
Abstract
Background and Purpose:
The EMS Swiss LithoBreaker is a new, portable, electrokinetic lithotripter. We compared its tip velocity and displacement characteristics with a handheld, pneumatic lithotripter LMA StoneBreaker.™ We also evaluated fragmentation efficiency using in vitro models of percutaneous and ureteroscopic stone fragmentation.
Materials and Methods:
Displacement and velocity profiles were measured for 1-mm and 2-mm probes using a laser beam aimed at a photo detector. For the percutaneous model, 2-mm probes fragmented 10-mm spherical BegoStone phantoms until the fragments passed through a 4-mm mesh sieve. The ureteroscopic model used 1-mm probes and compared the pneumatic and electrokinetic devices to a 200-μm holmium laser fiber. Cylindrical (4-mm diameter, 4-mm length) BegoStone phantoms were placed into silicone tubing to simulate the ureter; fragmented stones passed through a narrowing in the tubing.
Results:
For both 1-mm and 2-mm probes, the electrokinetic device had significantly higher tip displacement and slower tip velocity, P<0.01. In the percutaneous model, the electrokinetic device needed an average of 484 impulses over 430 seconds to fragment one BegoStone, while the pneumatic device needed 29 impulses over 122 seconds to fragment one stone. Both clearance times and number of impulses needed for percutaneous stone clearance were significantly different at P<0.01. Ureteroscopically, the mean clearance time was 97 seconds for the electrokinetic lithotripter, 145 seconds for the pneumatic lithotripter, and 304 seconds for the laser. Comparing the pneumatic device with the electrokinetic device ureteroscopically, there was no significant difference in clearance time, P=0.55. Both the pneumatic and electrokinetic lithotripters, however, demonstrated decreased clearance times compared with the laser, P=0.027.
Conclusions:
The portable electrokinetic lithotripter may be better suited for ureteroscopy instead of percutaneous nephrolithotomy. It appears to be comparable to the portable pneumatic device in the ureter. Further clinical studies are needed to confirm these findings in vivo.
Introduction
The EMS Swiss LithoBreaker (EMS, Nyon, Switzerland) is a new cordless, handheld electrokinetic lithotripter (Fig. 1). The LMA StoneBreaker™ (Laryngeal Mask Airway [LMA] Company, Switzerland; distributed by Cook Medical, Bloomington, IN) is a pneumatic lithotripter that is also portable and activated by a hand switch.

EMS Swiss Lithobreaker, a new portable, electrokinetic lithotripter.
We performed bench testing to quantify the basic physical parameters of the two lithotripters to establish a baseline for comparison and to see how these characteristics may impact stone fragmentation. Specifically, probe tip velocity and displacement were evaluated. We also compared in vitro fragmentation with both devices, using percutaneous and ureteroscopic models.
Materials and Methods
Lithotrite comparison
Technical specifications of the two lithotripters are compared in Table 1. 1,2
Tip dynamics
An optical system evaluated the probes in a noncontact manner (Fig. 2). Our method for measuring tip displacement and tip velocity has been described previously. 3 Briefly, the lithotripter is fixed to the benchtop in a customized frame, perpendicular to an expanded laser beam. The tip of the lithotripter is aligned so that its movement will partially occlude the laser beam aimed at a high bandwidth photo detector. Because there is a linear correlation between tip displacement and reduction in transmitted voltage from the laser beam, the measured voltage from the photo detector can then be converted to tip displacement values. Twenty-five displacement profiles of tip velocity and tip displacement were measured for 1-mm and 2-mm probes with each device.
