
Abstract
Purpose:
Development and full validation of a laparoscopic training program for stepwise learning of a reproducible application of a standardized laparoscopic anastomosis technique and integration into the clinical course.
Materials and Methods:
The training of vesicourethral anastomosis (VUA) was divided into six simple standardized steps. To fix the objective criteria, four experienced surgeons performed the stepwise training protocol. Thirty-eight participants with no previous laparoscopic experience were investigated in their training performance. The times needed to manage each training step and the total training time were recorded. The integration into the clinical course was investigated. The training results and the corresponding steps during laparoscopic radical prostatectomy (LRP) were analyzed. Data analysis of corresponding operating room (OR) sections of 793 LRP was performed. Based on the validity, criteria were determined.
Results:
In the laboratory section, a significant reduction of OR time for every step was seen in all participants. Coordination: 62%; longitudinal incision: 52%; inverted U-shape incision: 43%; plexus: 47%. Anastomosis catheter model: 38%. VUA: 38%. The laboratory section required a total time of 29 hours (minimum: 16 hours; maximum: 42 hours). All participants had shorter execution times in the laboratory than under real conditions. The best match was found within the VUA model. To perform an anastomosis under real conditions, 25% more time was needed. By using the training protocol, the performance of the VUA is comparable to that of an surgeon with experience of about 50 laparoscopic VUA. Data analysis proved content, construct, and prognostic validity.
Conclusions:
The use of stepwise training approaches enables a surgeon to learn and reproduce complex reconstructive surgical tasks: eg, the VUA in a safe environment. The validity of the designed system is given at all levels and should be used as a standard in the clinical surgical training in laparoscopic reconstructive urology.
Introduction
Despite the introduction of various training models, there are until now no established training standards in urologic reconstructive laparoscopic techniques, although even in beginners' hands, we have to guarantee the required quality of the surgical intervention. The concept of this study was to establish a stepwise training protocol of reconstructive laparoscopic techniques (ie, vesicourethral anastomosis [VUA]) and to analyze the validity of the system and its transferability in real life surgery (transfer validity).
Materials and Methods
Concept of a new laparoscopic training program
The development of a standardized approach for laparoscopic training has to include the well-known principles of reconstructive laparoscopy as well as the ideal simulation of the required surgical technique in a realistic physical environment. The main factors are the limited intracorporeal space, the lack of three-dimensional vision, and the handling of laparoscopic instruments. We developed a standardized stepwise training protocol to learn the basic techniques needed for complex laparoscopic reconstructive procedures in a safe environment. 4,6,7
To bridge the gap between laboratory use and real surgery, specific requirements concerning the individual training models had to be determined. The training models had to meet exactly the definitions of the face validity (Table 1). So we linked the laboratory part with the surgical part by analyzing the different reconstructive steps of laparoscopic radical prostatectomy (LRP) and translated them into basic suturing techniques applied on animal models in the pelvi-box trainer (Tables 1 and 2). 6
PLND=pelvic lymph node dissection; NVB=neurovascular bundle.
The study variables had to meet exactly the definitions of construct validity. In our training course, we chose time and mentor judged quality of the suturing as variables to discriminate between experienced surgeons and novices.
To assess the practical applicability of our training program, we analyzed the predictive validity. This allows a statement of the transfer of the training program in future clinical application (Fig. 1).
