
Abstract
Purpose:
To present our experience and the feasibility with laparoscopic ureteral reimplantation using ureteral tapering (intracorporeal or extracorporeal) for symptomatic primary obstructive megaureter.
Patients and Methods:
Between June 2005 and September 2010, 11 patients (mean age: 33.2 years) with symptomatic congenital primary obstructive megaureter underwent laparoscopic reconstruction. All patients underwent laparoscopic intracorporeal or extracorporeal ureteral tailoring and ureteroneocystostomy by the same surgical team. The relevant perioperative details and complications were recorded.
Results:
No open conversions or blood transfusions were necessary. Total mean operative time was 142 minutes (range 109–227 min). The mean operative time for the five patients with intracorporeal tailoring was 154 minutes (range 121–227 min), compared with 125 minutes (range 109–165 min) for the six patients with extracorporeal tailoring. The mean blood loss was 45 mL (range 30–85 mL) for all cases. Mean postoperative hospital stay was 6.4 days (range 5–8 days). In one patient, urinary leakage was noted immediately postoperatively; it disappeared spontaneously with conservative treatment by postoperative day 7. Average follow-up was 18 months (range 13–24 mos). Follow-up renal ultrasonography and intravenous urography confirmed decreased hydronephrosis with good drainage. Nonobstructed clearance was also demonstrated using diuretic renography in all cases.
Conclusions:
Laparoscopic intracorporeal or extracorporeal ureteral tailoring and ureteroneocystostomy is a feasible and reproducible procedure. Follow-up revealed satisfactory objective and subjective outcomes.
Introduction
The aim of this retrospective study was to report our experience with laparoscopic ureteral reimplantation using intracorporeal or extracorporeal tapering for symptomatic POM.
Patients and Methods
Between June 2005 and September 2010 at our tertiary care center, symptomatic POM was diagnosed in 11 patients (8 men and 3 women) with a mean age of 33.2 years (range 18–49 years). All patients presented with different degrees of flank pain, and two patients had concomitant urinary tract infection. All patients underwent laparoscopic intracorporeal or extracorporeal ureteral tailoring and ureteroneocystostomy by the same surgical team.
Preoperative laboratory assessments included urinalysis, urine culture, and serum urea and creatinine levels. All patients were evaluated using abdominopelvic ultrasonography, intravenous urography (IVU), voiding cystourethrography, and/or reconstructed spiral CT. Obstruction was confirmed by a diuretic technetium-99-diethylenetriaminepenta-acetic acid scan with the gamma camera moved to the level of the ureterovesical junction (UVJ) with a perurethral catheter in place to drain the bladder. Operative time, blood loss, postoperative hospital stay, and intraoperative and postoperative complications were recorded.
Operative technique
Step 1: Position
After induction of general anesthesia, a 4F ureteral catheter was placed cystoscopically to facilitate ureteral identification and tailoring. Subsequently, the patient was placed in the lithotomy position. A gel pad was placed under the ipsilateral gluteal region to elevate the affected side.
Step 2: Port placement
A 10-mm port for the laparoscope was established just superior to the umbilicus. Another three ports were placed for visualization.
Intracorporeal: A 10-mm port was placed on the midline midway between the umbilicus and the pubic symphysis. Two 5-mm ports were placed bilaterally on the midline midway between the umbilicus and the anterior superior iliac spine (Fig. 1).
