
Abstract
Purpose:
We describe an extended training program using the pelvitrainer to improve the basic laparoscopic skills of the junior urologists.
Materials and Methods:
Ten junior residents were involved in our program that consisted of an hour of training every other day; every 3 hours represented one training session. This curriculum started with 4 inanimate tasks that included peg transfer, disc cutout, extracorporeal, and intracorporeal knot tying. Each task was practiced for one training session with an objective evaluation at the initial attempt and at the end of its session. Thereafter, the participants began to perform an anastomosis using a latex glove model of the laparoscopic urethrovesical anastmosis (L-UVA) (5 experiments). This was followed by 10 experiments of the sheep intestine model of the L-UVA. The performance in these models was evaluated by both the amount of leakage of the injected saline and the time required for completing it. Lastly, another sheep intestine model was performed 3 weeks after the end of the training program.
Results:
The continuous evaluation of these trainees showed that there was a significant decrease in the time required to perform each of the first 4 tasks at the end of their corresponding sessions compared to the base line values (p=0.000). We also detected a significant decrease in the time and the amount of leakage in sheep intestine models in the 10th attempt compared to the first one (p=0.000). However, there was no significant difference between the results at the 10th model and those of the 3 weeks retest regarding both the time (p=0.198) and the amount of leakage (p=0.076).
Conclusions:
The use of the two described models of the L-UVA after the inanimate tasks in the pelvitrainer distributed course of training could help in the improvement and in the retention of the basic laparoscopic skills of the junior urologists.
Introduction
The urologist who would like to begin performing laparoscopy has to face many problems that include: the use of two-dimensional vision with loss of depth perception, the counterintuitive movements as a result of the fulcrum effect, the lack of direct tactile feedback, and the fatigue factor. However, the continuous and organized training is the only way to overcome these obstacles. Although, the training in the operating room is paramount, it is not suitable for acquiring the basic laparoscopic skills due to economical constrictions, patient safety, and medicolegal considerations. 1 –4 Therefore, various training models have been developed, including animal models, cadavers, electronic simulators (virtual reality simulation), pelvic trainers, and cardboard box trainers. 5 –10
The pelvitrainer provides a versatile and a relatively inexpensive means of laparoscopic training. Numerous exercises can be carried out in this box starting from simple tasks, such as manipulation of small objects, to more complicated ones, such as intracorporeal knot-tying and completing the anastomosis of a model of L-UVA or pyeloplasty. 11 –14 These exercises are used to help the trainee in the visual translation of the two-dimensional image into a three-dimensional construct to obtain familiarity with the laparoscopic instruments. They also enable trainees to gain eye–hand coordination and to improve spatial awareness. The in-vitro acquisition of these skills can help in shortening the learning curve and in the maintenance of the technical competence of the laparoscopic surgeons. 15
In this study, we described a progressive extended protocol using the pelvitrainer for the basic laparoscopic training of the junior urologists.
Materials and Methods
This study was carried out in the Tanta University Hospital after approval of the local ethics committee and it involved ten junior urology residents who underwent some training in open and endourological surgery, but they were not involved in any laparoscopic procedures. The whole training of these residents in this project, was mentored by four laparoscopic experts in the Urology Department and the pelvitrainer used was the “TRLCD05 Large Body MITS” (manufactured by 3-Dmed-USA) (Fig. 1).

The pelvitrainer.
Training tasks
The following exercises were practiced in order:
(1) Peg transfer. This was done by lifting one of the five objects in the pelvitrainer with a grasper in the left hand and transferring it midair to another grasper in the right hand to place it on a peg on the opposite side of the board. Once all of the five objects had been transferred, the process was reversed (Fig. 2).
