
Abstract
Background and Purpose:
The feasibility and diagnostic performance of multiparametric magnetic resonance imaging (mp-MRI) has to be proven further. In this study, we evaluate the role of mp-MRI for targeted biopsy of early stage prostate cancer (PCa).
Patients and Methods:
A total 32 consecutive patients with transrectal ultrasonography (TRUS)-guided biopsy-proven PCa meeting low-risk criteria and pursuing active surveillance were selected to undergo mp-MRI 3 Tesla (3T) with endorectal coil. Patients were divided then into three groups based on the method used to target the mp-MRI designated region of interest (ROI): Group 1 underwent TRUS-guided prostate biopsy using an MRI-based coordinate plan (cognitive targeting). Group 2 underwent MRI-targeted TRUS-guided prostate biopsy using MyLabTMTwice, which superimposed the archived MRI images onto the real-time ultrasonography image allowing targeted biopsy of the ROI (fusion targeting). Group 3 included selected patients who had an elevation in prostate-specific antigen levels, or patients followed after radiation therapy (two patients) for suspicious unifocal MRI lesion recurrence. These patients underwent MRI-guided biopsy of the suspicious ROI using the navigation system DynaTRIM.
Results:
The cancer detection rate in group 1 was 33.3% (3 of 10 patients), while in group 2, it was significantly higher at 46.2%. The sensitivity and specificity for group 1 was 45.5% and 33.3%, vs 61.9% and 20.8% in group 2, respectively. The positive predictive value in group 1 was 50.0% vs 53.8% in group 2 (P=0.04). In group 3, the cancer detection rate was much higher (80%) than in group 2, (P=0.005) although the majority of these patients (7 of 10) had a previously diagnosed prostate cancer on TRUS-guided 12-core biopsy.
Conclusion:
Our preliminary experience of mp-MRI suggests the detection of early stage prostate cancer with low-risk features yields potential candidates for active surveillance or focal targeted therapy. The MRI-TRUS fusion system increases diagnostic yield compared with cognitive MRI-directed TRUS-guided biopsy.
Introduction
Engelbrecht and associates 4 analyzed the advances in multimodality MRI/MRIS (MRI spectroscopy). They concluded that higher field MR scanners (3 Tesla [3T]) with improved endorectal coils will provide more sensitive MRI/MRSI images. The addition of other functional MRI parameters such as diffusion weighted imaging (DWI) can reveal changes in tissue microstructure angiogenesis, providing quantitative information (T2 maps, metabolite maps, water apparent diffusion coefficient maps) that, when analyzed together, will provide the necessary sensitivity and specificity needed to safely treat men with low-volume PCa who are candidates for active surveillance or focal therapy. Verma and colleagues 5 presented results of novel multiparametric (mp) MRI 3T with endorectal coil, which provides valuable information that will lead to MRI-targeting of small index tumor lesions for biopsy and ablation purposes. Villers and coworkers 6 evaluated the utility of dynamic contrast enhanced (DCE) MRI for targeted prostate biopsy to detect tumor foci more than 0.5 cc with a sensitivity and specificity of 86% and 94%, respectively.
More recent developments comprise a use of fusion software to superimpose MRI (especially a suspicious region of interest [ROI] for tumor cancer location) with transrectal ultrasonography (TRUS) to perform TRUS-guided, MRI-targeted prostate biopsy. 7,8 Currently, there are many fusion software packages available for clinical approbation including platforms developed by Philips, Eigen, Koelis, Esaote, Hitachi, and others. The targeted TRUS biopsy can potentially reduce inaccuracy of mapping inaccuracy from needle displacement because of deflection or deformation of tissues. A real-time deformable registration of prostate volume with three-dimensional image-based prostate tracking and elastic TRUS/MRI fusion has been proposed with the same intent. The latter approach necessitates histopathologic confirmation of every core, gathering detailed information that, in turn, can be introduced into the mapping software and be used as a guide for targeted therapy. While admittedly more costly, this approach provides additional information both for future research and for guiding treatment decisions regarding individual patients, enabling truly focal therapy that would treat precisely the involved portions of the gland.
Recently, Invivo Corporation introduced a direct MRI-guided biopsy system with promising preliminary results regarding sensitivity and specificity. The Invivo system, however, requires full access to MRI systems and MRI-compatible biopsy equipment, making this approach expensive and unwieldly for radiologists and urologists. Phase I and II studies are under way to evaluate these results.
