
Abstract
Background and Purpose:
Topical chemotherapy for urothelial cancer is dependent on adequate contact time of the chemotherapeutic agent with the urothelium. To date, there has not been a reliable method of maintaining this contact for renal or ureteral urothelial carcinoma. We evaluated the safety and feasibility of using a reverse thermosensitive polymer to improve dwell times of mitomycin C (MMC) in the upper tract.
Materials and Methods:
Using a porcine model, four animals were treated ureteroscopically with both upper urinary tracts receiving MMC mixed with iodinated contrast. One additional animal received MMC percutaneously. The treatment side had ureteral outflow blocked with a reverse thermosensitive polymer plug. MMC dwell time was monitored fluoroscopically and intrarenal pressures measured. Two animals were euthanized immediately, and three animals were euthanized 5 days afterward.
Results:
In control kidneys, drainage occurred at a mean of 5.3±0.58 minutes. Intrarenal pressures stayed fairly stable: 9.7±14.0 cm H20. In treatment kidneys, dwell time was extended to 60 minutes, when the polymer was washed out. Intrarenal pressures in the treatment kidneys peaked at 75.0±14.7 cm H20 and reached steady state at 60 cm H20. Pressures normalized after washout of the polymer with cool saline. Average washout time was 11.8±9.6 minutes. No histopathologic differences were seen between the control and treatment kidneys, or with immediate compared with delayed euthanasia.
Conclusions:
A reverse thermosensitive polymer can retain MMC in the upper urinary tract and appears to be safe from our examination of intrarenal pressures and histopathology. This technique may improve the efficacy of topical chemotherapy in the management of upper tract urothelial carcinoma.
Introduction
Materials and Methods
After obtaining Institutional Animal Care & Use Committee approval, five female juvenile farm pigs, ranging from 37 to 41 kg, underwent bilateral endourologic procedures (Table 1).
URS=ureteroscopy; PCN=percutaneous nephrostomy; perf=perforation.
After induction of general anesthesia, the pig was positioned prone. Both ureters were cannulated with a guidewire and a 6F open-ended ureteral catheter. A Foley catheter was placed to gravity drainage. Retrograde pyelography confirmed that the ureteral catheters were at the level of the renal pelvis and contrast was allowed to clear before instillation of MMC.
MMC (VWR, Radnor, PA) was reconstituted in sterile water and filtered for sterility using a 0.2 micron PES membrane filter (Millipore, Billerica, MA). MMC, stored at 4°C, was mixed with room temperature Isovue-300 contrast immediately before injection, for a final concentration of 20 mg MMC and 50% contrast. Total volume was 10 mL. On the control side, this mixture was injected into the renal pelvis via urethral catheter. Pressure measurements were taken with a digital manometer (Dwyer Instruments Inc, Series 477A, Michigan City, IN). With an 8F pediatric urodynamic catheter, the system was zeroed in comparison with rectal pressure. By connecting the ureteral catheter to the manometer, the catheter was effectively clamped. Intrarenal pressure (IRP) measurements and fluoroscopic images were taken immediately before instillation of MMC and contrast and at regular intervals until fluoroscopic clearance of the MMC and contrast.
On the experimental side, semirigid ureteroscopy was performed after ureteral catheterization. With the ureteroscope in the distal ureter, 5 mL of RTP was injected via a 3F injection catheter, which was then removed. The 6F ureteral catheter with its tip in the renal pelvis remained, and MMC and contrast was instilled (Fig. 1). Fluoroscopic images and IRP measurements were taken before placement of RTP and at regular intervals after instillation of MMC and contrast. After 60 minutes, if there was MMC and contrast remaining in the collecting system, RTP was dissolved. RTP is viscous at body temperature and a liquid below 16°C, so injection of room temperature saline through the ureteral catheter changed it to liquid. 8 Data were analyzed with JMP version 9.0, SAS® Inc (Cary, NC).

Schematic of experimental design.
Two of the animals were selected a priori for immediate euthanasia after completion of their procedures, and the other animals were sacrificed 5 days later. Intravenous pyelography (IVP) was performed to evaluate for postprocedural obstruction immediately before euthanasia on day 5.