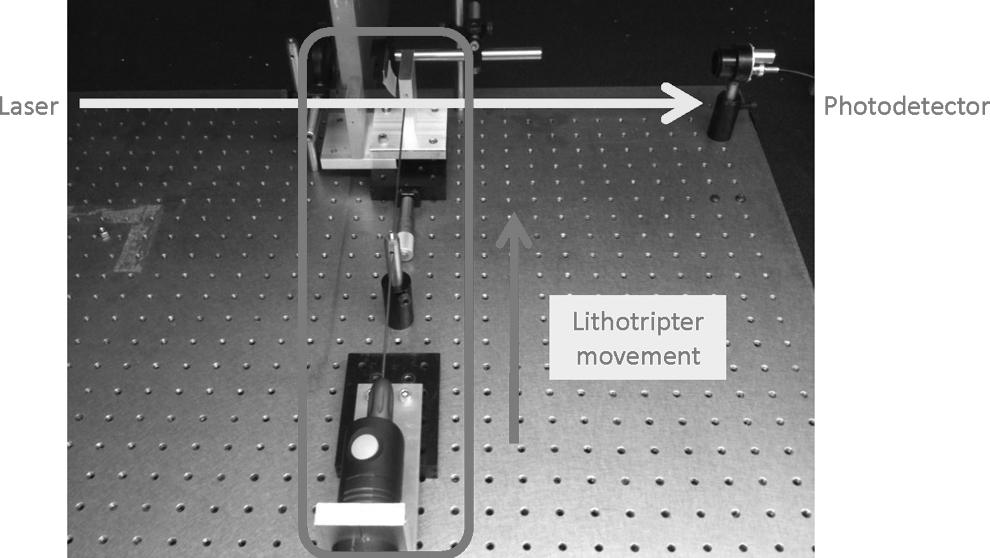
Measurement of tip dynamics with the benchtop optical system.
Percutaneous model
To simulate the contained space of the intrarenal collecting system, a 1-cm spherical BegoStone phantom was placed inside a vertical 20-mL syringe. The bottom of the syringe was removed and a 4-mm mesh sieve placed under the syringe (Fig. 3). With the 2-mm probe for both devices, the stone phantoms were fragmented under water by two endourology fellows. The time needed for all stone fragments to pass through the sieve was measured as stone clearance time. The number of impulses and time needed to clear each stone were recorded over four trials, with one stone fragmented in each trial.

In vitro model of percutaneous stone fragmentation, through a 4-mm mesh sieve.
Ureteroscopic model
This comparison used the 1-mm probes for the electrokinetic and pneumatic lithotripters. In addition, a 200-μm Flexiva™ laser fiber (Boston Scientific, Natick, MA) combined with a 100 W VersaPulse® PowerSuite™ laser (Lumenis Surgical, Santa Clara, CA) at settings of 0.2 J and 50 Hz served as a baseline for comparison. These laser settings were chosen because they are our standard settings for the management of ureteral stones. The ureter was simulated with a length of silicone tubing, and a cylindrical BegoStone phantom (4 mm diameter×4 mm height) served as an impacted ureteral stone. The silicone tubing was narrowed to approximately a 2-mm diameter, distal to the stone (Fig. 4). Stone clearance time was defined as the time for all fragments to pass by the narrowing. Five trials, in which one stone was fragmented per trial, were conducted with each instrument.

Diagram of in vitro ureteroscopic model for stone fragmentation.
Means and standard deviations were computed for all groups. An unpaired two-tailed Student t test or one-way analysis of variance were used when appropriate, with the GraphPad Prism version 5.00 for Windows, GraphPad Software, San Diego, CA.
Results
Tip dynamics
Compared with the pneumatic device, the electrokinetic device had a higher tip displacement and slower tip velocity for both probe sizes (Fig. 5). Mean tip displacement for the pneumatic lithotripter was 0.7443 mm and 1.219 mm for the electrokinetic lithotripter when tested with the 1-mm probe, P<0.01. Mean tip displacement for the pneumatic lithotripter was 1.381 mm and 2.135 mm for the electrokinetic lithotripter when tested with the 2-mm probes, P<0.01. With the 1-mm probes, mean tip velocity for the pneumatic device was 33.93 m/s and 18.09 m/s for the electrokinetic device, P<0.01. With the 2-mm probes, mean tip velocity for the pneumatic lithotripter was 36.66 m/s and 19.43 m/s for the electrokinetic lithotripter, P<0.01. A greater variation in displacement and velocity was observed with the pneumatic device.