Missed prostate cancers generally represent a chronic problem for urologists managing the disease, creating uncertainty and emotional stress for patients, and initiating a cascade of repeated testing and biopsies. Reducing the need for repeated biopsies necessitates techniques with a high negative predictive value. In this study, we present our initial experience of different mp-MRI–based techniques for targeted biopsy of the suspicious ROI. Our principal aim was to determine the detection rate of MRI-suggested TRUS-biopsy vs fusion MRI-TRUS–guided biopsy and evaluate the efficiency of MRI-guided biopsy in carefully selected patients who would be potential candidates for focal therapy or active surveillance.
Patients and Methods
Patients
A total 32 consecutive patients with PSA greater than 2 ng/mL and less than 15 ng/mL presented with one or more of the following clinical indications for prostate biopsy: Palpable nodules on DRE or history of negative TRUS-guided prostate biopsy with rising PSA, or positive biopsy with low-risk features managed or considered for management under “active surveillance” protocol. These patients were selected to undergo mp-MRI 3T with endorectal coil. In all 32 patients, ROIs for suspicious lesions were identified on mp-MRI.
Technique
Patients were divided into three groups based on the different techniques used to incorporate the mp-MRI imaging technology into the prostate biopsy procedure.
In both group 1 and group 2, we also performed random biopsies of MRI negative areas of the prostate to evaluate the accuracy (ie, sensitivity and specificity) of the mp-MRI technique.
Diagnostic algorithm
1. The use of mp-MRI (endorectal prostate 3T coil, Signa GE Medical Systems, Milwaukee, WI) for tumor staging evaluation incorporates several MRI parameters to establish areas suspicious for prostate cancer: T1- and T2-weighted imaging, DWI, DCE, and/or MRS to demarcate areas suspicious for prostate cancer. Prostate images were viewed on a DYNACAD analytical software work station that projected calculated DCE-MRI parameters and diffusion coefficient maps as color overlays onto T2-weighted axial and coronal images (Fig. 1). All patient images were read by one expert uroradiologist (SV). The prostate gland was divided in six standard areas in coronal projections (right and left of urethral midline and base, mid, and apex in traditional coronal sextants). A four point mp-MRI scale score was applied to each area: 0: no lesion; 1: benign or inflammatory lesion; 2: equivocal between benign/inflammatory or malignant; 3: suspicious for cancer.

MRI-guided biopsy setting. On left side: Position of patient after insertion of DynaTRIM endorectal device with calculation of trajectory for the biopsy needle. On right side: Performing of the biopsy after defining the target lesion.
2. We performed an MRI-targeted US-guided prostate biopsy using a novel MRI-ultrasound fusion navigation system MyLab™Twice or direct MRI-guided prostate biopsy DynaTRIM navigation system for biopsy of the ROI (Fig. 2). Within an average of 2 to 3 weeks after initial mp-MRI, patients underwent MRI-targeted biopsy (MRI-suggested, fusion, and direct MR guided, respectively). Antibiotic prophylaxis was administered with 500 mg ciprofloxacin orally alone for patients in the third group. In addition, gentamicin 5 mg/kg was administered to patients in the first two groups intravenously just before the procedure. All biopsies were obtained through a needle guide inserted transrectally either assembled to a TRUS probe or positioned using an MRI compatible biopsy guide. In groups 1 and 2, 2 to 4 cores were taken from the ROI targeted lesions and labeled as directed with lesion location with an additional 10 to 12 cores of “random” biopsies labeled as random with sextant coordinates. In the third group, one to two cores were obtained from the suspicious ROI alone. Samples were processed by routine histopathologic evaluation performed by a single uropathologist (QJZ). Tumor clinical significance was primarily determined by widely currently accepted (D'Amico definitions 9 and Epstein 10 ) definitions if detailed pathology data from the screening biopsy were available.
