
Abstract
Purpose:
The aim of our study is to assess the impact of skill in laparoscopic surgery on the learning of robot-assisted surgery by urologic surgeons using the Mimic dV-trainer (MdVT).
Materials and Methods:
Twenty-three urologic surgeons using the MdVT were assessed. Ten of them were laparoscopic surgeons certified by the Japanese Society of Endourology. Each of the subjects completed four trials of a program consisting of four EndoWrist modules and two needle-driving modules. The performances of all subjects were recorded using a built-in scoring algorithm.
Results:
In only one of the needle-driving tasks, Suture Sponge (that all subjects felt was the most difficult task), the scores of the certified laparoscopic surgeons became significantly better than those of the other subjects at the 2nd and the 3rd trials (p=0.0236 and p=0.0043 at the 2nd and 3rd trials, respectively). At the 4th trial there was no significant difference between the two groups with regard to the overall scores of any tasks.
Conclusions:
Our data indicate that familiarity with laparoscopic surgery is not associated with any advantage in learning the most fundamental techniques of robot-assisted surgery.
Introduction
Robot assistance can help surgeons overcome the technical difficulty of laparoscopic surgery, and previous studies have reported the benefits of robot-assisted surgery for urological diseases. 5 –9 Although laparoscopic surgeries for urology have been widely used in Japan, robot-assisted surgery is just beginning to be used there because the da Vinci Surgical System did not receive approval under Japan's Pharmaceutical Affairs Law until 2010. Many urologic surgeons will start using robot-assisted surgery regardless of the maturity of their laparoscopic technique, and the adaptability of individual surgeons to robot assistance is still unclear. Mimic's dV-Trainer (MdVT; Mimic Technologies, Inc.) is a virtual-reality simulator for the da Vinci Surgical System. Its face, content and construct validity have been confirmed, 10,11 and it has been shown to be useful for helping urologic students gain skill in robot-assisted surgery. 9,12
Japanese Society of Endourology and Japanese Urological Association (JUA) have conducted the certification system for laparoscopic surgeons, called “Endoscopic Surgical Skill Qualification System in Urologic Laparoscopic Surgery (ESSQSJJ)”. 13,14 ESSQSJJ is a well-validated system to ensure surgeons can perform urologic laparoscopic surgery as a chief surgeon with a low prevalence of perioperative complications and reasonable outcomes. 14 In this system, surgeons are required to experience 20 or more cases of laparoscopic surgery and to pass a video examination. Because certified laparoscopic surgeons thus have a fundamental laparoscopic surgery technique, it is adequate to compare between two groups: certified and uncertified surgeons for measurement if an obvious benefit exists for experienced laparoscopic surgeons.
Here, we report our evaluation of the relationship between urologic surgeons' experience in laparoscopic surgery and the degree to which using the MdVT helps them develop the basic skills needed in robot-assisted laparoscopic urologic surgery.
Materials and Methods
Subjects
This study used 23 urologic surgeons recruited from four hospitals in Hiroshima Prefecture, and the numbers in the experienced and inexperienced groups were chosen in accordance with previous studies of virtual-reality surgical simulation. 9 –12 To compare between groups of urologists with and without fundamental laparoscopic skill in this study, subjects were classified into two groups based on the existence of the certification by ESSQSJJ. 13,14 Ten of them (group A) were certified by ESSQSJJ as surgeons with fundamental technique of urologic laparoscopic surgery, and 13 of the surgeons (group B) were not. The median age, number of years of urologic practice, and experience of a laparoscopic surgeon were significantly greater in group A (Table 1). None of the subjects in this study had any previous experience with the MdVT, and there was no subject who had experienced the procedure of da Vinci system including training program.