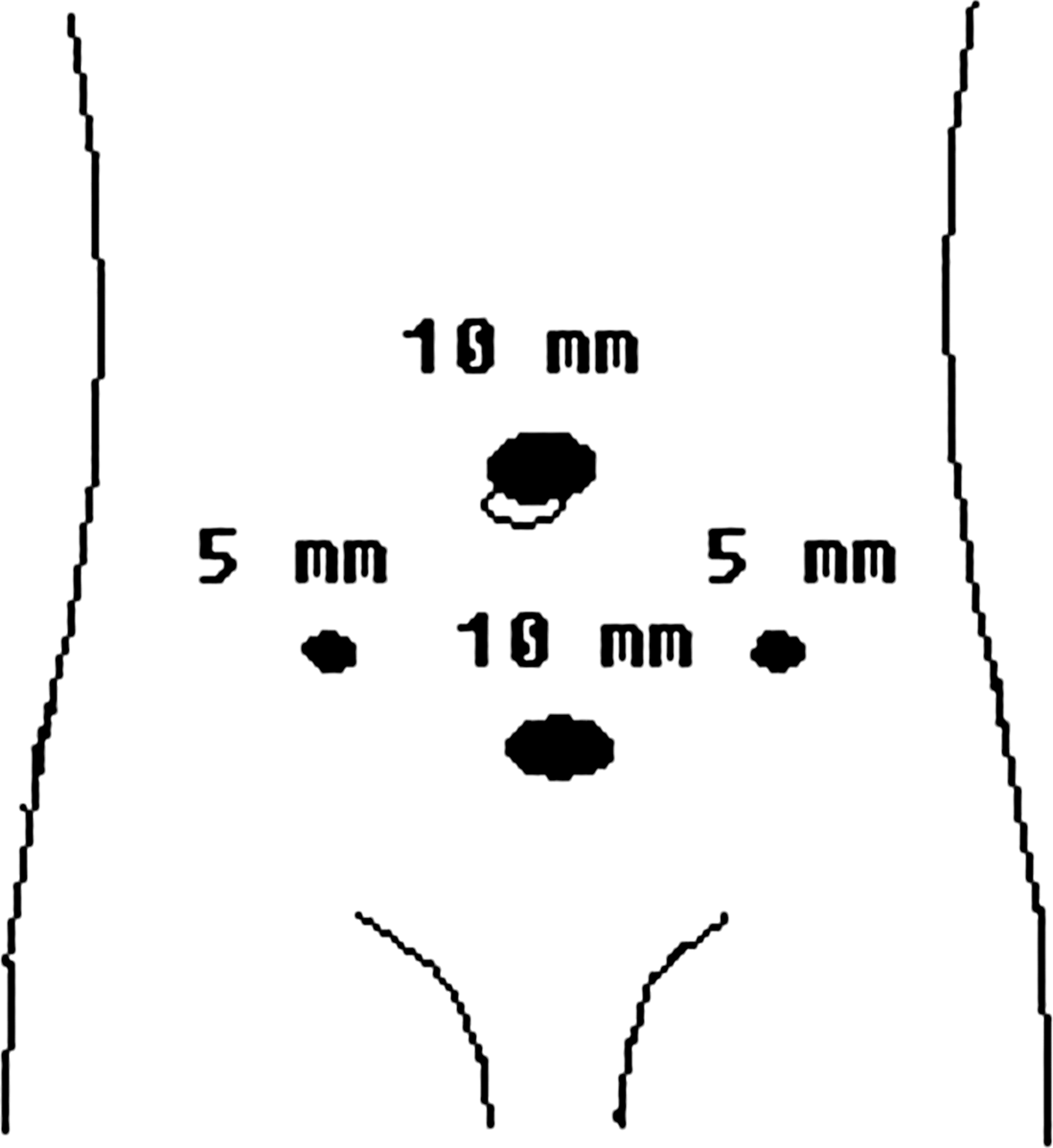
Port placement for intracorporeal ureteral tailoring procedure.
Extracorporeal: A 10-mm port was placed on the midline midway between the umbilicus and the affected side of the anterior superior iliac spine. A 5-mm port was placed on the midline midway between the umbilicus and the contralateral anterior superior iliac spine. A second 5-mm port was placed on the midline midway between the umbilicus and the pubic symphysis (Fig. 2).

Port placement for extracorporeal ureteral tailoring procedure (left-sided). Port placement for the right-sided procedure is a mirror image of the left-sided port placement.
Step 3: Exposure transection of ureter
The colon was reflected medially following an incision along the homolateral line of Toldt. The ureter was exposed and dissected circumferentially to the bladder, locating the narrow adynamic segment of the UVJ and resecting it sufficiently. Special care was needed to preserve the ureteral adventitia, which helps prevent postoperative ischemia.
