned KUB levels do, in fact, correspond with the UPJ or proximal ureter and UVJ, respectively.
Our study is limited by the fact that we are determining the stone location not from axial imaging on CT, but instead by plain radiography. Unfortunately, the reason is that the majority of patients referred to our center for SWL will have undergone a workup, including a noncontrast CT, outside of our institution and therefore these CT scans are not available for later review. With axial imaging, the exact stone location with respect to the UPJ, iliac vessels, and UVJ in each patient could have been determined rather than relying on the most common location of these sites based on 74 patients from within our cohort, as we did in this study. That being said, we were successful at identifying a clustering of stones in our cohort at the same locations where the UPJ and UVJ were found to be located in the subset of our population with CT scans. Therefore, we believe it is reasonable to conclude, when considering the entire cohort, that the two peaks in stone distribution detected are, in fact, associated with the UPJ and UVJ. More importantly, we do not see any peak in distribution across the two KUB levels that span the midureter. Therefore, regardless of exactly where the ureteral crossing of the iliac vessels occurs in each patient, we do not see a clustering of stones in this area.
A second limitation is that we did not exclude patients with a history of stone disease or previous ureteroscopy. The large sample size of patients reviewed, however, minimizes the likelihood that a bias in stone location would have been introduced as a result of stricture from previous stone disease or instrumentation.
Last, by examining patients referred for SWL, there is the potential for selection bias in our study sample, whereby patients with midureteral stone are not referred for SWL but instead treated with URS. Very commonly, distal ureteral stones are managed endoscopically, but nevertheless a large peak in stone distribution is seen in our series within the distal ureter.
Conclusion
In our retrospective cohort review of patients undergoing SWL, we identified two peaks in stone distribution corresponding to the UPJ/proximal ureter and intramural ureter/UVJ, but were unable to demonstrate a peak in stone distribution at the level of the iliac vessels. Our findings fail to support the traditional teaching that stones tend to lodge at three locations in the ureter.
Footnotes
Disclosure Statement
No competing financial interests exist.