
Abstract
Background and Purpose:
Use of metallic stents (Resonance) has been reported in the literature to be effective in relieving extrinsic obstruction in adults. Successful patency rates have been reported to be around 83.3%. The use of Resonance stents in children has not been reported. We present our experience with these stents in addressing extrinsic ureteral obstruction in the pediatric population.
Patients and Methods:
We identified two patients who underwent placement of Resonance stents for extrinsic compression at the Children's Hospital of the University of Pittsburgh Medical Center. The first patient is a 12-year-old girl with a solitary left kidney who had a diagnosis of pelvic rhabdomyosarcoma; she was treated with surgery followed by adjuvant chemoradiation. Two years post-treatment, worsening renal function secondary to ureteral strictures developed. The second patient is a 14-year-old girl with a history of Gardner syndrome. Recurrent desmoid tumors developed in her pelvis and retroperitoneum that led to right ureteral obstruction, necessitating a nephrostomy tube.
Results:
Both patients underwent successful technical placement of a Resonance stent. The time to failure for patient 1 was 3 months and for patient 2, 3 weeks. The first patient presented to the emergency department 3 months poststent in renal failure with a creatinine level of 13.7 mg/dL. This necessitated nephrostomy tube placement and hemodialysis. Ultimately, she needed an ileal ureter to preserve renal function. She is off hemodialysis and has a creatinine level of 2.2 mg/dL.The second patient, recurrent episodes of pyelonephritis, worsening hydronephrosis, and flank pain developed with just the Resonance stent in place. It was elected to remove the Resonance stent and replace the nephrostomy tube. She needed extensive ureterolysis, a right subtotal ureterectomy with a right to left ureteroureterostomy.
Conclusion:
We did not find the use of these stents to be effective in children. The time to failure was significantly shorter in children than those reported in the literature for adults.
Introduction
Management options include nephrostomy tube placement, polymeric ureteral stents, and metallic stents. Nephrostomy tube placement has been shown to affect the quality of life of patients. 1 Polymeric stents have a major complication rate of 34%, failure rate of 36%, with a mean indwelling time of 95 days. 2
Resonance® metallic double pigtail ureteral stents (Cook Medical, Bloomington, IN) have been introduced as a potential solution to this difficult problem of extrinsic ureteral obstruction for up to 12 months. 1 The metallic coil design is recalcitrant to compressive forces, and approximately 25 times more force is needed to occlude it compared with a plastic stent. 3,4 Others have reported benefits including improved patient comfort, higher patency and drainage rates. Reported success rates in the literature range between 51.2% and 100%. 3
The reported success of Resonance stents has been established in the adult population; however, there have been no reports on the treatment of extrinsic compression in the pediatric population. We present our experience with use of Resonance stents in the treatment of extrinsic ureteral compression in the pediatric population.
Patients and Methods
After receiving Institutional Review Board approval, we identified two patients who underwent placement of Resonance metallic stents for extrinsic compression at the Children's Hospital of the University of Pittsburgh Medical Center between the years 2005 and 2010.
Resonance stents were placed in a retrograde fashion following instructions recommend by Cook Medical.
Briefly, under anesthesia, the patient is placed in a dorsal lithotomy position. Under cystoscopic guidance, a 0.035-inch floppy wire is placed into the collecting system under fluoroscopic guidance. Then a coaxial system, which includes an outer 9F introducer sheath and an inner 5F ureteral catheter is passed over the guidewire and into the renal pelvis. 1 The outer sheath is then kept in place and the guidewire and the 5F inner sheath are removed. The Resonance stent is pushed through the introducer sheath using the inner sheath as a pusher. After the proximal curl is formed in the renal pelvis, the introducer sheath is retrieved with the pusher catheter held in place until the distal pigtail curl is deployed in the bladder. 1
Our first patient was a 12-year-old girl with pelvic rhabdomyosarcoma who was treated with extirpative surgery followed by adjuvant chemotherapy and radiation. She had a solitary left kidney. Two years post-treatment, worsening renal function secondary to ureteral strictures developed. Her stricture disease was attributed to retroperitoneal fibrosis from surgery, chemotherapy, and radiation. During a 4-month period, her obstruction was managed with a Resonance stent that failed on two occasions, resulting in acute renal failure necessitating hemodialysis and nephrostomy tube placement.
The second patient was a 14-year-old girl with a history of Gardner syndrome who has undergone multiple small bowel resections. She has had recurrent desmoid tumors in the pelvis and retroperitoneum that had led to right ureteral obstruction. She has had multiple recurrent episodes of right pyelonephritis with worsening hydronephrosis and pain. This ultimately led to nephrostomy tube placement. Because of extrinsic compression, she underwent placement of a Resonance stent and removal of the nephrostomy tube.
Within 3 weeks, she continued to have significant right flank pain, recurrent episodes of pyelonephritis, worsening hydronephrosis, and renal function that necessitated reinsertion of a nephrostomy tube and removal of the stent.