Step 4: Ureteral tailoring and suturing
Intracorporeal: Fixing the lateral wall of the ureter with atraumatic graspers on each side, the ureter was incised with cold shears through the port located on the midline midway between the umbilicus and the pubic symphysis. The redundant portion of the ureter was excised so that the distance of the two longitudinal cut edges was maintained at 1.5 to 2.0 cm. After the excision, a 6F Double-J stent was threaded through the port over a preplaced guidewire. Subsequently, the tapered ureter was sutured with 4-0 polyglactin using a continuous lock-stitch suture. Interrupted sutures were used for reinforcement.
Extracorporeal: The ureter was anatomized slightly upward to acquire extra length. Subsequently, the free ureteral end was delivered out through the ipsilateral 10-mm port and a 6F Double-J stent was placed in the ureter. Tapering and reconstruction of the ureter was similar to open surgery. The tapered ureter was returned to the peritoneal cavity.
Step 5: Ureteroneocystostomy
The bladder was filled with physiologic saline and a 1 to 1.5 cm longitudinal incision was made in the ipsilateral posterosuperior aspect. The pouting mucosa at the lowest part of the incision was opened using blunt dissection. A mucosa to mucosa ureterovesical anastomosis was completed with interrupted 4-0 polyglactin sutures at 6 o'clock, continuing the anastomosis in turn at 12, 8, 10, 2, and 4 o'clock after the distal end of the Double-J stent was fixed in the bladder. The detrusor and serosal layers were closed over the ureter to create a possible submucosal tunnel for an antireflux mechanism.
Step 6: Extraperitonealization of anastomosis
Hemostasis was checked carefully after reducing the pneumoperitoneal pressure. The posterior peritoneum was closed with continuous 2-0 polyglactin sutures, and an indwelling closed suction extraperitoneal drain was installed.
Results
No open conversions or blood transfusions were necessary. Mean total operative time was 142 minutes (range 109–227 min). The mean operative time for the five patients with intracorporeal tailoring was 154 minutes (range 121–227 min), compared with 125 minutes (range 109–165 min) for the six patients with extracorporeal tailoring. The mean blood loss was 45 mL (range 30–85 mL) for all cases. The use of analgesics postoperatively was minimal. The closed suction drain and Foley catheter were removed 3 to 5 days and 4 to 6 days postoperatively, respectively. The Double-J stent was removed 4 to 6 weeks postoperatively, and the mean postoperative hospital stay was 6.4 days (range 5–8 days).
Urinary leakage was noted immediately postoperatively in one patient after intracorporeal tailoring; leakage disappeared spontaneously with conservative treatment by postoperative day 7. Mean follow-up was 18 months (range 13–24 mos), and all patients experienced relief of symptoms. Follow-up renal ultrasonography and IVU confirmed decreased hydronephrosis with good drainage, and nonobstructed clearance was demonstrated using diuretic renography in all cases.
Discussion
Megaureter can be classified as primary (or intrinsic) or secondary. According to the international classification of Smith and associates, 4 it can also be classified as refluxing, obstructed, refluxing and obstructed, or neither refluxing nor obstructing. POM is characterized by a functional obstruction. There is considered to be an adynamic juxtavesical segment in the ureter, resulting in a lack of dissemination of ureteral peristalsis and, therefore, reduced urine flow rate.
With improved imaging technology and antenatal care, the diagnosis of megaureter is no longer difficult. In children, the overwhelming majority of asymptomatic megaureters regress or resolve without surgical intervention, 5 and surgical management is usually advocated when POM is associated with increasing dilation, symptoms, or progressive renal damage. 6 In adults, because kidney and ureter development is complete and POM is associated with complications such as urinary tract infections and stone formation, idiopathic resolution is unlikely and surgical intervention is usually indicated.
Surgical options for POM include open, laparoscopic, or endoscopic repair. Surgical endoscopy is minimally invasive; however, because the affected ureteral segment is retained, results are not acceptable. 7 Open surgery remains the gold standard because of excellent success rates. 8,9 Despite an encouraging report in 1994 by Ehrlich and colleaues, 10 laparoscopic ureteroneocystostomy remains technically challenging because ureteral intracorporeal tailoring and suturing has a steep learning curve.
There are two main types of ureteral tailoring techniques. Ureteral plication is used for mild to moderately dilated ureters but is associated with more complications for ureters wider than 1.75 cm diameter. 11 The excisional tapering technique described by Hendren 12 is suitable for massively dilated or thickened ureters. We performed excisional tapering in all the cases because our patients had megaureters ≥2.0 cm diameter.