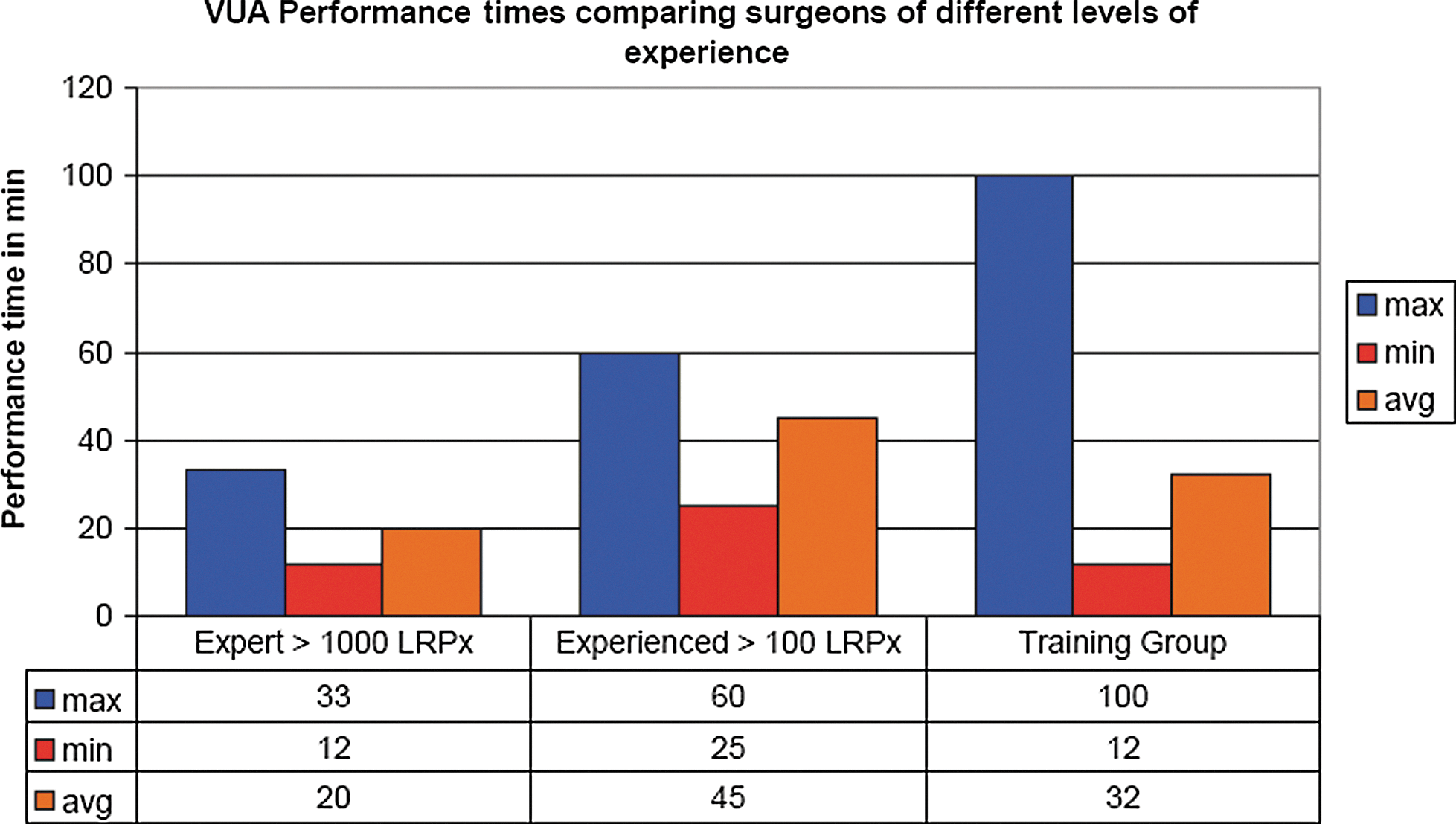
Comparing intraoperative vesicourethral anastomotic suturing times of surgeons of different levels of experience with those of the training group. LRP=laparoscopic radical prostatectomy.
Study population
Thirty-eight urologists who were novices or beginners with a low experience level of laparoscopic reconstructive surgery techniques were included in the study. Four very experienced laparoscopists (RJ, SO, FT, TD) performing the stepwise pelvi trainer tasks set the baseline for the training time per exercise.
Operative technique
The laboratory part of the study included the standardized six-step training protocol in the pelvi trainer box (Table 1). The surgical part of the study included the corresponding operative steps in LRP (Table 2).