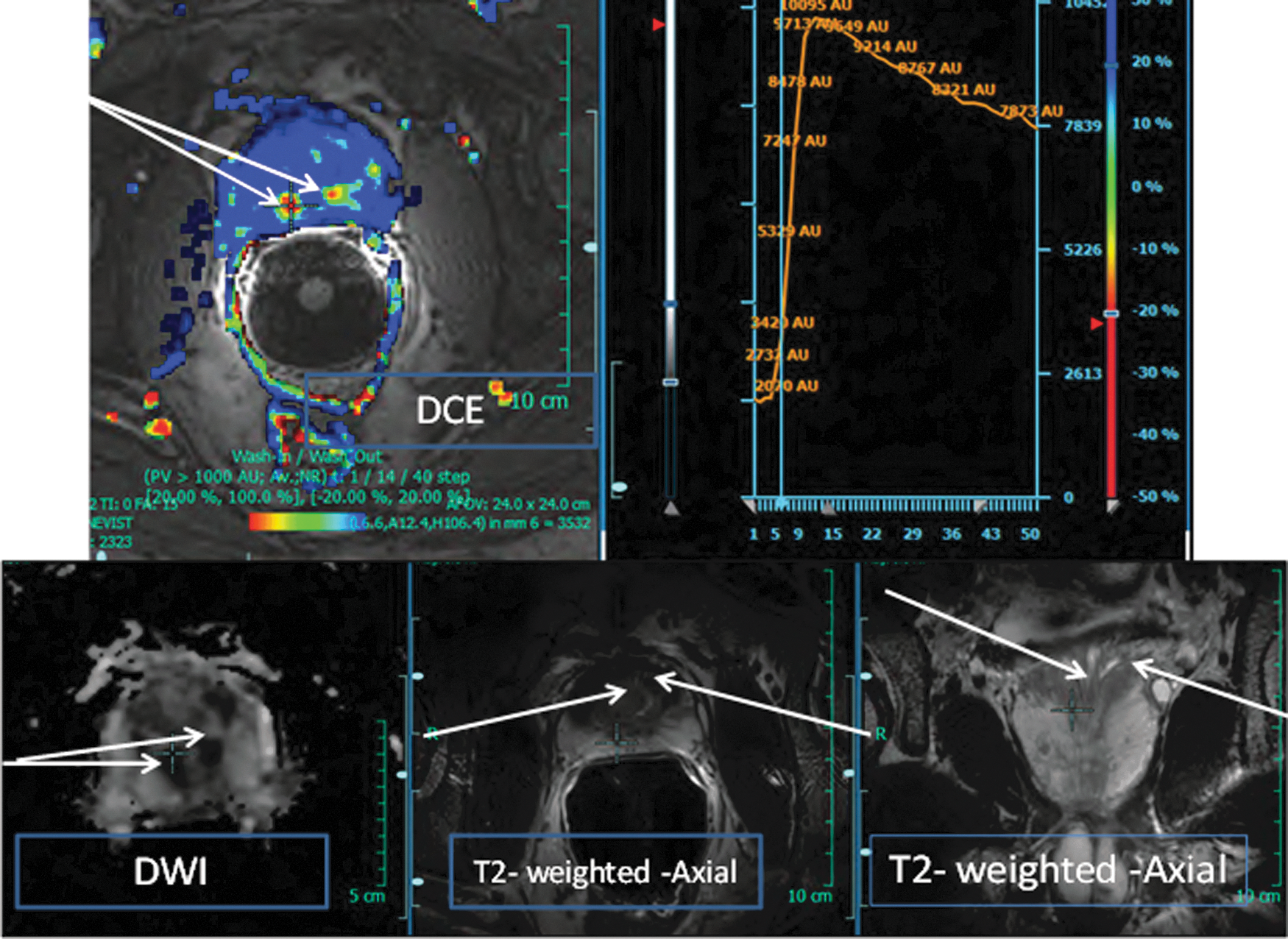
Case 1. 58-year-old man with a rising prostate-specific antigen level to 12.2. Multiparametric MRI shows suspicious low signal nodules (5 mm) (white arrows) in the right and left prostate base.
Statistical analysis
The chi-square test was used to calculate differences between group 1 and group 2. The nonparametric Mann-Whitney U test was performed to compare patient characteristics between the two groups with differences considered significant at P≤0.05. The 2×2 table was used to calculate sensitivity, specificity, and positive predictive value for MRI-suggested TRUS-guided and fusion MRI-TRUS biopsy with analysis of nontargeted cancers revealed by random biopsy of other areas. Statistical analysis was performed using SPSS,® version 20.0.01.
Results
Patient characteristics are presented in Table 1.
PSA=prostate-specific antigen; FP=false positive; FN=false negative; MRI=magnetic resonance imaging.
In group 1, two patients had a low-risk prostate cancer (T1c, Gleason score 3+3=6), being managed by active surveillance, while the other seven patients had slowly rising PSA levels with/or without DRE abnormalities. From these seven patients, two had just recently undergone biopsy and five had never undergone biopsy but demonstrated a slowly rising PSA level. In group 2, three patients had previously received a diagnosis of low-risk prostate cancer (T1c, Gleason score 3+3=6) managed by an active surveillance protocol, four patients had previous negative biopsy results, and six patients had slow rising PSA levels with or without DRE abnormalities. In group 3, 7 of 10 patients had low-risk prostate cancer based on previous biopsies and 3 patients had an elevated PSA level and no previous prostate biopsy.