Simulator and task
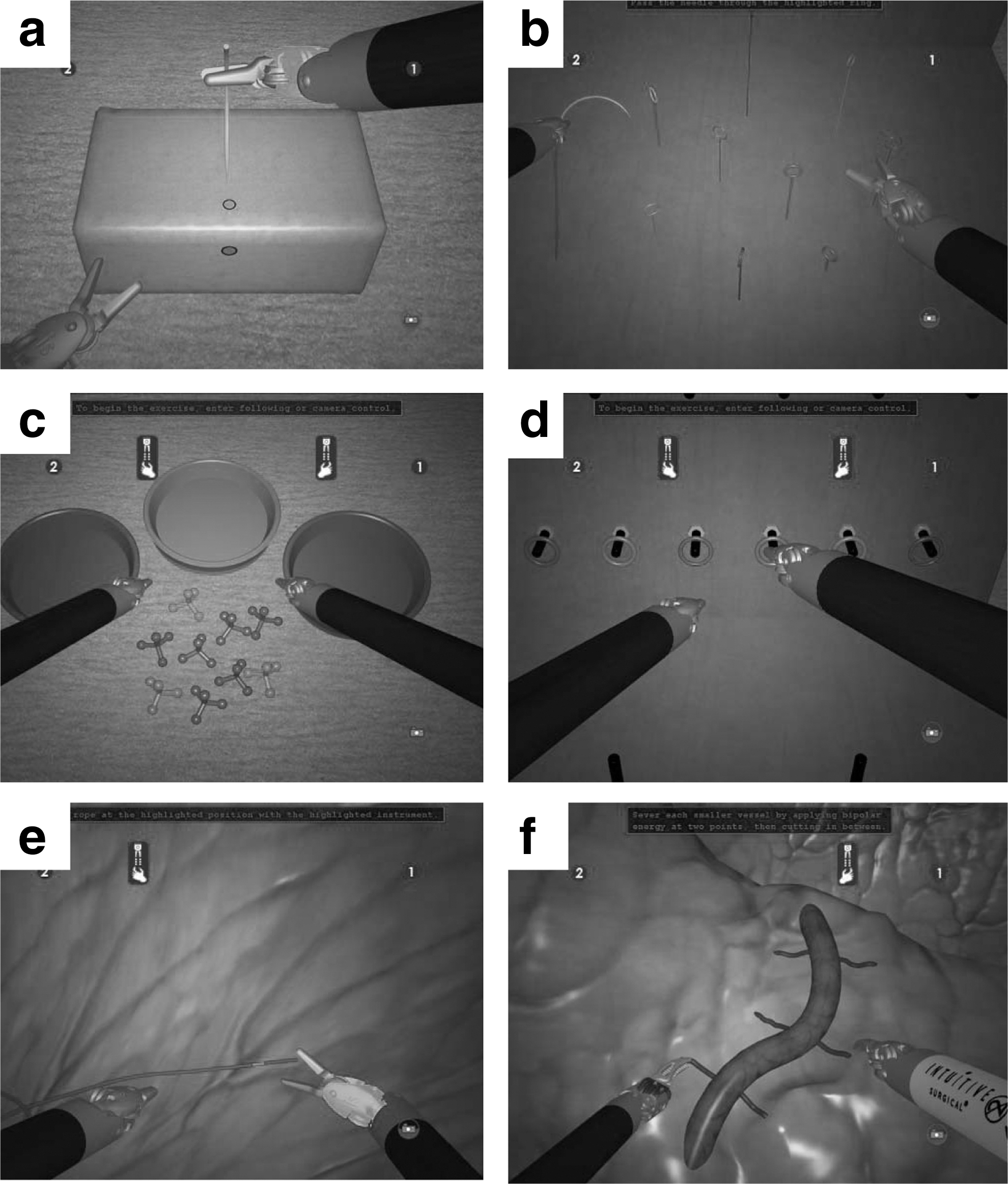
Each of the trials in this study consisted of six MdVT tasks, four focused on EndoWrist manipulation (Pick and Place, Peg Board, Rope Walk, and Energy Dissection) and two focused on needle-driving (Suture Sponge and Thread the Rings) (Fig. 1). In the first trial, before starting a task the subjects were given 2–3 minutes to become familiar with the platform and the task. After finishing the 1st trial, each subject completed a questionnaire about the difficulty of the tasks and repeated the trial three more times.
The program for the present study consisted of two needle-driving modules:
Performance was assessed using the built-in scoring algorithm considering the following metrics: Critical Errors, Economy of Motion, Number of Drops, Excessive Instrument Force, Instrument Collisions, Master Workspace Range, and Time to Completion.
Statistical analysis
All statistical analyses were conducted using the Statview 5.0 software package (SAS Institute Inc.). Scores for each task were compared between groups A and B, and 1st trial and others. These were assessed by Mann–Whitney U test and Wilcoxon test, respectively. A p value less than 0.05 was considered statistically significant.