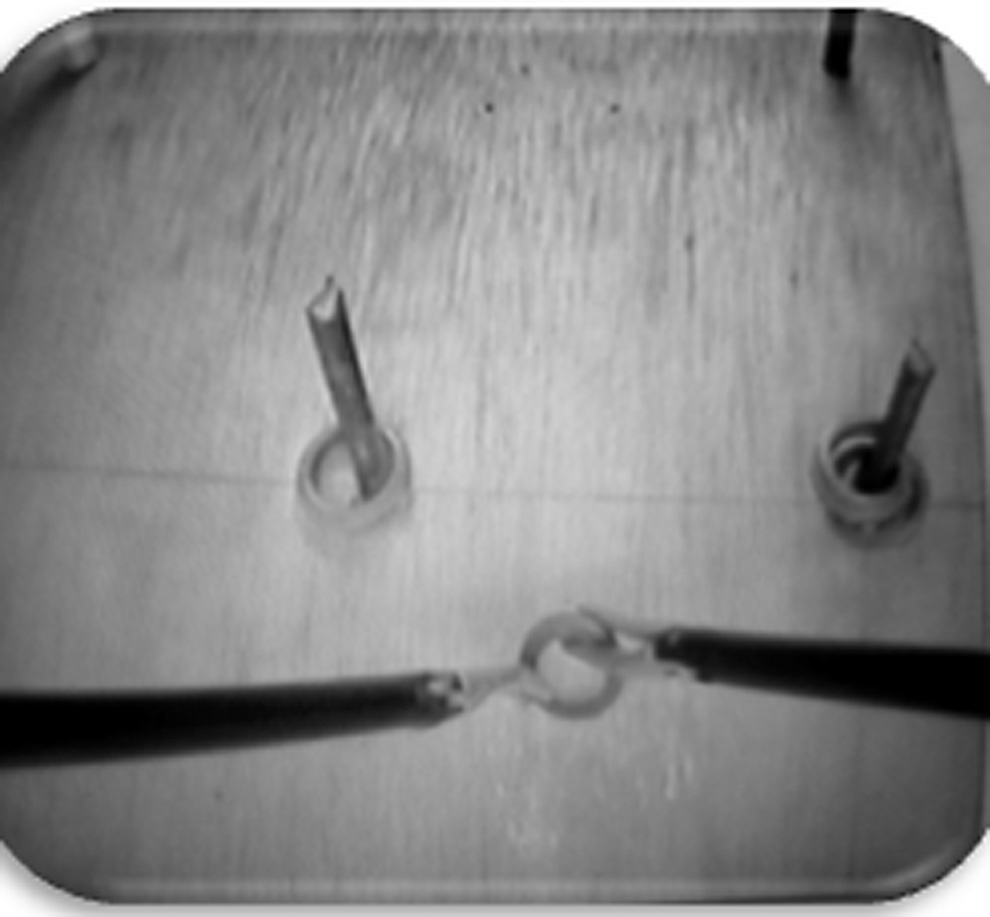
Peg transfer.
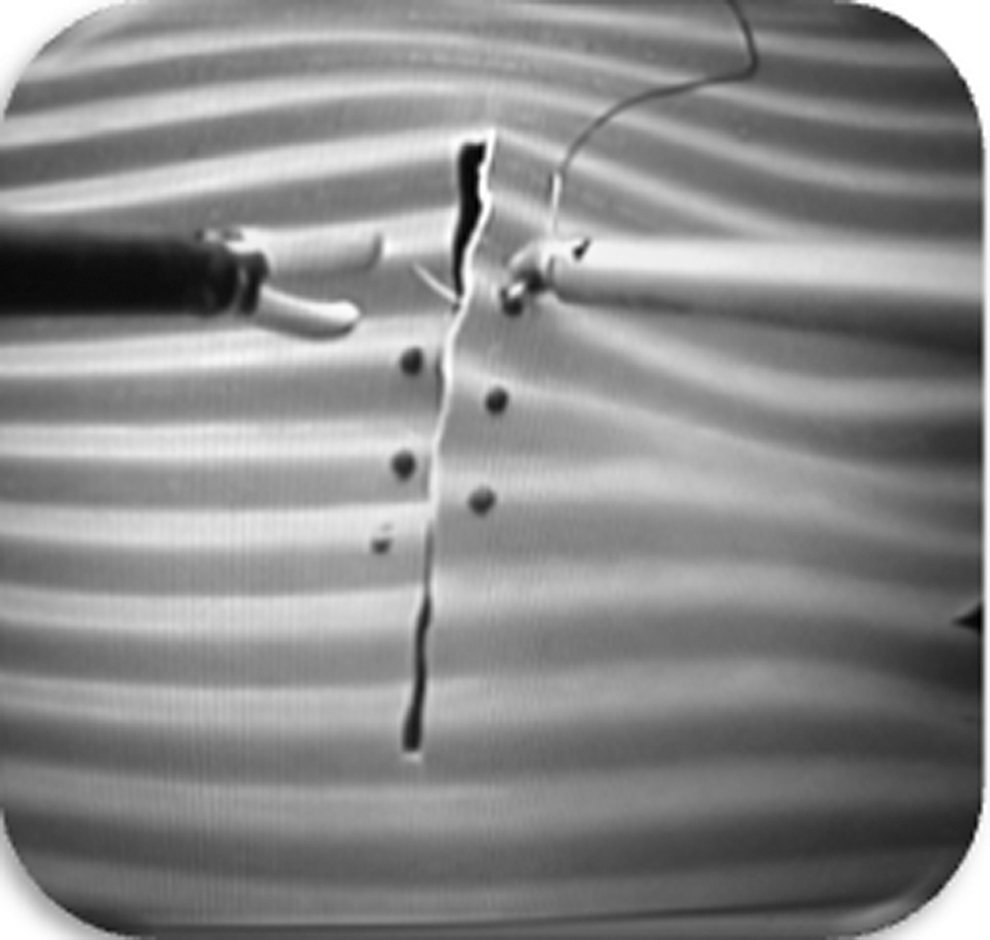
(2) Disc cutout. This was performed by cutting a predrawn circular pattern with endoscopic scissors. Errors were defined as any deviation from the premarked template (Fig. 3).

Disc cutout.
(3) Suturing with extracorporeal knot-tying. This task started with insertion of the suture (90–120-cm length, 2–0 silk) with its needle into the pelvitrainer and followed by the placement of the needle in the needle holder. The needle was then passed through two marks in a longitudinally slit rubber sheet. Thereafter, the trainee tied the suture extracorporeally using a knot pusher (Fig. 4).
Laparoscopic suturing.
(4) Suturing with intracorporeal knot-tying. This task was similar to the previous one, except that the suture was 15–20 cm and it was tied with the intracorporeal technique (Fig. 4).
(5) Models for L-UVA:
Two models were included in this protocol.
(a) Latex gloves model. This simplified model utilized the middle finger of the glove to simulate the bladder portion and the little one to simulate the urethral part. We used adhesive tapes to fix the middle finger of the glove to a 20-mL syringe and the little one to a centrifuge tube (Fig. 5). The model was then introduced into the pelvitrainer and an 18-F Foley catheter was placed through the urethra to be manipulated during the anastomosis. Two needles with 3/0 Vicryl® sutures were used for the anastomosis. They were placed outside-in through the bladder “middle finger of glove” and inside-out through the urethra “little finger of glove” at the 5:30 and 6:30-o'clock positions. Suturing was continued on each side (from the 5:30 and 6:30-o'clock positions) to the 12:00-o'clock position. An intracorporeal knot was then tied at the 12:00-o'clock position.

Latex gloves model of the laparoscopic urethrovesical anastomosis (L-UVA).
(b) Sheep intestine model. In this model, two 10–15-cm segments of sheep intestine were used to create a model of urethrovesical anastomosis. The plunger was removed from a 20-mL syringe, and the opposite end of the syringe was cut at a 45-degree angle. One of the segments of sheep intestine was placed over the syringe and secured to the syringe with 2–0 silk suture (bladder portion of the model). The other intestinal segment was fixed over a centrifuge tube (urethral portion), with 2–0 silk suture (Fig. 6). The anastomosis was done with 3/0 Vicryl® sutures in the same way described before.