The cancer detection rate of MRI-suggested TRUS-guided biopsy (group 1) was 33.3% (three of nine patients) while for fusion MRI-TRUS-guided biopsy (group 2), it was significantly higher: 46.2% (P=0.005), (Table 2). The sensitivity and specificity for group 1 was 45.5% and 33.3%, vs 61.9% and 20.8% in Group 2, respectively. The positive predictive value in group 1 was 50.0% vs 53.8% in group 2. In group 3 (MRI directed and guided biopsy), the cancer detection rate was much higher (80%) when compared with group 2 (P=0.005), although the majority of group 3 patients (7 of 10) had presented with previously diagnosed low-risk prostate cancer on TRUS-guided 12-core biopsy. Fusion biopsy (group 2) detected low-risk and low-volume disease in six cases (Fig. 3). In group 2, we found four cases of cancer lesions not targeted by mpMRI but discovered on “random” biopsy cores, all categorized as low-risk and low-volume cancer (Gleason score 3+3=6 and percent of tumor involvement [PTI] <10%). In group 1 (cognitive) with MRI-suggested TRUS-guided biopsy, cancer outside the targeted areas was discovered in three cases, one of them clinically significant with Gleason score 4+3=7 and PTI of 50%.
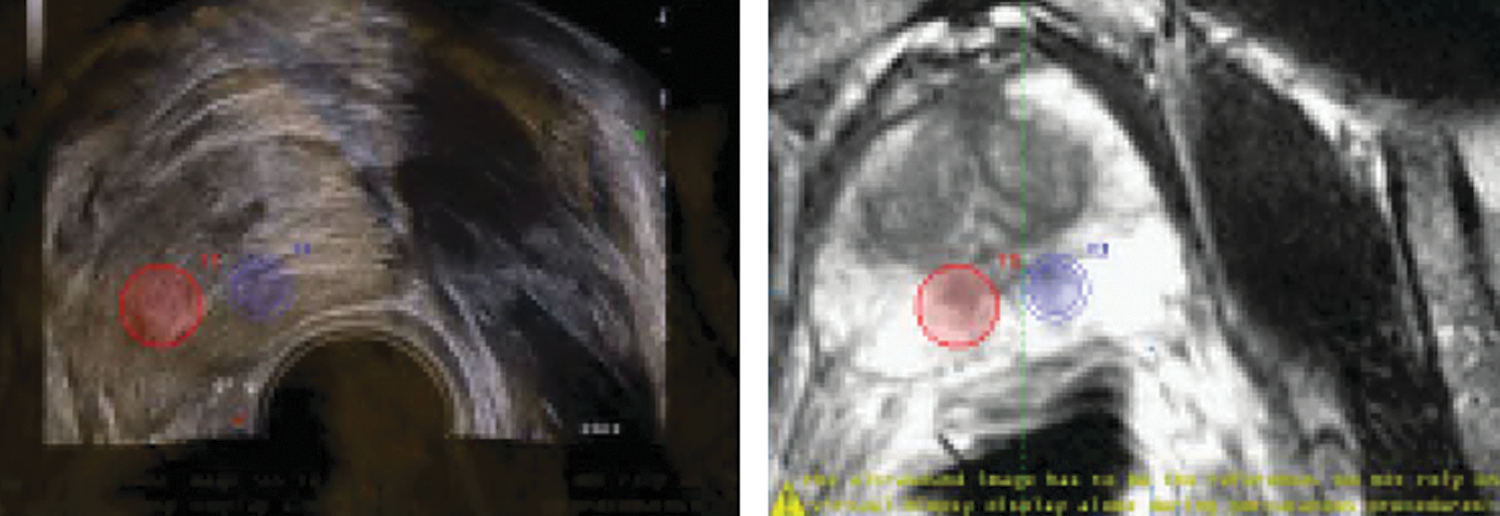
Case 1. 58-ear-old man with a rising prostate-specific antigen level to 12.2. On left side: Fusion of mp-MRI targets (as a red and blue circle) with transrectal ultrasonography images to perform a targeted prostate biopsy. On right side: Prebiopsy uploaded MRI image with suspicious two targets.
In 8 of 10 group 3 (MRI directed and guided) patients, MRI-guided biopsy confirmed low-risk and low-volume PCa. Pathologic examination of the negative MRI targeted and guided biopsies indicated benign lesion: Prostate atrophy and prostatitis.
Discussion
Eradication of cancer at an early stage offers the best chance for reducing cancer morbidity and mortality. Since the introduction of PCa screening in the United States with PSA and DRE, the clinical characteristics of the patients at the time of presentation has changed: Younger age at diagnosis, increased incidence of nonpalpable cancers, and decreased PSA level. This happened in parallel with an evolution of biopsy instruments and prostate coordinate schemes with subsequent changes in sampling methods and histopathologic interpretation.