Results
The overall scores for each task in each of the trials are listed in Table 2. For five of the six tasks the overall scores in the first trial did not differ significantly between groups A and B. For Peg Board, however, the overall score of group A was significantly better than that of group B.
p<0.05 (1st trial vs. 2nd, 3rd and 4th trials)
In the 2nd to 4th trials there was no significant difference between groups A and B in the overall scores for any of the EndoWrist-manipulation tasks or for Thread the Rings. The overall score for Suture Sponge, however, was significantly better for group A in both the 2nd and 3rd trials. We therefore assessed the Suture Sponge data for the two groups in more detail. As shown in Table 3, in the 2nd and 3rd trials the Critical Errors and Economy of Motion Value for group A were significantly better than those for group B, and in the 3rd trial the Master Workspace Range Value was significantly better for group A. In the 4th trial none of the scores differed significantly between the two groups.
p<0.05 (1st trial vs. 2nd, 3rd and 4th trials)
Discussion
The present study evaluated the learning of robot-assisted surgery by urologic surgeons. Both certified experts in laparoscopic surgery and surgeons with little experience in laparoscopic surgery can develop similar levels of skill in robot-assisted surgery by using the MdVT. To the best of our knowledge, the present study is the first to investigate the impact of experience in laparoscopic surgery on the MdVT-assisted learning of robot-assisted surgery skills by urologic surgeons.
Learning the robot-assisted technique with efficacy and safety before using it on patients is very important. Delp et al 15 reported the first simulation system for studying the technique of orthopedic surgery in 1989, and the first virtual-reality simulator for use in robot-assisted surgery was reported in 1993. 16 In recent years the evolution of virtual-reality simulation or training systems for laparoscopic and robot-assisted surgery techniques has progressed remarkably, and many simulators have been widely used for training surgical residents or medical students and assessing their skills. Previous studies have demonstrated that MdVT scores were closely related to the maturity of robot-assisted surgery technique. Although some other simulators have been reported, 17 –20 the MdVT is thought to be one of the best investigated. Thus, in this study we evaluated the effectiveness of using the MdVT to learn the techniques used in robot-assisted surgery.
There are six kinds of basic tasks in the MdVT program modules. Four of them intended to develop EndoWrist manipulation and two intended to develop needle-driving skill (Fig. 1). Each is offered at various levels of difficulty. Because we focused the initial period of the learning curve and all of the subjects were novices, all subjects were evaluated at the easiest level of these six tasks. To evaluate the learning curve for more advanced robot-assisted skills, other studies using programs consisting of tasks with different levels are required.
With regard to overall score, in the 4th trial there was no significant difference between the two groups (Table 2). Previous studies have demonstrated that the use of robotic assistance significantly improved the learning curve for laparoscopic surgery, 21 –23 especially in the learning of suturing skills. 19 Our results are consistent with those reports and also suggest that the maturity of a subject's laparoscopic surgery technique may have no relationship to the development of fundamental robot-assisted surgery skills after a few training sessions. On the other hand, for Suture Sponge the overall score of group A was significantly higher than that of group B in the 2nd and the 3rd trials (Table 2). The scores of group A were better than those in group B with regard to Critical Errors, Economy of Motion, and Master Workspace Range (Table 3). These findings indicate that, in the initial phase of learning the skills of robotic surgery, more experienced laparoscopic surgeons are more effective and safer than surgeons less experienced in laparoscopy. The surgeons in the certified group had larger volumes and experience of laparoscopic surgery. Laparoscopic suturing technique is well established as one of the most discriminating skills. Thus, the present Suture Sponge data were an expected finding for us. Even in this task, however, practice on the simulator quickly produced score improvements in all participants, and at the 4th trials the overall scores of the certified laparoscopic surgeon did not differ from those of others (Table S1).
We herein focused on just gain of “technique.” In actual surgery there are a lot of other important factors such as mental factors, spatial intelligence, anatomical understanding, and cooperation with assistant staff. Previous studies reported that psychological stress impaired the learning curve of surgical performance, 24,25 and a randomized control study based on the virtual-reality curriculum for laparoscopic cholecystectomy demonstrated that mental practice enhanced the quality of surgical performance 26 and reduced subjective, cardiovascular, and neuroendocrine response to stress. 27 Another study reported the effect of spatial ability on learning of complex surgical techniques. 28 These studies were designed for laparoscopic surgery or open surgery, and investigation of the effects of such factors on training in robot-assisted surgery may lead to some improvement of the learning curve.
Conclusions
In the present study we demonstrated that the fundamental technique of robot-assisted surgery can be gained through a few MdVT training sessions regardless of one's familiarity with laparoscopic surgery. Robot-assisted surgery will soon be more widely used. We focused on the initial period of learning, so future studies are expected to assess the learning curve for gain of higher level techniques of robot-assisted surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.