
Abstract
Purpose:
Transurethral resection of prostate (TURP) still represents the gold standard in the surgical treatment of symptomatic benign prostatic hyperplasia (BPH). The most frequent complication is represented by intra- and perioperative bleeding. Preoperative use of 5-alpha-reductase inhibitors (finasteride or dutasteride) to reduce surgical bleeding is still a topic of debate in literature.
Previous studies provided favorable data on blood loss reduction by preoperative administration of finasteride or dutasteride. The aim of this study was to evaluate whether pretreatment with dutasteride for six weeks before surgery can reduce surgical blood loss.
Methods:
A total of 142 patients with BPH—who were to undergo TURP—were enrolled and randomized into two groups. The dutasteride group comprising of 71 patients, was treated with dutasteride (0.5 mg/day) for 6 weeks before surgery and the control group, comprising of other 71 patients, did not receive dutasteride. Blood loss was evaluated in terms of a reduction in the serum hemoglobin level (ΔHb and ΔHCT), and was estimated by measuring the Hb and hematocrit levels before and 24 hours after surgery.
Results:
None of the patients treated with dutasteride reported any side effects. A significantly lower mean blood loss was observed in the dutasteride group compared to the control group (ΔHb=−1.29±0.81 v −1.83±1.25, respectively, p<0.0027; ΔHCT=−5.67±2.58 v −6.50±2.40, respectively, p<0.0491).
Conclusions:
Our results showed that pretreatment with dutasteride for 6 weeks before TURP reduces the surgical bleeding considerably. This treatment schedule can be used routinely to decrease TURP surgical bleeding.
Introduction
Methods
Between January and December 2010, 142 patients, who agreed to undergo TURP for symptomatic BPH, chosen randomly after applying the exclusion criteria, were enrolled in the study. All the patients signed an informed consent form before their enrolment in the study. The study was conducted in accordance with the Declaration of Helsinki and was approved by the local Medical Ethics Committee.
All the patients were treated with alpha-blockers before TURP. To evaluate the prostate volume, transrectal ultrasonography was performed within 10 days before surgery, after the completion of dutasteride pretreatment. A routine hematologic analysis, including prostate-specific antigen (PSA), was also performed.
Patients were divided equally by simple randomization (after a stratified randomization to control all the baseline covariates between the two study arms) into two treatment groups to avoid bias: the first group, comprising of 71 patients, received pharmacological therapy with dutasteride (0.5 mg/day) for 6 weeks before surgery (dutasteride group); the second group comprising of the other 71 patients did not receive dutasteride (control group). The body mass index of the control group was comparable to that of the treatment group and ranged between 19.6–26.3. Patients who had renal impairment, previous invasive procedures of the prostate, or coagulation disorders were excluded from the study. In total, 16 patients were excluded, out of which 8 patients were on NSAIDs and aspirin (four patients belonging to the group treated with dutasteride and four to the untreated control group). Intake of nonsteroidal anti-inflammatory drugs and aspirin was discontinued 2 weeks before surgery. Spinal anesthesia was given to all patients. The same expert surgeon performed all the procedures using a 26-Ch resectoscope (Karl Storz, Tuttlingen, Germany). Furthermore, the surgeon was blind to each patient's profile (with or without dutasteride pretreatment) to prevent a possible bias. Blood loss, indicated by the reduction in hemoglobin (ΔHb) and hematocrit (ΔHCT) levels, was estimated by measuring Hb and HCT values before surgery and 24 hours after surgery. Although it may be more accurate to do the measurement after 48 hours, but for comparison purpose, we believe that the relative effect at 24 hours or 48 hours will be similar. Hence, to reduce the total time of experimentation and measurements, we estimated Hb at 24 hours after surgery. Dilution can affect the results of Hgb. Therefore, the amount and rate of dilution by intravenous hydration to the cohort after surgery was maintained constant at 1500 mL. The rate of hydration was maintained at 125 mL/hour.