The extent of ureteral tailoring depends on individual patients. Ideally, ureteral incisal margins are maintained at 1.5 to 2.0 cm after excisional tapering. This distance can be increased slightly to avoid ureteral stricture when severe adhesions of the ureter to the peripheral tissues are present. It is important, however, to avoid strain on the anastomosis and avoid redundancy beyond 2 to 3 cm. Most experts recommend that the medial ureter is incised and tailored to preserve the blood supply that comes from the iliac vessels laterally. Some megaureters, however, are significantly dilated or distorted, and a true dissecting relationship of the blood vessels supplying the ureter is atypical. Laparoscopy could preserve the blood supply to the ureter in such cases.
The ureteral orifice should be beveled to appropriately anastomose with the bladder. The caliber of the anastomosis must be moderate because too small a caliber may lead to postoperative ureterostenosis and too large may result in urine reflux. In our study, we accomplished nonrefluxing extravesical suprahiatal reimplantation with a caliber of anastomosis of approximately 1 cm. We did not find regurgitation or reobstruction in the follow-up period.
There are two methods of ureteral tailoring: Intracorporeal and extracorporeal. Ansari and coworkers 13 described their experience with extracorporeal tailoring for megaureter in three patients. Their method is similar to ours, but the differences are the position and size of the port where the lower ureteral end was delivered. In our study, we exteriorized the ureter through the ipsilateral 10-mm port with minimal invasion.
We prefer extracorporeal tailoring if the situation allows, for the following reasons: First, pulling the free ureteral end through the ipsilateral 10-mm port is not difficult. Second, extracorporeal tailoring and suturing for megaureter is not only an easy operation compared with the intracorporeal procedure, but it is also less time-consuming. Third, placement of a Double-J stent is also easier when the ureter is exteriorized. In our series, the mean operative time is 125 minutes for the six patients with intracorporeal tailoring, and shorter than the 154 minutes for the five patients with extracorporeal tailoring. More of the upper ureter is required to exteriorize adequately, however, and this may lead to ischemia. In our study, no ureteral ischemia was found in the extracorporeal tailoring cases within the follow-up period. Extracorporeal tailoring may also result in excessive traction on the ureter and may not be feasible in an obese patient.
Intracorporeal tailoring is necessary in some circumstances. The concern is maintaining orientation when making the excision and suturing the ureter. Agarwal and associates 14 reported a novel technique for intracorporeal excisional tailoring of megaureter with satisfactory results in three young men. The difference with their technique is that they did not disconnect the ureter before tailoring was completed and thus the rotational orientation was maintained.
In our series, the port placed on the midline midway between the umbilicus and the pubic symphysis was very important. During the procedure, the ureter can be tailored by inserting laparoscopic scissors into the peritoneal cavity through this port, and threading of the Double-J stent over a preplaced guidewire can be performed with relative ease. During the suturing procedure, we put traction on the ureter using an atraumatic grasper through this port. The location, orientation, and degree of traction can be varied providing versatility during this procedure and making for more convenient suturing. Mean operative time in our cases with intracorporeal tailoring was 154 minutes and slightly shorter than the operative time in other reports.
In our study, the mean postoperative hospital stay was 6.4 days longer than that reported in the literature. Because of differences in medical insurance between China and other countries, most Chinese patients stay in the hospital until they can return to normal activity. Another reason for the greater length of stay in our study is that urinary leakage was noted in one patient in the early postoperative period. Although it disappeared spontaneously with conservative treatment, it also prolonged hospitalization.
Recently, robotic assistance has been successfully used in certain areas of urology and is well accepted. 15 –17 The articulated arm of the robot can mimic the dexterity of the human wrist, and this increases the degree of freedom, especially during dissection and suturing. This may contribute to shorter operative times and learning curves. The current limitation of this technique is the high price, however.
Conclusions
Our results demonstrated that laparoscopic intracorporeal or extracorporeal ureteral tailoring and ureteroneocystostomy is a feasible and reproducible procedure. Follow-up revealed satisfactory objective and subjective outcomes comparable with those seen in open surgical procedures.
Footnotes
Disclosure Statement
No competing financial interests exist.