
Abstract
Purpose:
We developed a genitourinary skills training (GUST) curriculum for incoming third year medical students (MS3) and performed a follow-up study of comfort with and utilization of these skills.
Materials and Methods:
GUST consisted of a didactic lecture followed by skills sessions including standardized patient testicular examination (TE) and digital rectal examination (DRE), male and female Foley catheter (MFC and FFC) placement training, suture-knot tying, and a faculty-directed small group learning session. Precourse and postcourse, and 6 and 18 months after the course, MS3 rated comfort with each skill (Likert scale 0–5), and quantified skill usage. Results were compared with 4th year students (MS4) who had not undergone GUST.
Results:
Participants were 281 MS3 GUST students and 44 MS4. Post-GUST, mean comfort on a Likert scale (0=uncomfortable) increased for all four skills (88.2%–96.9% vs 8.3%–18.5%, P<0.0001). This was maintained at the 6-month and 18-month follow up time points (P<0.0001). At 18 months, MS3 trended toward higher comfort with TE compared with MS4 (74 vs 54%, P=0.068), while with the other skills, both groups showed equal comfort. MS4 learned exam skills from faculty and MFC and FFC from nurses on the wards. Eleven percent of MS4 were never formally taught TE or DRE. MS3 and MS4 performed TE and/or DRE on <8% of newly admitted patients.
Conclusions:
MS3 described improved comfort with the GU skills at all time points during follow-up. This was particularly important because both MS3 and MS4 reported using their skills infrequently during their clinical training years.
Introduction
Several methods have been used to fill the critical gap in the standard medical education paradigm that comes after “see one” and “do one,” just before “teach one.” The concept of “practice many” has brought with it new teaching modalities, including the use of standardized patients (SPs), simulated models, and multimedia aids, which have become validated mainstays of learning technical and examination skills. 3 –6 With practice comes comfort, which encourages more practice and continued development of these skills.
At the University of California, Irvine (UCI), an intensive month of basic skills training and preparation for clinical clerkship has been developed for medical students at the end of their second year of medical school training. As part of this preparatory course, a dedicated two-day GU skills training (GUST) curriculum was designed to provide students with training in the basic urology skills expected of all medical students on the clinical wards. The immediate impact of the course on comfort with GU skills was evaluated previously. 7 This resulted in modifications of the curriculum to provide a more efficient and cost-effective curriculum. The current study evaluates the long-term impact of this curriculum on both student comfort level and use of these new skills throughout their clinical medical school career.
Materials and Methods
The GUST curriculum was designed as a two-day adjunct to the month-long Clinical Foundations III (CF-III) course at the UCI School of Medicine. The CF-III course was developed by the Office of Educational Affairs to help new third year medical students (MS3) transition their cognitive knowledge of basic science courses and their nascent history and physical examination skills to application at the bedside during the clinical clerkship years. The details of the curriculum have been described. 7 The virtual reality cystourethroscopy station was discontinued during the second year of the curriculum, because it was the lowest rated in utility with the highest associated cost. In its place, a suturing workshop was added because students indicated they wanted more practice of this surgical skill. This study was approved by the Institutional Review Board at the University of California, Irvine. The course was required, and precourse and postcourse questionnaires were collected. Briefly, the course was structured as follows:
Course objectives
The GUST curriculum was designed to teach both the basic elements of the male GU examination and bladder catheterization for male and female patients. The learning objectives of the GUST curriculum were to (1) demonstrate Foley catheter placement in a male (MFC) and female (FFC) inanimate model while describing pertinent urethral and bladder anatomy, (2) perform a GU examination of the testes and prostate in a male SP, (3) discuss abnormal findings that may be encountered on testicular examination (TE) and on digital rectal examination (DRE).
Teaching strategies
During the first day of the GUST curriculum, MS3 attended a 90-minute didactic session led by a senior faculty member of the department of urology (EMM) that included a PowerPoint™ presentation of the normal anatomy of the male and female GU tracts, the technique of the TE and DRE, as well as MFC and FFC placement. Video demonstrations of MFC and FFC were included in this lecture. An opportunity for questions and discussion of the material presented was provided at the conclusion of the didactic presentation.