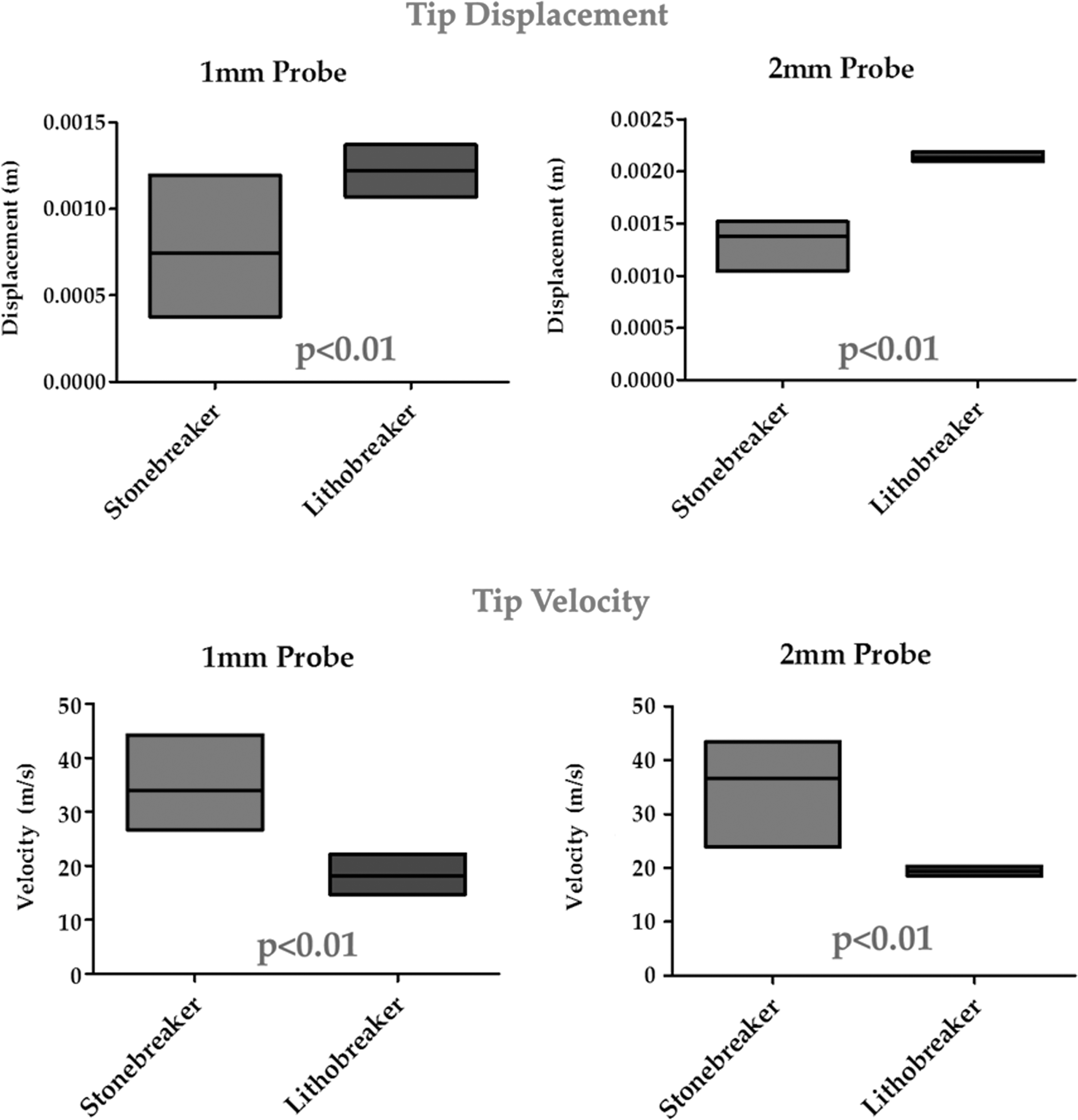
Benchtop testing results of tip dynamics.