In one animal, MMC and contrast was administered bilaterally via a 16F Councill catheter placed percutaneously in the renal pelvis. RTP was instilled in the ureter as described above on the treatment side. The animal was euthanized after 5 days.
Histopathology
After euthanasia, kidneys and ureters were removed through a midline laparotomy, fixed in 10% formalin, and hemisected and photographed. For each kidney, ≥80% of the renal pelvis derived from a central slice was submitted for microscopic examination. The attached ureter was divided into proximal, midproximal, middistal, and distal fourths. Each segment was cross-sectioned and submitted separately in toto. Sections were prepared and stained with hematoxylin and eosin. A single histopathologist preparing and examining the specimens was blinded to the procedures and designation of treatment and control arms.
Results
RTP was successfully deployed in the distal ureter in all animals without complications. Ureteral perforation occurred in one control and urethral perforation in another animal (Table 1). No animals experienced any postoperative complications.
For controls, drainage of MMC and contrast occurred at a mean of 5.3±0.58 minutes. We were unable to obtain a drainage time for Pig A's control, because of ureteral perforation. With the experimental kidneys, RTP occluded the ureter with no appreciable MMC and contrast drainage after 60 minutes (Fig. 2). Room temperature saline was used to wash out the RTP. After dissolution of RTP, average washout time was 11.8±9.6 minutes. In the pigs that received IVPs before euthanasia on day 5, interpretation was limited by bowel gas. Drainage, however, appeared to occur by 10 minutes.
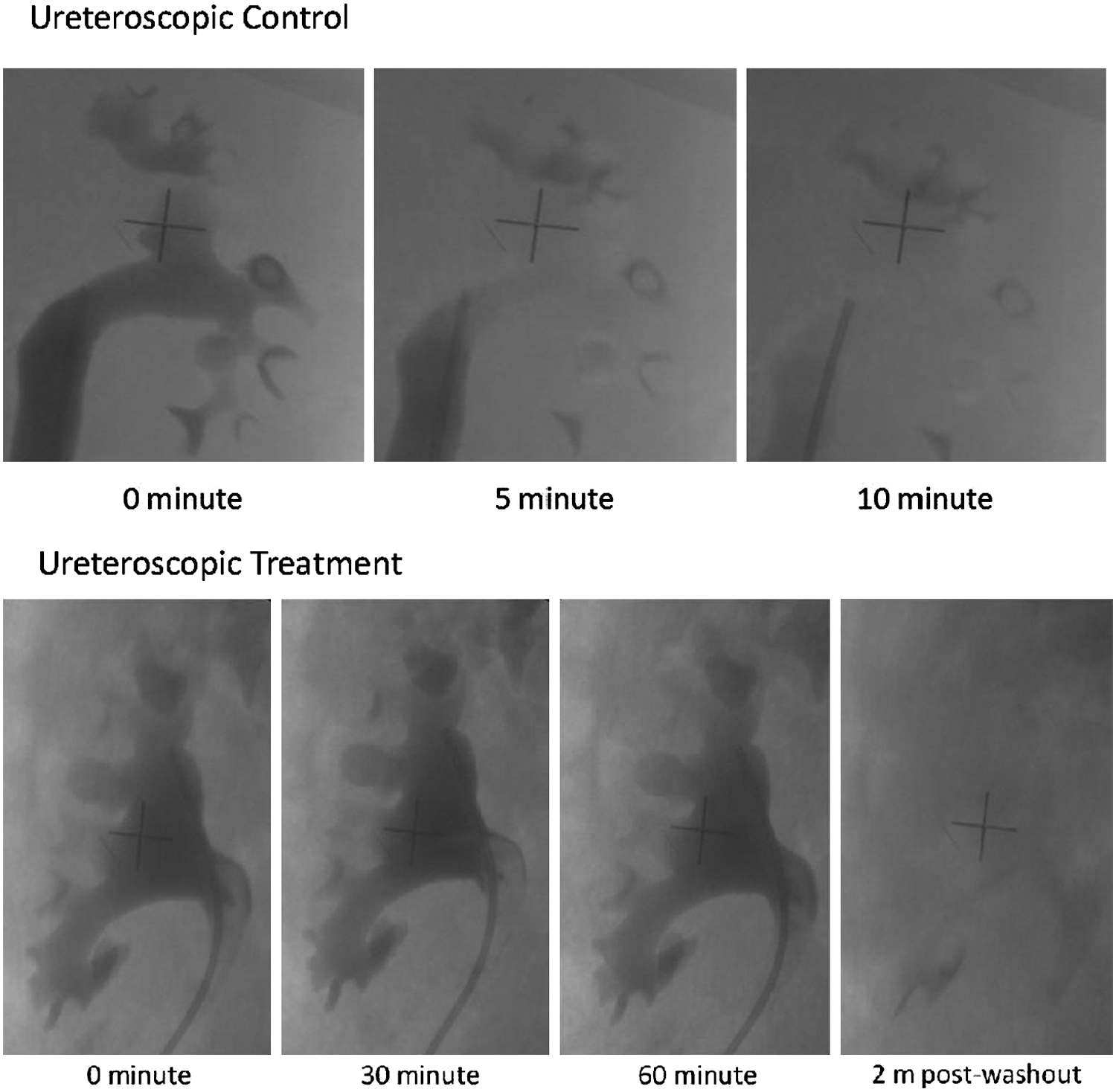
Fluoroscopic images confirming drainage of mitomycin C and contrast.
For controls, IRPs stayed fairly stable at an average of 9.7±14.0 cm H20. For the experimental side with RTP instillation, IRPs rose to a maximum mean pressure of 75.0±14.7 cm H20 at 30 seconds post-RTP instillation and stayed fairly constant at approximately 60 cm H20 until washout occurred at 60 minutes. After washout, the pressure dropped to a mean of 21.9±18.5 cm H20 in 5 minutes (Fig. 3).
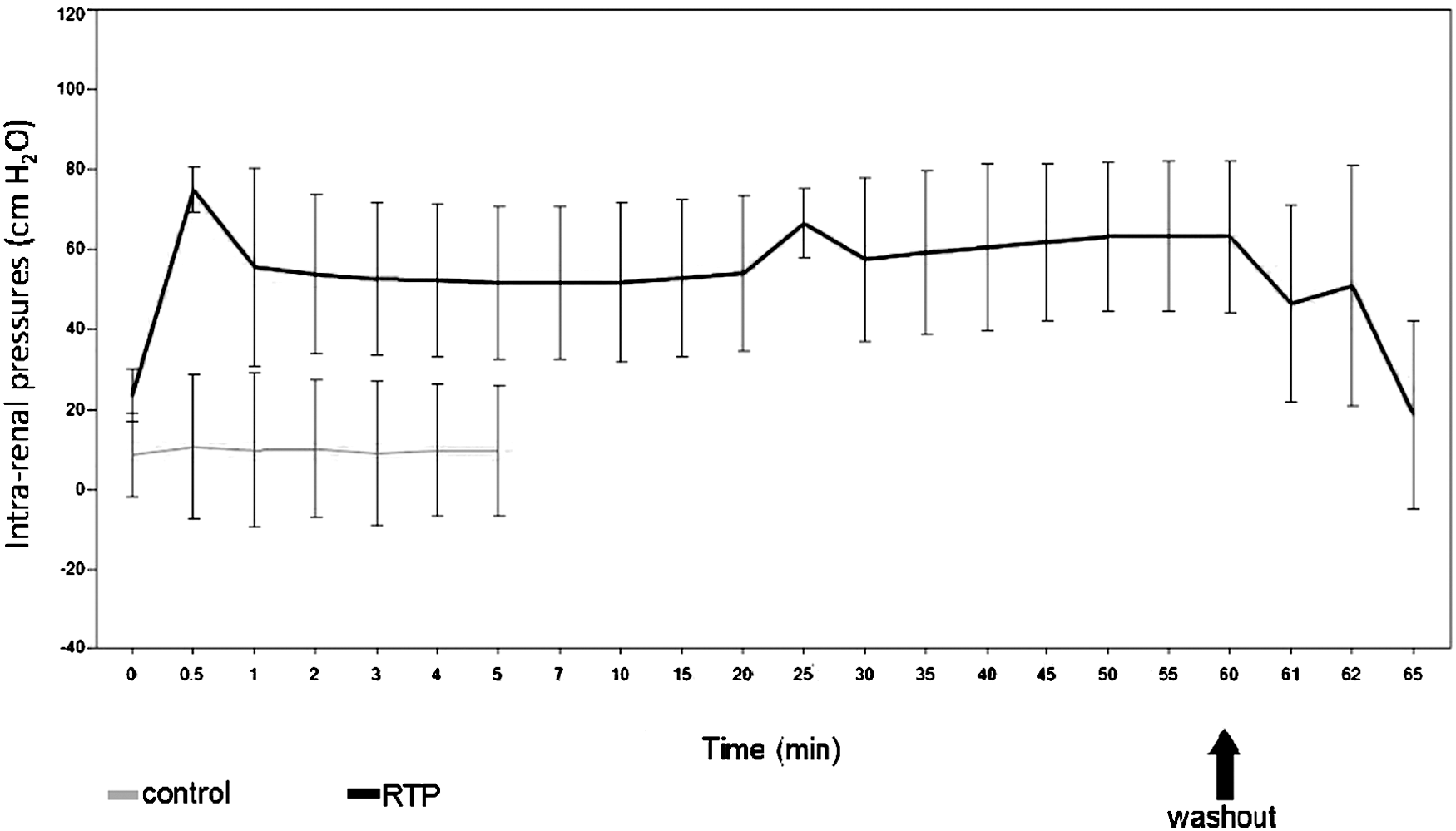
Comparison of intrarenal pressures between experimental and control kidneys.
In the animal that underwent percutaneous access and antegrade instillation of MMC and contrast, drainage occurred on the control side in 20 minutes. With RTP instilled ureteroscopically, drainage of MMC and contrast occurred in 40 minutes.
Histopathology
Slides from each specimen were reviewed and compared qualitatively for urothelial alterations, inflammation, edema, necrosis, tubular dilation, or other features. No systematic differences in any of these parameters were noted between the control and experimental kidneys in all animals (Fig. 4).