Resected prostate weight and operation time were recorded at the end of the procedure. The catheter was removed 48 hours after surgery for all patients. The results are expressed as mean±SD and median. The Student's t-test was used to compare the patients' variables (prostate volume, resected prostate weight, and blood loss) of both the groups; p<0.05 was considered statistically significant.
Results
There was no statistically significant difference between the two groups with regard to age, prostate volume, resected prostate weight, PSA, and operation time (Table 1). None of the patients reported any side effects with dutasteride treatment. The dutasteride-treated cohort was confirmed to be 5-ARI naïve. The average hospital stay after surgery for patients from both the cohort was 3.6 days. Only two patients in the control group required new catheterization for clot retention, and only one patient needed a transfusion of 1 unit of blood. There was a significantly lower mean blood loss in the dutasteride group compared to the control group (ΔHb=−1.29±0.81 v−1.83±1.25, respectively, p<0.0027; ΔHCT=−5.67±2.58 v −6.50±2.40, respectively, p<0.0491) (Fig. 1).
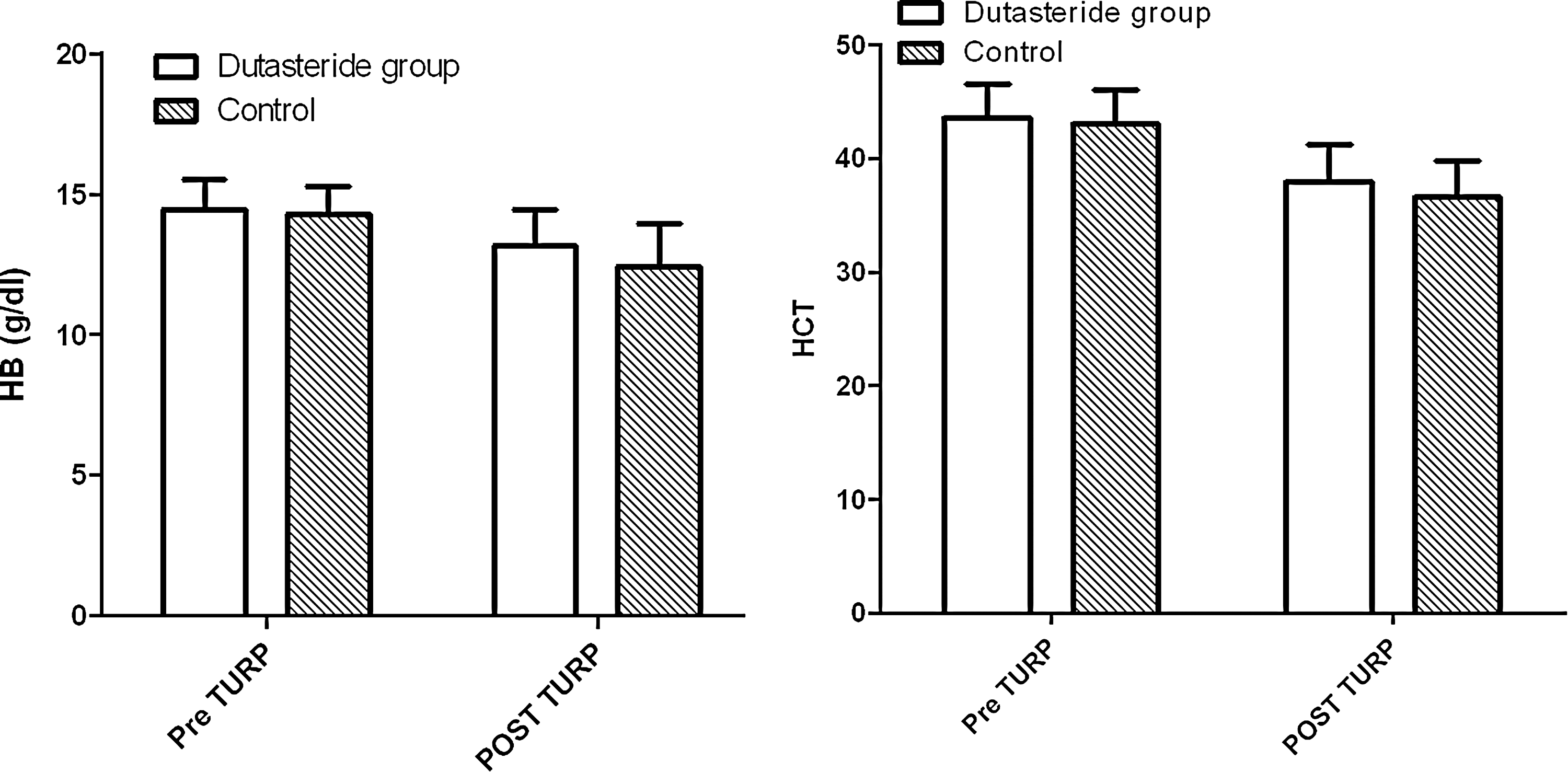
Mean change of hemoglobin (Hb) and hematocrit (HCT) levels (baseline v after surgery) in the two treatment groups.