To standardize the operative technique, an analysis of the suturing technique of every step of the protocol was performed including the definition of the direction of the stitches and the preferred angle between the needle and the needleholder (eg, Task 2: suture technique to close the vertical incision using the chicken leg model; left directed righthanded forehand stitches angle: 90 degrees). This technique was exactly transferred in the surgical setting. The participants performed the whole laboratory training protocol while the times needed for each exercise were recorded. The quality of the task performance was supervised by an experienced laparoscopist. After successfully finishing the laboratory part, the participants took part in the surgical part under direct supervision of a experienced laparoscopist. The performance times of each correspondent step of the surgery were recorded.
Results
Content validity
To prove the content validity of our training model, the correlation between the steps of the pelvi training protocol and the steps of the surgery (laparoscopic prostatectomy) was analyzed. The surgical procedure was divided into 10 parts. Three parts of the surgical procedure fit the best to our training modalities. By comparing the training models with the surgical sections, a clear correlationship between the rising level of difficulty in the surgical technique and handling of the instruments can be shown. As expected, the model of the VUA showed the best concordance between model and surgery (Tables 1 and 2). The content validity between the model and the surgical steps is given in three sections: (1) VUA (Exercise 6); (2) ligation of the plexus Santorini (Exercise 4); (3) dissection of the endopelvic fascia and backflow ligation (Exercise 3). The other parts of the training protocol can be seen as preliminary practice.
Construct validity
To analyze the construct validity, we divided the group of 38 laparoscopic novice participants and 4 experts according to their laparoscopic experience level (LEL) (Table 3). Based hereon, we compared the groups and analyzed the training behavior. For statistical analysis, the Wilcox rank sum test for two-sided issues was used (α=0.01).
LEL=laparoscopic experience level; PLND=pelvic lymph node dissection; RLND=retroperitoneal lymph node dissection.
There was no significant difference between the group of previous minimal laparoscopic ablative skills (LEL 2a) and the group of no previous laparoscopic skills (LEL 1) (Table 4). This means previous laparoscopic ablative techniques do not help very much when performing intracorporeal suturing techniques. Comparing the expert group with the novice group, there is significant evidence that the expert group performs much better (Table 5). Conclusively, construct validity of the concept is proven.
LEL=laparoscopic experience level.
LEL=laparoscopic experioence level; VUA=vesicourethral anastomosis.
Predictive validity
To analyze the predictive validity of the training program, we correlated the training times on the pelvi trainer box with the times the participants needed in the surgical part. For statistical analysis, the Wilcoxon rank sum test for two-sided issues was used (α=0.01) (Table 6).
Task 3: U-shape incision chicken leg model; EPF=incision of the endopelvic fascia. Task 4: plexus Santorini chicken leg model; DVC=dorsal vein complex. Task 6: vesivourethral anastomosis pig bladder model.
Between the laboratory and surgery results of the three best corresponding tasks was a significant difference. The results in the pelvi trainer represent a task performed in an ideal environment without being disturbed by bleeding or worsening of the vision because of getting the telescope tip dirty. The essential step of the training program (VUA) showed the best concordance with a 25% plus in time when working in the real environment. In summary, there is a clear correlation between the laboratory times and the operating room times. The reson for the slightly better times in the laboratory training setting is the ideal training environment with less disturbing factors. The predictive validity according the training protocol is given.