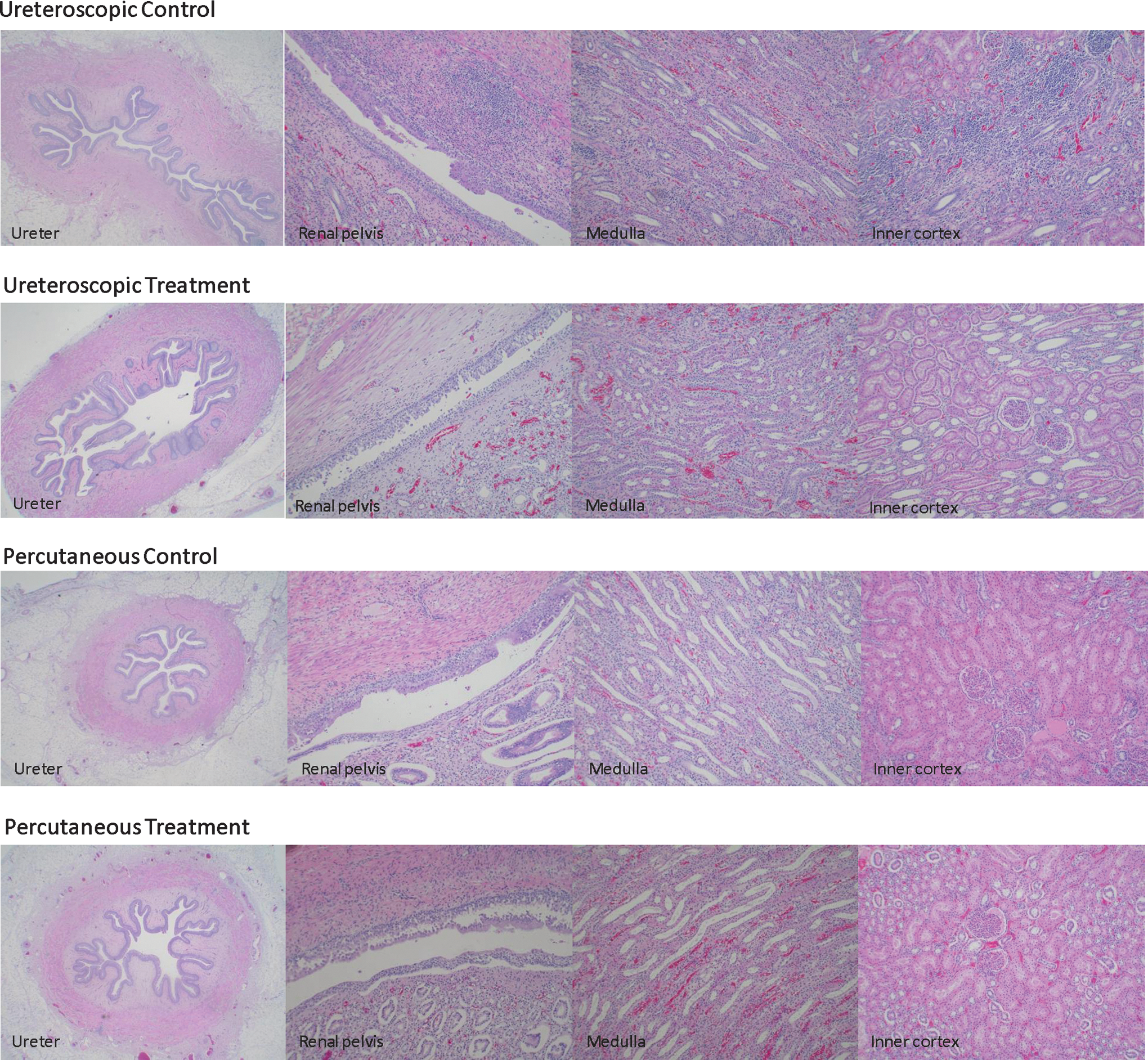
Histopathology. No differences in urothelial alterations, inflammation, edema, necrosis, tubular dilation, or other features.
Discussion
The first endoscopic treatment of UUC was described by Huffman and associates 9 and applied to patients with a solitary kidney as well as patients with functioning contralateral kidneys. Both ureteroscopic and percutaneous approaches have been used for tumor ablation and chemotherapy instillation. 2 –5,10,11
In bladder cancer, a single dose of MMC (40 mg of MMC mixed in 40 mL H2O and kept in the bladder for 60 minutes) post-transurethral resection of bladder tumor (TURBT) decreased the risk of recurrence by approximately 48% from 82% to 42% over 2 years of follow-up, P<0.001. 12 A meta-analysis of randomized trials with patients receiving one post-TURBT dose of epirubicin, MMC, thiotepa, or pirarubicin also established a lower risk of recurrence. 1
MMC has been used after endoscopic treatment of UUC and instilled via nephrostomy tube, open-ended ureteral catheter, or intravesically with a Double-J stent. Despite this, recurrence rates range from 29% to 54%. 2,4 –6 We hypothesized that a reverse thermosensitive polymer may increase dwell time of chemotherapy in the upper tract and thereby decrease recurrence. We describe the initial report of using RTP to increase upper tract dwell times of a chemotherapeutic agent. We achieved a dwell time of 60 minutes to match typical bladder instillation times, but RTP has been shown to dissolve in human urine after 116.5±31.0 minutes at 37°C. 13
BackStop Gel is a stimuli-responsive polymer with inverse thermosensitivity. At body temperature in the urinary tract, it is solid. Below body temperature, it is a liquid, allowing its injection while cool and dissolution when flushed with cool irrigation. It belongs to a class of nonionic surfactants known as pluronics, or triblock copolymers of polyethylene oxidea–polypropylene oxideb–polyethylene oxidea. 14 Specifically, BackStop consists of copolymers 188 and 407. It is currently used clinically to decrease stone retropulsion during ureteroscopic stone fragmentation and was approved for this indication by the Food and Drug Administration in 2009. 8
RTP's ability to completely occlude the ureter and prevent stone migration appears to translate well to increase MMC dwell time. We chose to investigate an ureteroscopic model, because this is the least invasive method of endoscopic treatment of UUC. Because larger tumors in the kidney may need to be approached percutaneously, we selected one animal to demonstrate that RTP can also increase dwell time with antegrade instillation of MMC. Dwell time may have been shortened by the presence of leakage around the nephrostomy tube, because the MMC drained in 40 minutes compared with the lack of ureteroscopic drainage at 60 minutes.