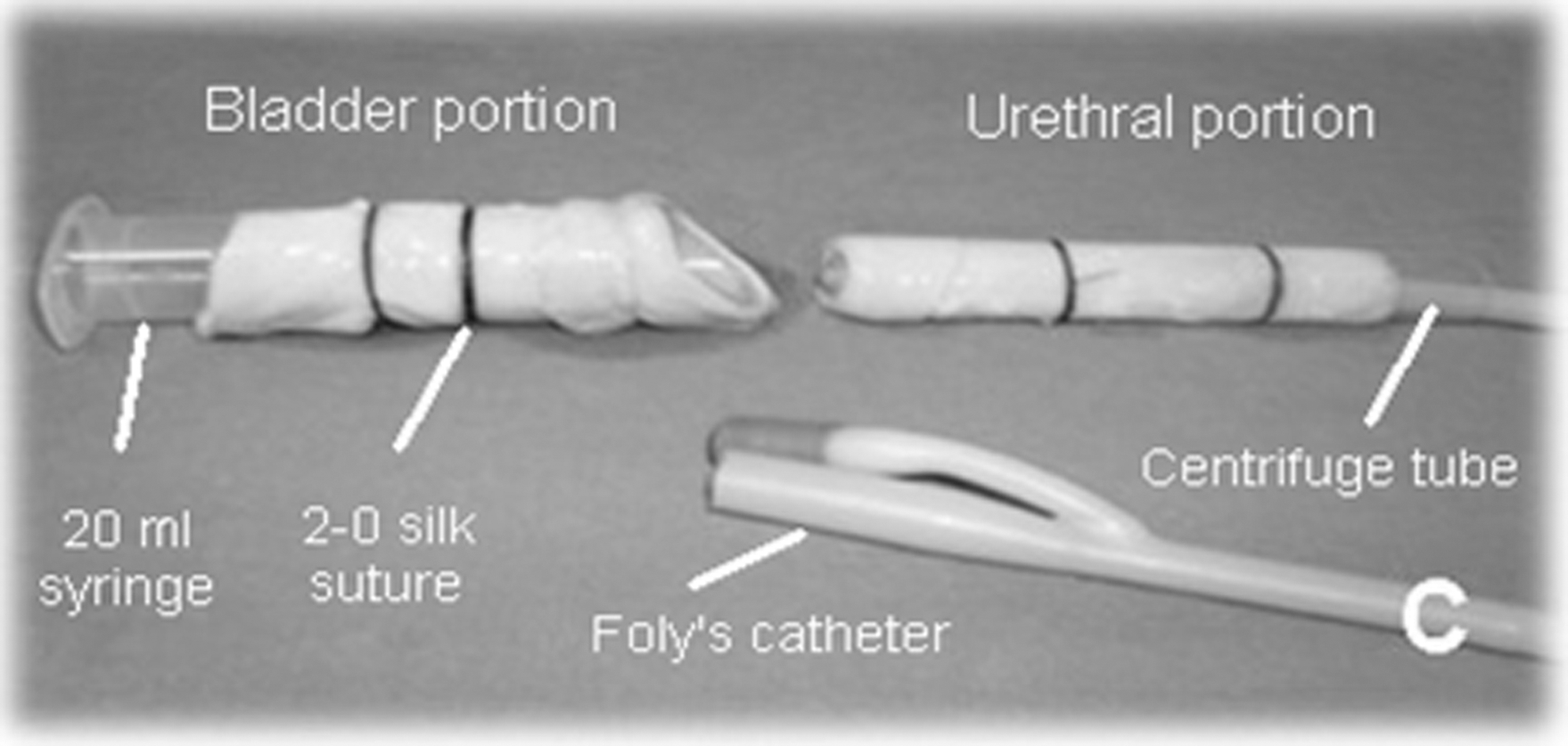
Sheep intestine model of the L-UVA.
At the end of the procedure, a syringe was connected to the bladder side of the anastomosis, and 30 mL of saline was slowly infused (by gravity only) through the anastomosis in an antegrade fashion. Petri dishes were placed underneath the anastomosis and at the distal end of the centrifuge tube to estimate the amount of leakage from the anastomotic site.
Training protocol
The trainees were asked to view an instructional video demonstrating the proper performance of each of the previous tasks (one at a time). Thereafter, each task was performed by a laparoscopic expert as a live demonstration. The trainees were then allowed to perform the previously seen experiment without assistance, but under continuous mentoring by the laparoscopic experts. The participants also had free access to the video tutorial during their training.