Ranking of training benefits
To rank the benefit of the stepwise laparoscopic training protocol, we analyzed the time needed to perform the VUA (Fig. 1):
(1) For a very experienced laparoscopist with >1000 radical prostatectomies
(2) For an experienced laparoscopist with >50 radical prostatectomies
(3) For the group of novice laparoscopists after performing the training protocol
Comparing the three groups, an obvious trend can be seen: After passing the training protocol, the time-consuming performance of laparoscopic VUA can be significantly reduced (novice after training: mean 32 min; max 100 min; min 12 min) to a level of an experienced laparoscopist (mean 45 min; max: 60 min, min: 25 min) but without reaching the level of an expert (mean: 20 min, max 33 min; min 12 min). This shows clearly the benefit for both—the trainee and the patient—because a realistic training simulation reduces intraoperative time needed to perform advanced reconstructive surgical steps. The graph also shows the limitations of preoperative dry-laboratory preparation; eg, anastomotic time, 100 minutes, reflects a very difficult case that is not comparable to the training setting (very limited intracorporeal space or a very short urethral stump). The comparison also shows that reaching the expert level demands a lot more experience than pelvi-box training can offer.
Discussion
More than 15 years after the first performance of an LRP, it is now a well-established and standardized procedure that is regularly performed in laparoscopic high-volume centers. The success of the technically demanding procedure was achieved by a standardized approach. The limitations of the procedure lie in the distinctive learning curve that limits its widespread use. To overcome intraoperative problems and to shorten the learning curve, pelvi-box training was established. Until now a various number of different training models to perform VUA laparoscopically in a mechanical simulator have been published (Table 7). The different working groups show the feasibility to mimic the surgical technique even under spatial limitations. In all different models, a tubular structure (urethra model) is realigned to a bladder neck model using exactly the armamentarium and material that is also used in the operating room, and the whole procedure is performed under realistic physical conditions. The content validity is proven in all predescribed models. 2,4,8 –11
In about 50% of the described training models, the construct validity was shown—therefore, a significant difference between very experienced and not experienced groups of participants has been detected. In our study, marginal differences according to the previous level of experience between the training groups (no experience LEL 1 vs low experience with easy laparoscopic ablative techniques LEL 2a) were not detected. A significant difference between the expertgroup (LEL 4b) and the whole training group (LEL 1 and LEL 2a), however, was clearly shown. This result was expected, because easy ablative techniques do not require knowledge and abilities in intracorporeal suturing.