By increasing dwell time with RTP, we also introduced a period of acute urinary obstruction. We demonstrate that IRP was highest at initial instillation at a mean pressure of 75 cm H20, but pressures stayed at approximately 60 cm H20 until washout. There was no evidence of pyelovenous backflow, which has been cited to occur in humans at 110 to 136 cm H20. 15 In addition, mean renal pelvis pressures of 128 cm H20 have been described in flexible ureteroscopy without the use of an access sheath. 16 Overall, renal pressures do not appear to be excessive with RTP-induced obstruction during our porcine experiments.
Histopathologically, MMC caused an equal degree of inflammation in animals that received MMC with RTP and those that received MMC without RTP. This suggests that there is no additional impact from RTP or from the temporary ureteral occlusion it induces. Another porcine ureteroscopic study of BackStop instillation for management of ureteral calculi also found no histologic changes in animals immediately euthanized and those euthanized 1 week later. 13 In addition, there were no differences between the animals euthanized immediately and those euthanized 5 days postprocedure. MMC-induced changes may not resolve in 5 days, because studies in rat bladders have shown persistent fibrosis and inflammation 30 and 60 days after intravesical MMC instillation. 17
There were several limitations. We had a limited number of animals to study and focused primarily on ureteroscopic intervention, although the animal that underwent percutaneous instillation of MMC did well and had no histologic differences compared with the ureteroscopically treated animals. We did not measure pharmacokinetic data such as serum or urine chemistries, drug levels, nor urinalyses/urine cultures. A previous porcine ureteroscopic study with RTP for stone treatment had shown no increased risk of infection or alterations in chemistries. 13 Also, our animals did not undergo simulation of ureteroscopic ablation of UUC before MMC or RTP administration. Histopathologic changes and absorption may be affected by adding urothelial ablation to the model. Clinically, it seems wise to defer MMC use after endoscopic treatment of UUC if there has been full-thickness injury to the collecting system, corresponding to how MMC is not used in the bladder if there is suspicion of bladder perforation.
Conclusions
Endoscopic management of UUC confers the benefits of renal conservation but has significant recurrence risks. Increasing contact time of topical chemotherapy with the use of a RTP plug could lower recurrence rates. We demonstrate that use of a reverse thermosensitive polymer is feasible to safely increase dwell time to 60 minutes.
Footnotes
Acknowledgments
Many thanks to Stephan Spitzer for preparing ![]() . This study was investigator initiated and supported. Backstop® Gel and injector catheters were provided by Boston Scientific. Gastón M. Astroza was supported by the Endourological Society and Cook Urological. Andreas Neisius was supported by a Ferdinand Eisenberger grant of the Deutsche Gesellschaft für Urologie (German Society of Urology), grant ID NeA1/FE-II.
. This study was investigator initiated and supported. Backstop® Gel and injector catheters were provided by Boston Scientific. Gastón M. Astroza was supported by the Endourological Society and Cook Urological. Andreas Neisius was supported by a Ferdinand Eisenberger grant of the Deutsche Gesellschaft für Urologie (German Society of Urology), grant ID NeA1/FE-II.
Disclosure Statement
Dr. Lipkin is a consultant for Boston Scientific and speaker for Lumenis; Dr. Ferrandino is a proctor for Intuitive Surgical; Dr. Inman has research funding from GlaxoSmithKline. For the remaining authors, no competing financial interests exist.