The training program was planned to be an hour of training every other day (i.e., 3 hours per week). Every 3 hours of training represented one training session. The first 4 tasks were practiced in order within 4 weeks (i.e., one session per week). The trainees underwent two evaluations; one at the beginning and the other at the end of each session. This evaluation included both the efficiency (time required to perform each task) and the precision of their performance. The trainee was allowed to shift to the next task only after reaching the proficiency level of the previous one. The proficiency level was defined as completion of the task within the specified time while performing it in a precise way (i.e., committing an allowable number of errors). The specified proficiency time of each task was obtained by calculating the mean time needed by three laparoscopic experts to do it.
The models of the urethrovesical anastomosis were designed to start by performing five latex gloves models. Thereafter, the trainees were allowed to perform ten models of the sheep intestine model in a course of a distributed fashion (i.e., one model every other day). Each performed anastomosis (sheep intestine model) was evaluated by both the quality (precision) and the time consumed (efficiency). The quality of the anastomosis was analyzed by measuring the amount of leakage of the injected saline as discussed previously. The progression in both time and quality of the performed anastomosis was evaluated at three occasions: • The baseline evaluation: after performing the first model. • The second evaluation: after performing the 5th model. • The third evaluation: after performing the 10th model.
The 3 weeks retest
All of the trainees were asked to perform another anastomosis at 3 weeks after the end of the training program. During this interval, the trainees had no access to any laparoscopic training. This test was done to examine the consolidation of the gained skills.
Statistical analysis
A progression curve was plotted for each trainee for each task. The data were collected and analyzed by the Student t-test with the p<0.05 considered statistically significant. All tests were done by the computer software SPSS 17.0 for Windows® (Chicago–IL).
Results
The ten urology residents who were involved in this laparoscopic course had successfully completed it and the results of the questionnaire that obtained at its end showed that all of them were very satisfied about it. All of the trainees encountered some difficulties in the beginning of performing each task, but a marked improvement was noticed with the repeated training. Most of the trainees reached the proficiency level (Table 1) in each task (the criteria of the proficiency level was predetermined based on the three expert's performance) after completing the preplanned training hours. However, the trainee number 8 needed an additional hour in the peg transfer exercise and the trainee number 3 needed one more hour in the disc cutout task. Meanwhile, the trainees number 5 and 10 in the 1st task and 6 and 10 in the 2nd one reached the proficiency level earlier before the end of the corresponding session. Regarding, the extracorporeal knotting, the trainees number 4 and 10 reached the proficiency level before the end of the session, while the trainees number 6 and 7 needed an additional hour. In the intracorporeal knotting, the trainees number 1 and 4 needed an additional hour. In addition, we have also noticed that there was a significant difference in the time required to perform each task (first 4 tasks) between the initial trials and the last ones (p=0.000) (Table 2).
The five latex gloves models were successfully completed by all trainees with some difficulties that were related to the cut in the gloves by introduction of the needle. The analysis of the collected data from the sheep intestine model revealed that, after performing 5 models, both the time and the amount of leakage decreased significantly compared to the baseline (time: from 116±6.5 minutes to 85.5±5.75 minutes, p=0.000) (amount of leakage: from 21.5±2.01 mL to 6.16±1.75 mL, p=0.000) for all trainees. In addition, a significant decrease in these 2 parameters was also detected when we compared the results of the 10th model to those of the 5th one (p=0.000). On the other hand, the results of the 3 weeks retest were close to those of the 10th model with no significant difference between them regarding the time (p=0.198) and the amount of leakage (p=0.076

Percentage of change in the time and leakage compared to the base line.