The class was randomly divided into two groups of equal size, and each group was designated a specific time to attend on the next 2 consecutive days for the skills training portion and second part of the GUST curriculum. On each day of the skills training sessions, the group was divided into small groups of eight to 10 students, and each small group rotated through five skills training stations. The students had 45 minutes at each station for a total of just less than 4 hours. A total of 12 faculty, senior residents, or fellows participated in the teaching sessions.
Standardized patient DRE and TE
With a urology faculty-to-student ratio of 1:1 or 1:2, MS3 were instructed and performed a TE and DRE of the SP. Eight SPs and eight faculty volunteers were required for each session. These patients were well trained and provided feedback to the students as to the performance of their examination during the session. In addition, the faculty teachers provided direct supervision and guidance.
During the instruction, the urology faculty, senior resident, or fellow led a discussion of abnormal GU findings in the testis and rectum that might be encountered during a GU examination. The students were provided an opportunity to ask questions and explore areas of the GU skills training to better understand the procedures and possible clinical findings.
MFC and FFC placement in a silicone model
Each student was instructed and performed, using proper sterile technique, MFC and FFC placement on a silicone model (Limbs & Things, St. Phillips, Bristol, United Kingdom) under supervision by a urology faculty, senior resident, or fellow.
Suturing and knot tying
A urology faculty, senior resident, or fellow led a group tutorial in basic suturing and knot tying skills with opportunity to practice after each demonstration.
Curriculum evaluation
On the first day of the course, before the didactic lecture, all participants filled out a binary questionnaire asking if they had experience with different aspects of GU care and examination. This included MFC and FFC placement, TE, and DRE. If they answered yes to any of the questions, they were asked to rate how comfortable they were with each procedure on a five-point Likert scale. 8,9
At the completion of the skills training sessions, participants were asked to complete a course evaluation in which they rated the usefulness of each station and evaluated the faculty who taught the sessions. They were also asked to reevaluate their comfort level with the four clinical skills of MFC and FFC placement, TE, and DRE, using the same Likert evaluation scale. Mean comfort level with each skill before the session was compared with the comfort level after the session using a Student unpaired t test (SPSS v17.0) with significance set at P<0.05.
Six months after the course, the same students filled out a questionnaire regarding their comfort with GU skills. If they were uncomfortable (Likert item<3), they were prompted as to why. In addition, they were asked to quantify their use of each of the skills on the clinical wards by defining the number of history and physicals performed in the preceding month and the percentage of DREs and TEs done. The course took place for three separate and evaluable MS3 classes, once in 2008, in 2009, and in 2011. The first class of MS3 also filled out an 18-month questionnaire, with the same questions. Lastly, students from the 2008 fourth year class (MS4), who had not previously undergone a GUST curriculum, were asked the same comfort questions with the addition of a prompt to elicit from whom they were taught each of the skills and during which clinical rotation.
Results
Ninety-six MS3 participated in the 2011 GUST session, and all (100%) completed a pre-GUST questionnaire while only 90 (94%) completed the post-GUST questionnaire. In 2009, 94 MS3 participated in the GUST session, and all completed the pre-GUST questionnaire, while 86 (91.5%) completed the post-GUST questionnaire. A total of 281 MS3 participated in the GUST curriculum from 2008, 2009, and 2011. Of the 281 MS3 students who participated, 100% completed the pretraining questionnaire and 260 students (92.5%) responded to the post-training questionnaire. One hundred students (54.1%) submitted the 6-month follow-up online questionnaire. Thirty-five of the 94 (37.2%) GUST 2008 students also completed an 18-month follow-up survey. Forty-four MS4 who had never undergone GUST completed a GU skills comfort assessment.
The number of students reporting on their comfort with MFC and FFC placement, DRE, and TE over time is shown in Table 1 with the mean comfort scores graphed in Figure 1. Before GUST, the participating medical students reported an average comfort score of 0.54 to 0.83 out of 5 on a Likert scale with 0 representing “not at all comfortable” and 5 “completely comfortable” with performing the four GU skills. Twenty-eight students (10.0%) had previously performed a TE on a patient, 37 (13%) had performed a DRE, 6 had FFC placement experience, and 6 had performed MFC placement (2.0% each).