Results
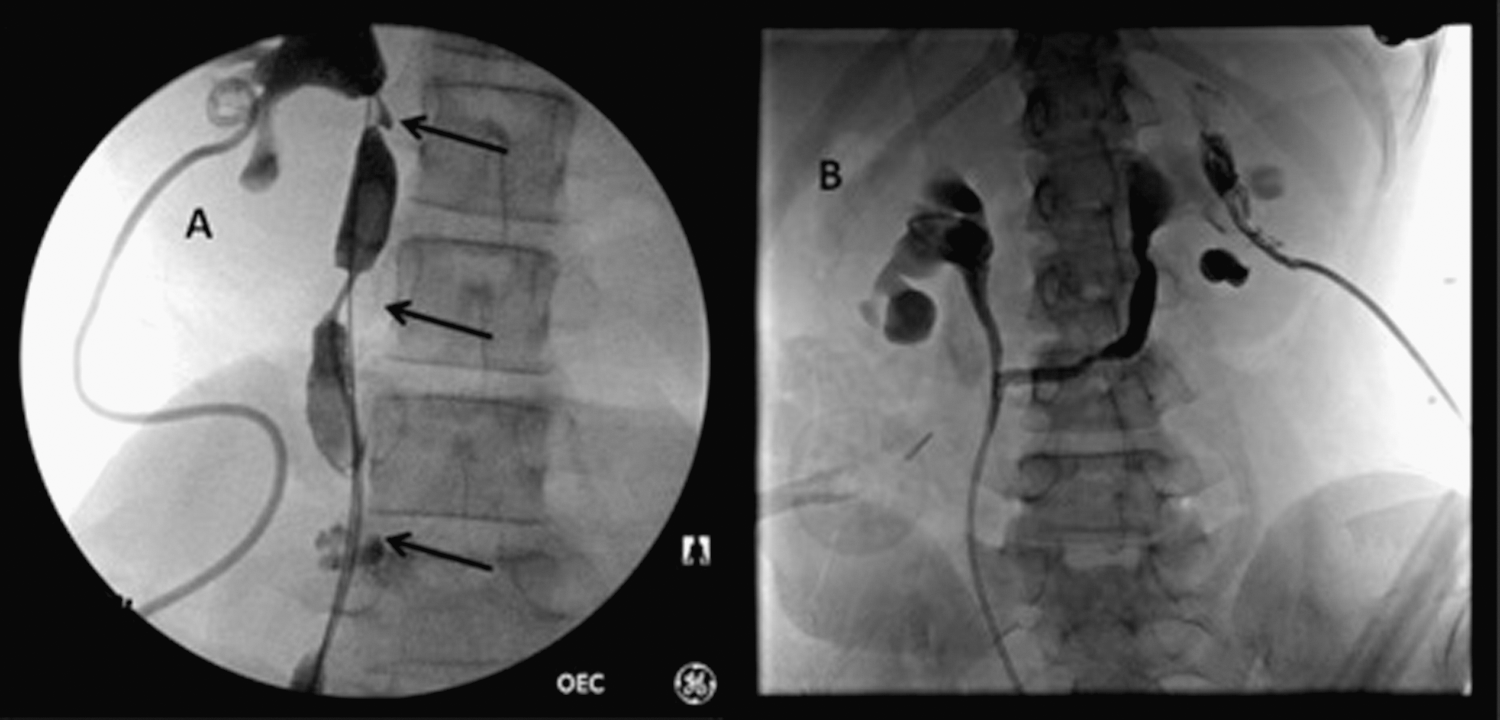
Both patients underwent successful technical placement of a Resonance stent (Fig. 1). The time to failure for patient 1 was 3 months and for patient 2, 3 weeks. Patient 1 presented with acute renal failure, necessitating hemodialysis and placement of a nephrostomy tube for decompression. Patient 2 presented with worsening hydronephrosis and increased flank pain.

Successful resonance stent placement:
The first patient presented to the emergency department 3 months poststent placement in renal failure with a creatinine (Cr) level of 19.7 mg/dL and with a blood urea nitrogen value of 146. This necessitated immediate nephrostomy tube placement, which dropped her Cr level to 5.8 mg/dL. Ultimately, she needed ureteral reconstruction with ileum to preserve renal function in her solitary kidney. She is off hemodialysis and has a creatinine level of 2.2 mg/dL.
In the second patient, recurrent episodes of pyelonephritis, worsening hydronephrosis, and significant flank pain developed with the Resonance stent in place. It was elected at that time to remove the Resonance stent and keep her renal system decompressed with a nephrostomy tube. She ultimately needed extensive ureterolysis, a right subtotal ureterectomy with a right to left ureteroureterostomy (Fig. 2).
Discussion
The use of metallic stents to relieve mechanical obstruction in children has not been described in the literature. This is most likely because of the rarity of this form of obstruction in children and the long-term requirement for indwelling stents.