Discussion
The use of pelvitrainer is not new in the field of laparoscopic training, but in this study, we tried to use it in a more comprehensive protocol for the basic training of junior urologists. We designed this protocol to be of increasing complexity with continuous subjective and objective evaluation of the trainees to get the maximum benefit from this apparatus. Our protocol was applied to a homogenous group of trainees with no previous laparoscopic experience to enable us to do a sound comparison between them. On the other hand, because of the continuous availability of the pelvitrainer in our department, we preferred to use an extended course with a distributed pattern of training. The distributed practice pattern has the advantage of avoiding the mental and the physical fatigues that started after one to 2 hours of continuous practice. In addition, the consolidation of the learned material during breaks gives the participant sufficient time for mental rehearsal and better long-term retention compared to the massed practice. 16,17
The initial part of our training protocol (the first 4 inanimate tasks) was directed to help the trainee to work in a two–dimensional image monitor and to get the manual dexterity and the coordination needed for laparoscopic surgery. We also used both subjective and objective evaluations in each experiment to make sure that the trainees had successfully passed it. The same evaluation was previously reported by Scott et al. and Vassiliou et al. in similar experiments. 18,19 On the other hand, in the curriculum of our program, we dedicated one training session for each of these tasks and our results showed that, most of the trainees reached the proficiency level within this period. This observation suggests that, the preplanned time in this study is sufficient to master these techniques and this can be applied safely in the future protocols.
The next part of our program involved the two models of the L-UVA. We started with the latex glove model because of its simplicity and to make the trainees more familiar with the procedure. However, although a similar model was described before for laparoscopic pyeloplasty training, these models lack reality with inability to get a good objective evaluation of the quality of the anastomosis. 20 On the other hand, when the participants had completed the five sessions of the latex glove experiment, they started the sheep intestine model. This model was also previously described by Boon et al. and it avoids the drawbacks of the previous model as it imitates the human tissue and it gives the impression of a real-life laparoscopic urethrovesical anastomosis. 21 In this task, we evaluated the trainees by the time needed to complete the anastomosis and by the amount of leakage after its completion. However, the analysis of the learning curve of the trainee showed that the improvement in the quality of the anastomosis was achieved before the improvement in the time needed to complete it. We have noticed that the anastomosis was of good quality after performing 4–6 models, while the time became acceptable after 8–10 models. This observation was also reported by Nadu et al. who used a similar model and they explained it by the need of the trainees to consume much time in the early trials to improve memorization of the procedure steps and to enhance their manual dexterity. The acquisition of these skills by the participants resulted in a significant improvement of the quality of the anastomosis that was evident after about five models. Thereafter, the steps were performed in an automatic fashion resulting in a significant reduction of the consumed time in the late trials. 12
On the other hand, we have used this experiment not to make these junior trainees able to do the anastomosis in the living patients, but as a method of training to get the basic laparoscopic skills. In this task, we noticed that all of the trainees were insisting on completing the anastomosis despite the considerable difficulty of the early ones and this represented a great challenge to them. In addition, there was an obvious improvement in the performance of the participants in the late experiments compared to the early ones. Therefore, it was clear to us that, the addition of this experiment after the initial inanimate tasks was greatly beneficial to the trainees. This can be attributed to the need of the participant to get the right angle and the right direction of the needle to have a good suturing and to avoid tearing of the intestine. 22
At the end of this program, we wanted to see if the trainees were able to retain the acquired skills after a period of no training as proposed by previous studies. 23 Therefore, we repeated the sheep intestine model after a period of 3 weeks of no laparoscopic training. This re-evaluation test showed no significant differences between its results and those of the last experiment (10th model). This gave us a clue about the retention of the acquired skills after our proficiency-based distributed protocol, but as a matter of fact, continuous training is mandatory for any laparoscopic surgeon to keep and improve his skills.
Finally, at this point, we do not know the impact of our training program on the surgical performance of these trainees in real-life laparoscopic surgery. However, in the literature, there is some controversy about the relationship between the degree of in vitro training and laparoscopic performance in vivo. For example, Scott et al. showed that this training significantly improve the performance of laparoscopic cholecystectomy. 4 On the other hand, Traxer et al. demonstrated that intensive laparoscopic training did not improve the overall performance during laparoscopic nephrectomy in the porcine model. 24 Therefore, more studies are needed to see the impact of this extended training protocol on the surgical performance of the participants. Moreover, we may try to compare the surgical performance the junior residents after this program to that obtained in another group who had completed another shorter training program.
Conclusions
The use of the two described models of the L-UVA after perfection of the inanimate tasks in the pelvitrainer could lead to an additional improvement of the basic laparoscopic skills of the junior urologists. Meanwhile, the application of this progressive extended protocol can help the trainees to retain the acquired skills.
Footnotes
Disclosure Statement
No competing financial interests exist.