Values are represented as mean±SD (Standard Deviation); median.
p<0.05.
Δ Hb=delta hemoglobin; Δ HCT=delta hematocrit; PSA=prostate-specific antigen; TURP=transurethral resection of the prostate.
Discussion
TURP still represents the gold standard in the surgical treatment of symptomatic BPH. One of the most important complications of TURP is intra- and perioperative bleeding, which sometimes leads to urine retention because of blood clots. BPH is characterized by increased proliferation of stromal and acinar cells around the urethra sustained by increased gland vascularity (neoangiogenesis). Some studies demonstrated the effect of finasteride in reducing BPH-related hematuria. 2 –4 Finasteride, which blocks the conversion of testosterone to dihydrotestosterone, decreases the activity of androgen-controlled growth factors responsible for angiogenesis. This feature was used to prevent intraoperative bleeding in patients undergoing TURP. Some studies supported the pharmacological use of finasteride to reduce surgical blood loss. 2 –6 Dutasteride is an inhibitor of type 1 and 2 isoenzymes of 5-alpha reductase commonly used, as is finasteride, for treatment of symptomatic BPH.
Some studies attempted to resolve whether dutasteride could be used to reduce bleeding after TURP in the same way that finasteride is 7 –11 Hahn et al used dutasteride for 2–4 weeks before TURP without significant reduction in blood loss compared to the placebo group. 7
Other authors have confirmed these results, concluding that a short-term treatment with dutasteride was not superior compared to the control group in decreasing TURP-related blood loss, and suggested that a longer duration treatment will reduce intraoperative and postoperative bleeding. 8 –10 Martov found a significant reduction in blood loss in patients by using dutasteride for at least 1 month before TURP compared to the control group. 11 Kravchick demonstrated that 6 weeks of treatment with dutasteride reduced prostatic vascularity, especially in the periurethral area. 1 Based on these evidences, we attempted to evaluate if pretreatment with dutasteride (0.5 mg/day) for 6 weeks before TURP could reduce surgical bleeding. None of the previous authors had used dutasteride for 6 weeks before surgery. The results of the present study showed that treatment with dutasteride for 6 weeks before TURP reduces surgical bleeding. No differences were found with regard to prostatic volume, prostate resected weight, and operation time between the dutasteride and control groups. Aim of our work was to verify that pretreatment with dutasteride helps in reducing surgical blood loss and validate this statistically for a large number of subjects. In this case, we have considered 71 patients in the study group and 71 in the control group. Although, in most cases the drop in HCT/Hgb (while statistically significant) was not clinically significant, but it is important considering that we have enrolled a large number of patients (i.e., 71) in each group.
Based on the results of this study, we can conclude that 6 weeks of pharmacological treatment with dutasteride seems to be sufficient to reduce prostate tissue vascularity.
Footnotes
Acknowledgments
The authors declare that the manuscript has not been supported by any sources of support, including sponsorship and any sources of material.
Disclosure Statement
The authors declare no conflict of interest.