The adult literature describes multiple treatment strategies for the relief of extrinsic compression. Rotariu and associates 5 describe the placement of two double-pigtail ureteral stents to aid in the expansion of the ureter. They double-stented ureters with either two 7F stents or a combination of 8F/6F Double-J ureteral stents after their single stent placement had failed. After follow-up of 16 months, they reported significant improvement of hydronephrosis and kidney function. Other treatment options include the placement of nephrostomy tubes, which in adults is associated with a decreased quality of life. 6 In children, the same holds true.
Conventional plastic stents have been reported to have a failure rate between 35% and 50%. Docimo and Dewolf 7 reported a 44% stent failure rate in the first 30 days of stent insertion in patients with extrinsic obstruction.
Chung and colleagues 8 reported on their 15-year experience of the management of extrinsic compression with ureteral stents. With a mean follow-up of 11 months (range 1–127 mos), in 101 patients with 138 ureteral units with stents, 58 (42%) failed. Of the failures, 25 happened within 6 days of placement.
The advantage of metallic stents is their ability handle greater radial forces than the conventional plastic stents. Cook Medical says that the metallic Resonance stent was found to maintain its flow rate with up to 1000N exerted by an external pressure point load in a ex-vivo artificial model ureter system; when testing traditional plastic stents, flow rates were markedly diminished at 30 N (unpublished data).
Wang and coworkers 1 reported their experience with metallic Resonance stents. In 19 patients, with a total of 22 stents inserted, they reported a patency rate of 77.3% at 5-month follow-up.
Others have reported the use of metallic stent placement for the management of ureteral obstruction. Modi and colleagues 3 conducted a multi-institutional retrospective study of the use of metallic stents. Seventy-six stents were placed in a total of 59 ureteral units. Of the 59 renal units, 44 were obstructed from malignancy. Only 15 of the 41 metallic stents that were placed secondary to failed plastic stents became obstructed. Of those who had secondary metallic stents placed, 37% become reobstructed. With the median follow-up time to obstruction 1.5 months, 43% of stents were removed before 1 year. 3
In their series, describing 50 patients with malignant and benign obstructions, Liatsikos and associates 4 reported at 11 and 6.8 months follow-up a patency rate of 100% for malignant and 44% for benign obstruction. Twenty-five stents were placed for malignant obstruction, 18 for benign, 7 for an obstructed metal mesh stents placed for ureteroenteral stricture disease. They reported no complications and 100% technical success rate.
With metallic ureteral stents established as formidable option for the treatment of extrinsic compression in adults, the use in children has not been reported.
Most of the literature in regard to obstruction and the use of stents in the pediatric population is related to failed pyeloplasties and/or antireflux surgery. This is most likely secondary to the rarity of pediatric extrinsic ureteral obstruction. Benign obstruction in children is mostly related to correctable embryologic abnormalities. Thus, the use of metallic stents or chronic indwelling ureteral stents for the management of obstruction is rare.
For those disease processes that do cause ureteral obstruction, such as familial adematous polyposis disease (FAP), treatment has been with the use of ureteral stents and pharmacologic therapy. Joyce and coworkers 9 reviewed their prospectively collected database of 107 patients with FAP with concurrent desmoid tumors. Of the 107 patients, 30 had ureteral obstruction secondary to the development of desmoids tumors. Of these patients, 93% had undergone surgery before development of desmoid disease leading to ureteral obstruction. Eighteen patients underwent ureteral stent placement, and in 5 of these patients, nephrostomy tubes were placed with/without antegrade stent insertion for failure of the stent. Four patients underwent nephrectomy, and one patient underwent a reimplant with construction of a Boari flap. One-third of the patients underwent more than one procedure to help alleviate obstruction.
There are several shortcomings of our study, the first being the small size of our cohort. Extrinsic obstruction is rare in children, and thus obtaining a sufficient cohort to statistically define a success rate may not be feasible. Thus, our experience with two patients may not be a large cohort, but our intent is to describe our experience with the use of metallic stents in the pediatric population. At this time, we would not recommend the use of metallic stents in the treatment of pediatric extrinsic compression without close follow-up and awareness that a secondary procedure will be needed to manage the obstruction.
We also understand that because of our small cohort, these two events could have occurred by chance. With the relatively short time to failure of the stents, however, these failures were most likely related to the lack of effectiveness of the stents rather than by chance. We acknowledge that in order to determine whether the use of metallic stents in the setting of pediatric extrinsic compression should be considered an effective treatment, a multi-institutional study may be necessary.
Conclusion
We report our experience with metallic stents in the treatment of extrinsic compression in the pediatric population. The use of metallic stents had 100% failure rate, and patients needed further treatments to alleviate the obstruction. The incidence of pediatric ureteral obstruction secondary to extrinsic compression is rare; however, we must develop more effective means of being able to manage these problems. Further research and development is needed to develop effective stents for the treatment of extrinsic compression in the pediatric population.
Footnotes
Disclosure Statement
No competing financial interests exist.