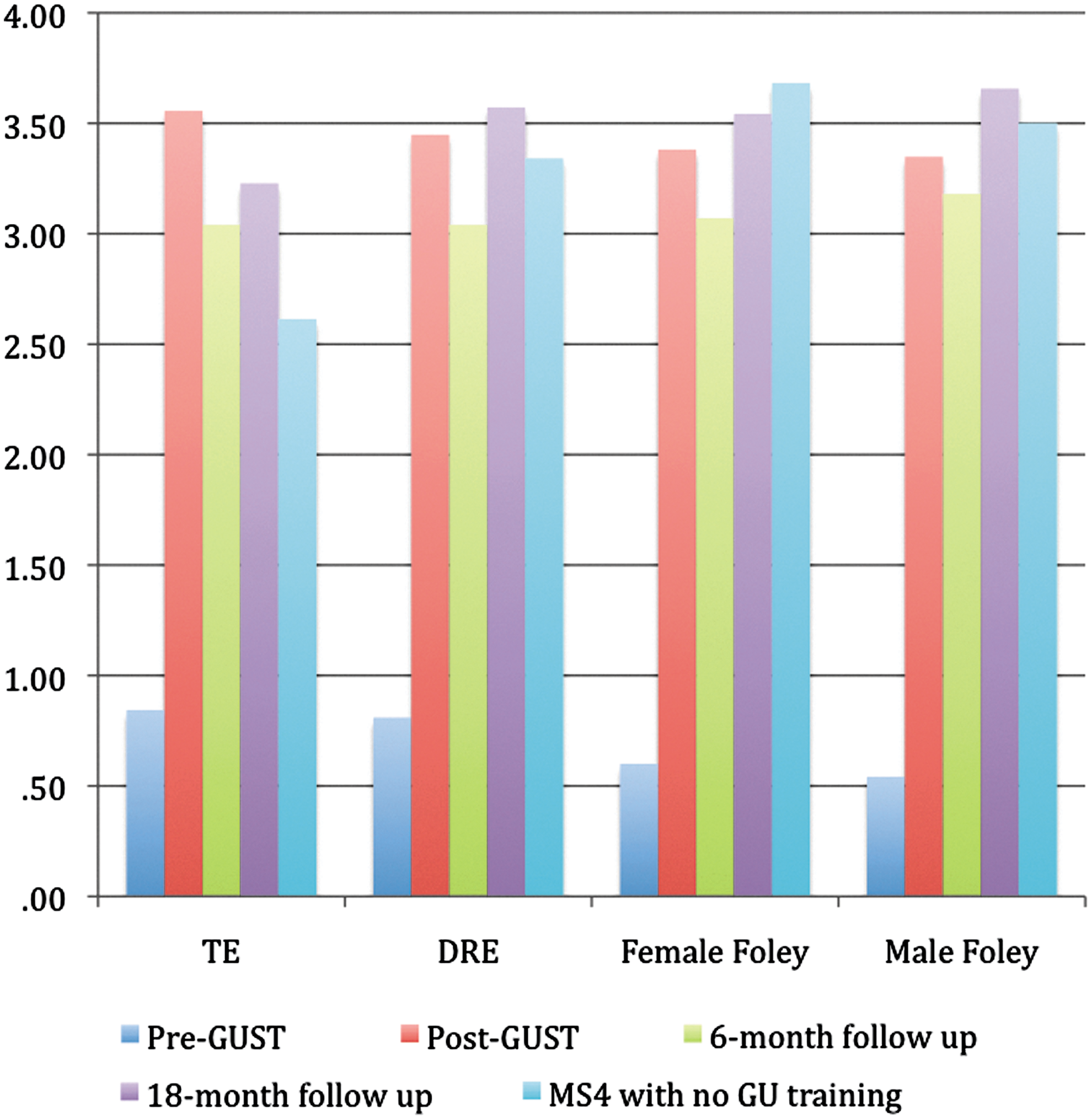
Mean Likert score of medical student comfort level with four GU skills at four time-points. GUST=genitourinary skills training; MS4 – fourth year medical student; TE=testicular examination. DRE=digital rectal examination.
Significantly higher than pre-GUST in independent samples t test (P<0.0001).
Significantly lower than post-GUST in independent samples t test (P<0.0001).
Significantly lower than post-GUST in independent samples t test (P=0.003).
Significantly lower than post-GUST in independent samples t test (P=0.038).