A complete evaluation of a mechanical simulator reconstructive training program with an adaequate number of trainees consisting of a dry laboratory part and a linked surgical part including the transfer to the operating room (Fig. 2) has not been published yet.
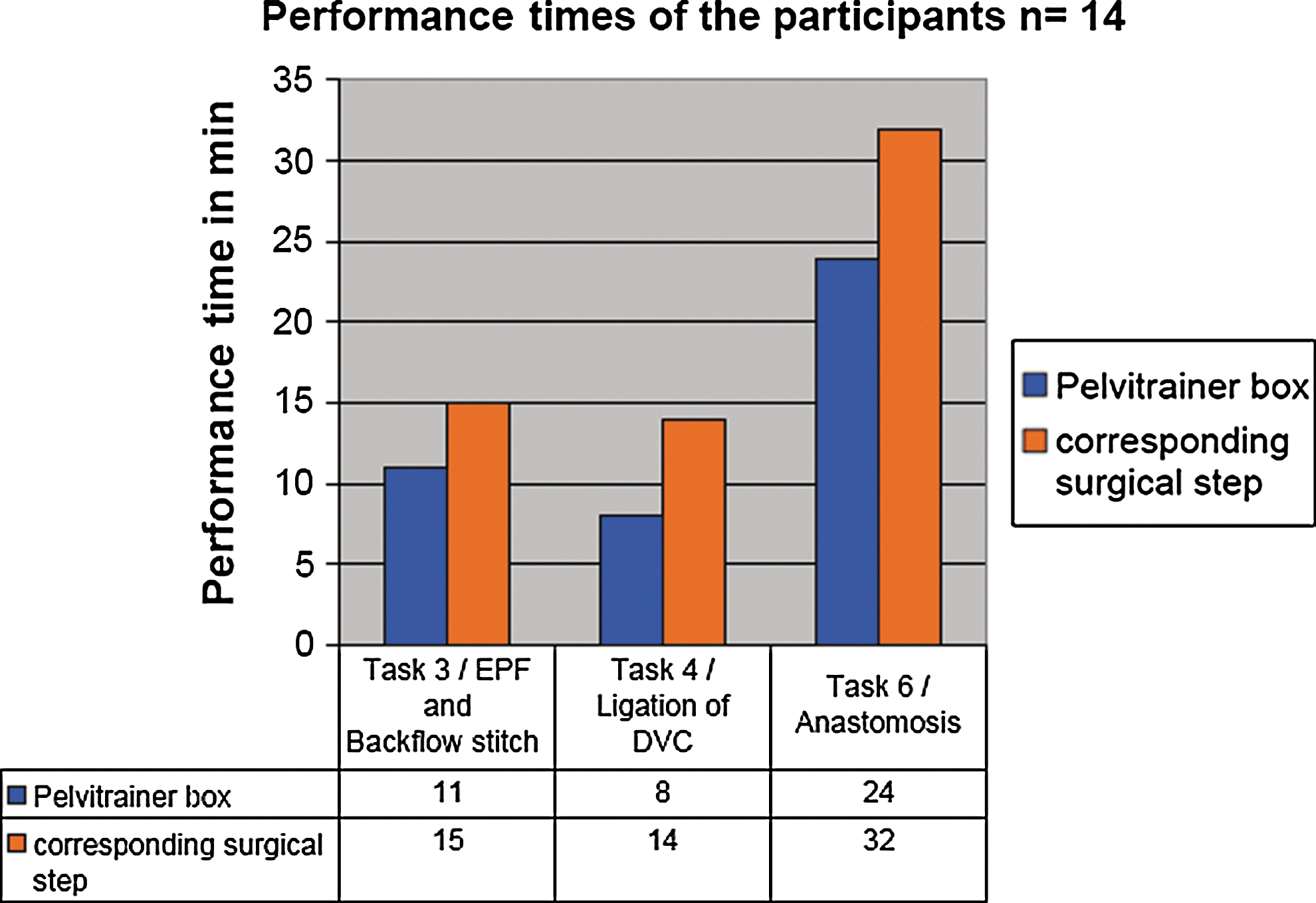
Performance times of the trainees in the dry laboratory (blue) vs operating room times (orange). Task 3=U-shape incision chicken leg model; EPF=incision of the endopelvic fascia. Task 4=plexus Santorini chicken leg model; DVC=dorsal vein complex. Task 6=vesicourethral anastomosis pig bladder model.
Why did we choose a mechanical simulator? The published data about the transferability of surgical skills acquired in virtual reality surgical simulator (VRSS) settings linked with the real surgical performance of a cholecystectomy in a swine model (ablative technique) was not encouraging. The da Cruz working group could not demonstrate that VRSS training resulted in an improved surgical performance. 12 –14 One reason could be the lack of real physics (simulated haptic feedback, simulated physical behavior of instruments) in VRSS that are, though progressing, still far from realistic handling of real tissue and laparoscopic instruments. Mechanical simulators using the same physical settings as they are in the operative field still play the major role in laparoscopic surgical training. Another benefit of mechanical simulators lies in the possibility to adapt the task to the needs of the trainee. A difficult task—eg, the VUA —can be divided into multiple easy steps without the need to update the software of the simulator. 15,16
The consensus of a number of studies shows the necessity to standardize urologic training protocols. This study shows how clinical laparoscopy training can be easily organized, standardized, practiced, and transferred in the operating room.
Conclusion
The standardized six-step training program enables the participant to learn difficult reconstructive surgical techniques—eg, the VUA—in a safe environment. Once the technique is learned, a transfer in the operating room is possible and can be applied with the routine of a advanced laparoscopist. The validity criteria of the training concept are proven. The program can be used as a standardized tool in the clinical surgical training of reconstructive laparoscopic surgery in urology.
Footnotes
Disclosure Statement
No competing financial interests exist.