Sextant biopsy have remained the standard practice at large academic centers with gradual transition to increase in biopsy number to 8, 10, 12, and 24 (saturation) core biopsies with the intent of increasing sensitivity to detect cancer. 11 The standard sextant prostate biopsy cannot provide reliable information about the low volume or low risk of PCa. 12 Beyond the increase in number of cores retrieved, precise imaging will improve the efficiency of diagnosis and reliability of localization for patients in whom this information would be relevant (eg, active surveillance or focal therapy).
The use of mp-MRI is capable of detecting low-risk (Gleason 6) disease with greater sensitivity and specificity when compared with traditional US-guided “random” biopsy as demonstrated by patients with previous negative prostate biopsy results with rising PSA whose cancer was correctly targeted by mp-MRI. 13 The addition of fusion imaging allows greater precision in coregistering MRI and US images to provide assurance of biopsy of the lesion when superimposed on the real-time US image with positive diagnosis in 6 of 13 (46%) patients. Furthermore, within the limitations of our study, fusion imaging did not miss intermediate-risk prostate cancer (Gleason 7), in contrast to cognitive US guidance to MRI targets.
On the other hand, fusion MRI-TRUS biopsy did not detect low-risk PCa foci demonstrated in nontargeted areas in three patients. The value of mp-MRI to detect a low-risk PCa is clear, especially in the light of a revolutionary paradigm shift in PCa management toward active surveillance or focal targeted therapy to avoid overtreatment and “right-size” the treatment to the severity of the disease.
We compared a group of patients who underwent cognitive targeted biopsy (group 1) vs a cohort of patients with fusion biopsy (group 2) clinically equivalent for measurable characteristics such as age and PSA level. The detection rate for low-risk disease in the first group was 33% including one patient with intermediate-risk disease vs 46% in the second group (P≤0.005). We intentionally did not compare group 3 patients with MRI-guided biopsy with group 1 and group 2 because there were no non-TRUS guided “random” biopsies in this group. This study demonstrates the feasibility of this modality for cancer lesion follow-up.
The primary limitation of this study is the small sample size that limits definitive conclusions about the value of mp-MRI and novel navigation systems for targeted biopsy. Our initial experience, however, demonstrated promise for this approach, especially for fusion MRI-TRUS guided or MRI-guided biopsy. Previous MRI-guided biopsy is probably the most accurate technique because it does not require translation of tumor suspicious lesions to another imaging technique where some distortion or nonprecise superimposition is inevitable. The current body of literature has the shown the value of mp-MRI–guided biopsy for low-risk prostate cancer.
Historically, urologists have not depended on radiology when diagnosing prostate cancer during the evolution of techniques beginning with transurethral biopsy at the time of transurethral resection of the prostate (1970), followed by transperineal prostate biopsy guided by digital palpation of the needle in the rectal submucosa or pararectal space (1980), and digital-rectal finger-guided fine needle aspiration for cytology.
When transrectal US guidance was established, urologists essentially embraced this technology and adapted to become radiologist and urologist combined. We recognize, however, that MRI 3T imaging centers are typically institutional assets, not owned and operated by urologists. So prostate cancer diagnosis will necessitate collaboration and delineation of responsibilities between urologist and radiologist similar to what is a standard operating collaboration for the diagnosis and treatment of renal tumors. Whether the MRI targets are processed with cognitive US guidance or through fusion imaging from MRI to US, we believe that MRI machines cannot be devoted to imaging and biopsy guidance because of the expense of this resource. Thus the use of fusion MRI-TRUS–guided biopsy is ideal for use in an oupatient office setting or in the outpatient surgery suite.
Our early results are promising with respect to the value of prostate mp-MRI in patients in whom prostate cancer is suspected. Increase in accuracy with the use of fusion imaging for targeting will further increase the efficiency of prostate biopsy by reducing the number of repeated biopsies in diagnostic and active surveillance settings. This study is clearly not conclusive, however. Multicenter collaborative studies are desperately needed to modify and verify these technologies and imaging strategies before they can be widely adapted. We must be cautious and recognize the complexity of the multiparametric MRI image acquisition and postacquisition processing, which demands the expertise and experience of a dedicated radiologist uon whom the program is built to last.
Conclusion
Our preliminary experience of mp-MRI suggests an increase in early detection of early stage prostate cancer disease with low-risk features yields potential candidates for focal targeted therapy. The MRI-TRUS fusion system increases diagnostic yield, while the highest detection rate was found with the use of direct mp-MRI targeted MRI-guided biopsy.
Footnotes
Disclosure Statement
No competing financial interests exist.