Significantly lower than MS3 at 18-month follow-up in independent samples t test (P=0.037).
Significantly higher than at 6-month follow-up in independent samples t test (P=0.020).
Significantly lower than MS3 at 18-month follow-up in independent samples t test (P=0.037).
GUST=genitourinary skills training; MS4=fourth year medical student.
Before GUST, the number of students who reported being comfortable with the GU skills (Likert>2) ranged from 8.3% to 18.5% (Table 2). After GUST, 88.2% to 96.9% of the students reported feeling comfortable performing the four tasks, a significant increase compared with pre-GUST levels (P<0.001). At 6-month follow up, although the students still reported being more comfortable than they were before GUST, the percent who were comfortable with these skill tasks declined significantly from post-GUST levels. At 18-month follow up, while the students' reported comfort levels were still higher than pre-GUST levels, the percent of students comfortable with the four tasks was significantly higher than at 6-month follow up for DRE and MFC and FFC placement. MS3 at 18-month follow-up reported similar to MS4 on all tasks except TE, where a higher percentage of MS3 felt comfortable with TE than MS4 (P=0.068).
Significantly higher than pre-GUST in independent samples t test (P<0.0001).
Significantly lower than post-GUST in independent samples t test (P<0.0001).
Significantly lower than post-GUST in independent samples t test (P=0.011).
Significantly lower than post-GUST in independent samples t test (P=0.008).
Significantly higher than 6-month follow-up in independent samples t test (P=0.015).
Significantly higher than 6-month follow-up in independent samples t test (P=0.017).
Significantly higher than 6-month follow-up in independent samples t test (P=0.030).
Lower than MS4 students at 18-month follow-up (P=0.068).
GUST=genitourinary skills training; MS4=fourth year medical student.
At both 6-month and 18-month follow-up time points, the majority of respondents reported that they did not have enough opportunities to practice each of the skills. Twenty-four (54.5%) of the 44 MS4 respondents also selected lack of opportunities to practice as the dominant contributing factor to their discomfort with TE while 11 (25%) reported that not enough time was spent on learning this skill. With regard to DRE and MFC and FFC placement, the respondents commonly reported that they “did not have enough opportunities for practice.”
At the 18-month time point, when asked to report on the percentage of new patient or admitting physical examinations in which the students performed a TE within the past month, the minority of both MS3 and MS4 students reported having performed TE (22.9% and 20.9%, respectively) and DRE (45.7% and 37.2%, respectively).
The majority of MS4 students reported having been trained in TE and DRE by faculty. Nurses were the primary group from whom this same group of students learned FFC placement (43%), closely followed by residents (36%). This order was reversed for MFC placement with residents serving as the primary educators (46%) followed by nurses (32%). Eleven percent of the MS4 reported that they had not been taught TE or MFC placement by anyone, and 2% expressed this lack of skill training for FFC placement. Sixty-four percent of these students learned TE while on rotation with the department of family medicine followed by 14% who learned the skill during rotations with internal medicine, 7% during surgery clinical experience, and 2% while on emergency medicine.
The majority of the students who learned DRE were taught by instructors from internal medicine (70%) followed by family medicine (21%), obstetrics/gynecology (OB/GYN) (5%), surgery (2%), and emergency medicine (2%). Fifty percent of the students learned FFC placement through surgery, and 40% learned the skill during their Ob/Gyn rotation, while only 2% were taught by the urology department. Surgery was the dominant rotation during which students learned MFC placement (66%) followed by emergency medicine and internal medicine (7% each) and urology (5%).
The 85 students in GUST 2009 gave a mean score of 4.19 to 4.97 to all four sections. Students ranked the TE and DRE training with SPs as the most useful session followed by the faculty discussion on abnormal GU findings, suturing and knot tying, and lastly Foley catheterization. The students also rated the faculty teaching each section as moderately good to very good with average scores of 3.73 to 3.87 on a scale of 1 to 4 (1=poor, 4=very good).
Discussion
We have shown previously that in the short term, an intensive skills training curriculum significantly improved medical student comfort with regard to basic GU skills, including DRE, TE, and MFC and FFC placement. We considered it equally important, however, to evaluate the intermediate and long-term student comfort and clinical application of these GU skills.