Percutaneous model
For the pneumatic lithotripter, the mean number of impulses needed to fragment the stones to less than 4 mm diameter was 29±3.7 impulses. For the electrokinetic lithotripter, this needed an average of 430±97 shocks, P<0.01. The time needed to stone clearance was also significantly different. The pneumatic lithotripter needed an average of 122±56 seconds compared with the electrokinetic lithotripter's 484±79 seconds to clear the stones, P<0.01.
Ureteroscopic model
Both the electrokinetic and pneumatic devices compared favorably with the 200-μm holmium laser (Table 2). The average stone clearance time for the pneumatic device was 142.6±121.3 seconds, for the electrokinetic device 97.4±26.7 seconds, and for the holmium laser 304.4±99.9 seconds. In evaluating the pneumatic device against the electrokinetic device, the pneumatic device needed more time for stone clearance at 142.6 seconds compared with the electrokinetic's 97.4 seconds, despite needing fewer shocks to clear the stone (mean of 33.2±19.8 shocks for the pneumatic and 178.2±54.1 shocks for the electrokinetic devices). Stone clearance time for the pneumatic lithotripter included the time needed to change one CO2 cartridge. The time needed to change one cartridge was 70 seconds. The difference in stone clearance time between pneumatic and electrokinetic devices was not statistically significant, P=0.55. When comparing all three groups, however, the pneumatic and electrokinetic clearance times were both significantly less than the laser, P=0.027.
Discussion
Rigid intracorporeal lithotripters can be used with both ureteroscopy (URS) and percutaneous nephrolithotomy (PCNL). The pneumatic Stonebreaker has been demonstrated to be efficacious and safe in both of those approaches. Rané and associates 4 described their percutaneous, ureteroscopic, and intravesical experience with the Stonebreaker in a multicenter, prospective trial. Nerli and colleagues 2 also published their experience with the StoneBreaker in URS. Both trials found this handheld pneumatic device to be safe and efficacious. A prospective randomized trial comparing the Stonebreaker with the Swiss LithoClast Classic and 350-μm laser fiber with semirigid distal URS found similar rates of stone clearance, retropulsion, stone-free status, and complications between the groups. 5
Our study is the first report on the LithoBreaker, a novel portable electrokinetic intracorporeal lithotripter. Because the Lithobreaker is similar to the pneumatic StoneBreaker in terms of portability and possible indications for semirigid URS and PCNL, establishing basic physical parameters is useful for baseline comparison. Our testing demonstrates that the power source and design of both instruments impact the tip dynamics. The pneumatic lithotripter demonstrated much more variability in velocity and displacement, most likely related to the depletion of the CO2 cartridge. The electrokinetic device was much more consistent, because of the steady and long-lasting power supply from the batteries. As the battery wanes, the time needed to generate the energy to propel the tip increases, but the tip velocity and tip displacement stay constant.
We did not observe any noticeable decrease in the deployment rate, however, when operating the device across multiple trials. Its 6×higher impulse frequency also provides greater power (energy/time) delivery compared with the pneumatic lithotripter. The electrokinetic lithotripter had a slower tip velocity but higher tip displacement compared with the pneumatic lithotripter. This result was consistent with both 1-mm and 2-mm probe diameters. Higher tip displacement may theoretically increase the probability of stone retropulsion, and a slower tip velocity may produce smaller stone fragments that are easier to pass. We then attempted to see how these results translated with in vitro testing.
Our percutaneous model was designed to allow for stone mobility and to simulate the fact that stones in vivo can often move in the intrarenal collecting system during PCNL. The electrokinetic device needed a significantly higher number of shocks to clear a stone. This may in part be attributed to the electrokinetic device's lower tip velocity and its continuous impulse mode. The continuous delivery at 3 Hz allows for more power to be delivered to large semifixed stones. In our percutaneous model, however, the stone was mobile and impulses were delivered even when the device was not directly targeted on the stone.