From this study, we have first observed that after learning these skills, students show an immediate and significant increase in their comfort with these skills that lasted throughout their medical school career. Their immediate increase in comfort is likely multifactorial. In the case of the TE and DRE, the students commented on a sense of relief to be able to practice tasks that involve contact with sensitive and potentially painful areas of the physical examination under the guidance of an expert clinician. By having the instruction of both the expert urology faculty and the feedback directly from the SPs, the students learned the key points of these clinical patient assessments and how to minimize patient discomfort. With proper demonstration and a perceived “safety-net,” the students gained more confidence in their own skills. The integration of didactic instruction with the opportunity for hands-on practice, provided students a more comprehensive understanding of these clinical tasks which they would soon be expected to perform routinely when evaluating patients.
In the case of the Foley catheter placement, the students had the unique opportunity to review lower GU anatomy by way of virtual reality cystourethroscopy (during the first iteration of the course), a didactic lecture, and a teaching model before learning, through hands-on practice, the proper technique for Foley catheter placement in an inanimate model. Student comfort with these tasks waned at the middle of their third year. This may be related to a decrease in opportunities to practice their skills on the clinical wards. As the students progressed through their rotations, however, they reported an increase in comfort that ultimately reached, and in some skills surpassed, the MS4 students who had not received a formal GU skills training curriculum.
Second, it should be noted that graduating students without formal examination skills training reached a statistically similar level of comfort with DRE and MFC and FFC placement by the end of medical school. These data can be interpreted in several ways. The MS3 students post-GUST reached the same level of comfort as those who did not take the course, suggesting that the course imparted minimal benefit, or that after an initial immediate benefit after the course, the students' comfort reached a plateau comparable to the levels of those who did not take GUST.
Interestingly, the MS4 were less comfortable with TE compared with the GUST-trained MS3s. This reported observation may be because several students (11%) were never formally taught to do a TE on the wards. Within the current medical education paradigm, authors have described considerable variation in the clinical experiences obtained by students in terms of both the range of cases and numbers of patients seen. 10 Without a clear teaching structure and educational objectives, students learned all of these skills from several different services in a noncohesive way, and often from personnel other than faculty. This type of training could potentially result in serious gaps in these students' medical education and skills learning.
These observations highlight the importance of providing a standardized curriculum for all students to learn and practice basic medical skills. Several studies have demonstrated the usefulness of SPs for teaching and evaluating GU skills to medical students. 3,11 In a survey of medical school physical examination course directors, Dull and Haines 12 observed that the genitalia examinations were primarily taught by demonstrating (54.2%) and practicing (65%) on SPs. Respondents to their surveys maintained that the best method for teaching the genital examination was by practicing on SP. 12 Anderson and colleagues 13 similarly noted that 60% of United States and Canadian medical schools use SPs for teaching and evaluating female pelvic examination but only 39% use SPs for the male genital examination. 13
A third important observation from this study was a concerning low percentage of students performing DRE and TE for admitted patients, despite the stated importance of these examinations as part of the routine physical examination. Many medical students can be relatively passive in the educational process and may not actively seek out opportunities to practice, although they generally agree that practice is essential for the mastery of skills. 10 We are presently identifying clinical rotations where the students may receive additional clinical experience in performing these clinical skills and making the performance of these examinations and procedures a requirement of the rotation, such as during the emergency medicine, operating room, or obstetrics experience.
The long-term goal of the course was to create a learning experience that would foster retention of the information and skills taught for application in clinical practice. The course met these objectives. Follow-up of these students demonstrated a potential need for continued opportunities to practice these skills either in the educational or clinical setting to maintain their comfort. In addition, further follow-up of these students' competence with these skills and the relationship of competence to comfort in performing them must be ascertained.
Conclusion
A GUST curriculum significantly improved medical student comfort with examination skills and Foley catheter placement in the short term, and their comfort remained throughout their medical school career. Graduating students without formal GU examination skills training reached a statistically similar level of comfort with DRE and MFC and FFC placement by the end of medical school, but not in TE, likely because of a lack of formal teaching. A concerning low percentage of admitted patients received a DRE or TE from a medical student, with or without having received a formal curriculum, despite the stated importance of these examinations as part of the routine physical examination.
Footnotes
Disclosure Statement
No competing financial interests exist.