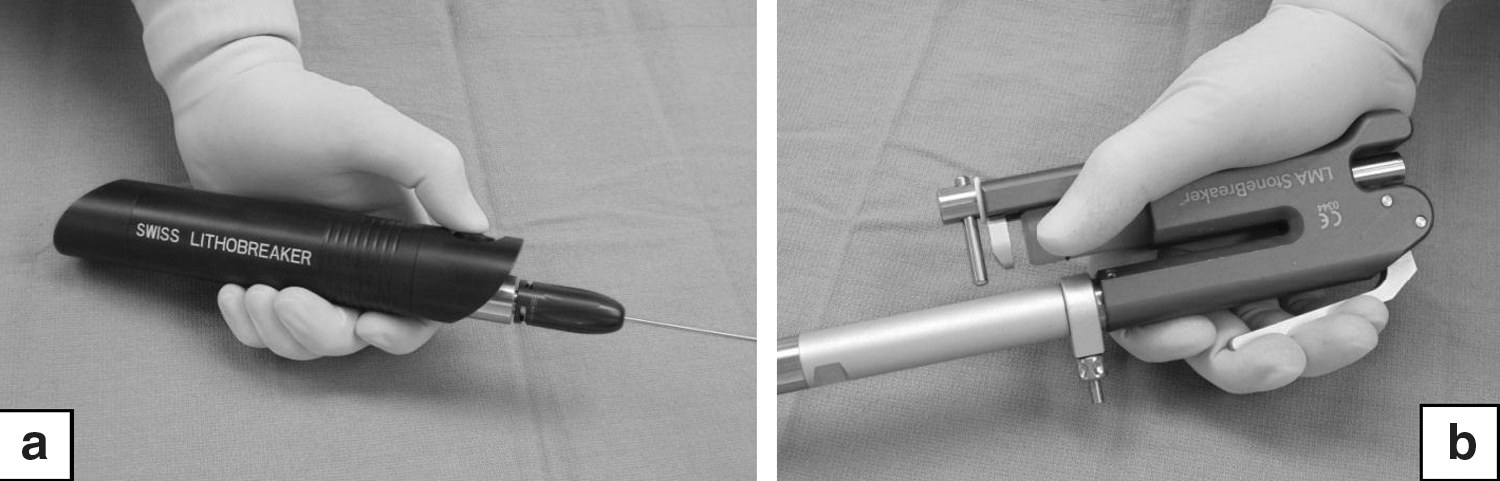
While the pneumatic lithotripter had more variable tip dynamics at the benchtop, it fragmented a mobile stone much more easily in the percutaneous model. While tip dynamics can partially explain this, another major factor was that the pneumatic lithotripter was less fatiguing to use because of ergonomic factors. The placement of the deployment button on the handpiece of the electrokinetic lithotripter caused more hand and arm fatigue. The operator's hand had to form a “thumbs-down” sign. This was not an issue for the pneumatic lithotripter, because the device could be operated by easily squeezing the handle (Figs. 6a, 6b). Another notable difference was that the pneumatic lithotripter could fragment a stone by placing it near the stone. In contrast, the electrokinetic lithotripter needed firm pressure and direct contact on the stone to cause fragmentation.

Ergonomics of using the electrokinetic Lithobreaker
To evaluate each device for use during URS, we added the laser as an intracorporeal lithotripter for comparison because it is considered the gold standard for ureteral stone fragmentation. Our model used a cylindrical BegoStone impacted in a length of silicone tubing, and the stone fragments had to pass by a narrowing in the tube. This is not a typical clinical scenario, so our conclusions are tempered by the limitations of this model. With the stone in a confined space, the electrokinetic lithotripter did not have the same difficulties in focusing on the stone as in the percutaneous model where the stone was mobile. It had the shortest mean stone fragmentation time of 97.4±26.7 seconds, although this was not statistically significantly from the pneumatic lithotripter's mean time of 142.6±121.3 seconds. The variability in fragmentation time was most likely associated with the depleting CO2 levels in the cartridge. We saw in our tip dynamic studies that the StoneBreaker had significantly more variability in tip velocity and tip displacement, also attributed to this reason.
Perhaps most interestingly, the laser had the longest stone fragmentation time at 304.4±99.9 seconds. This finding may be because of the laser settings chosen (0.2 J and 50 Hz), which we use clinically. The BegoStone phantom used has mechanical properties similar to those of calcium oxalate monohydrate stones. Even with this type of stone, we had no tip degradation with our settings. A higher energy (J) and lower pulse frequency setting (Hz), however, may have provided faster stone fragmentation. As Sea and coworkers 6 have demonstrated, different laser power settings result in significant differences in total fragmentation, stone fragment size, and degree of retropulsion. The continuous impulse design may have also favored the electrokinetic device with our model of an impacted stone. Of note, proper use of the pneumatic lithotripter necessitated a 3 second pause between each impulse to allow for CO2 levels to equilibrate. The CO2 cartridge also required one replacement over the five trials, slightly increasing stone clearance time. Even excluding the time needed to change the CO2 cartridge, however, there was no statistical difference in fragmentation time between the electrokinetic and pneumatic devices.
Other researchers have clinically evaluated ballistic lithotripters in the ureter. Bapat and associates 7 retrospectively evaluated nearly 400 patients with proximal ureteral stones treated with either the LithoClast or holmium laser. The LithoClast caused more retropulsion, at 14% compared with 2% for the laser group. Stone-free rates were better for the laser group, at 97% compared with 86% for the LithoClast, defined by radiography of the kidneys, ureters, and bladder obtained 2 weeks postoperatively. Two patients in the LithoClast group needed secondary URS to treat stones impacted in the lower ureter.
Manohar and colleagues 8 described a prospective, randomized trial of 50 patients with proximal ureteral stones treated with either the LithoClast 2 or a 200-μm holmium laser and found the two to be comparable. Stone fragmentation time and retreatment rates were not significantly different, below 10 minutes and approximately 15%, respectively. Stone retropulsion and mucosal injury rates were also equivalent. Stone-free rates were 88% for the Lithoclast 2 group and 84% for the laser group, defined by intravenous pyelography obtained 3 months postoperatively.
Most recently, Salvado and coworkers 5 conducted a prospective, randomized, controlled trial of 69 subjects with distal ureteral stones treated by a 350-μm holmium laser, the LithoClast Classic, and StoneBreaker. Mean stone fragmentation time was equivalent. Stone retropulsion rates, intraoperative complications, and need for secondary procedures were not statistically different. Stone-free rates, defined by CT obtained at postoperative day 15, were approximately 97%. The pneumatic or portable lithotripters appear to be clinically comparable to the holmium laser, but at a lower cost.
The button placement on the electrokinetic LithoBreaker was much more suited for ureteroscopic use, making it less fatiguing in this model than in the percutaneous model. The users thought that the pneumatic Stonebreaker and electrokinetic LithoBreaker were equally easy to use ureteroscopically. Because the operator's hand is below the level of the stone (ie, closer to the floor), LithoBreaker deployment did not necessitate awkward hand positioning as it did in the percutaneous model (Figs. 7a, 7b). Our results indicate that the electrokinetic LithoBreaker functions very well in our ureteroscopic model against other devices currently on the market for ureteroscopic stone fragmentation.
Ergonomics of using the electrokinetic Lithobreaker
We acknowledge several limitations of our study. Whether our models can be translated to clinical results is to be determined; our models have not been validated. Mucosal damage was not assessed, yet one might assume it would be less for the electrokinetic and pneumatic devices than for the holmium laser fiber. We also did not quantify the degree of hand fatigue, and only recorded subjective observations. We could not evaluate the degree of stone retropulsion in our in vitro model because ureteroscopic stone clearance was defined by stones passing beyond a narrowing in our silicone tubing.
Conclusions
In this initial report on a new portable lithotripter, the electrokinetic EMS Swiss LithoBreaker's tip dynamics are described and compared with a commercially available portable lithotripter, the pneumatic LMA StoneBreaker. The LithoBreaker did not seem to perform as well as the StoneBreaker in our percutaneous stone fragmentation model. Both devices, however, were equally simple to operate and fragmented stones in our obstructed ureteral stone model with similar stone fragmentation rates. Further clinical studies are needed to assess the utility of this new electrokinetic device.
Footnotes
Disclosure Statement
Dr. Lipkin is a consultant for Boston Scientific. For the remaining authors, no competing financial interests exist.