
Abstract
Objective:
To analyze our experience in management of urolithiasis in renal donors.
Materials and Methods:
The stones were treated either pretransplant or posttransplant. The Amsterdam forum criteria for acceptance of living donors were used for donor selection. The donors underwent the following procedures: pretransplant extracorporeal shock wave lithotripsy (ESWL) (n=5), pretransplant retrograde intrarenal surgery (RIRS) (n=1), ex-vivo ureteroscopy (ex-vivo URS) (n=1), and ex-vivo pyelolithotomy (ex-vivo Pyl) (n=2); intraoperative Double-J stent; and observation (n=3). Data were analyzed for technical feasibility, intraoperative and postoperative complications, and stone clearance.
Results:
The male and female ratio was 4:8 and average age was 52.3 years (38–71). In the pretransplant ESWL group, average of 740 shocks (600–1500) was given; the power was not ramped up beyond 12 kV. Ex-vivo URS was performed on bench with 6F pediatric cystoscope, while in the ex-vivo Pyl, a 12F nephroscope was introduced via a pyelotomy and stones were retrieved intact with a dormia basket. A postoperative ultrasound at one month revealed complete clearance of stones in all except one donor. At a mean follow-up of 36 months (10–58), there was no stone recurrence in donor or recipient.
Conclusions:
This report shows the feasibility and safety of ex-vivo URS and ex-vivo Pyl in living donors, in select cases with subcentimeter calculi, an option of conservative management with Double-J stent is safe. ESWL/RIRS can be performed safely in the pretransplant setting. Proper donor selection and follow-up are crucial to success. We propose a treatment selection algorithm for management of these donors.
Introduction
Due to recent trend of performing computed tomographic angiography as a part of work-up, increasing number of donors with nonobstructing unilateral asymptomatic stones are diagnosed during donor work-up. These potential donors are likely to be rejected by centers due to concerns regarding management of stones in the graft and the risk of recurrence, in spite satisfying other Amsterdam criteria. 1,3
In this article, we evaluated the safety and efficacy of extracorporeal shock wave lithotripsy (ESWL), retrograde intrarenal surgery (RIRS), ex-vivo ureteroscopy (ex-vivo URS), and ex-vivo pyelolithotomy (ex-vivo Pyl), as a means of rendering a donor and/or the harvested graft stone free in living-related donor renal transplantation.
Materials and Methods
After institutional review board approval, a retrospective chart review of all cases who had urolithiasis during live renal donor work-up was done. Data analyzed included technical feasibility and details of all the modalities employed, intraoperative and postoperative complications, and the recipient outcome at follow-up. All patients with <4 mm stones were counseled regarding follow-up. They were explained the possibility of residual stones and the steps to be taken in the event of olignuria or anuria.
Criteria for selection of treatment modality
As a dictum the “better kidney was left with the donor.” The decision to treat the stone pretransplant or posttransplant was taken after assessing the CT findings. It was imperative that the patient did not have any metabolic abnormality prior to acceptance as donor. Hard stones with higher Hounsfield units (>1200) were preferably tackled with ex-vivo (URS or Pyl) endoscopic intervention or preoperative RIRS. The choice between the two was decided by the pelvicalyceal anatomy. All stones that were soft (<1200) were tackled with pretransplant ESWL. Stones <4 mm were treated with Double-J stenting and close observation (Fig. 1). The wait period between pretransplant RIRS/ESWL and transplantation was 3 weeks. The stone clearance was confirmed on ultrasound and kidney, ureter, and bladder (KUB) skiagram. The anatomic considerations for deciding the modality were the infundibular width, infundibular length, and the pelvicalyceal angle.

Proposed management algorithm for urolithiasis in donors.
Techniques used for stone clearance
Ex-vivo ureteroscopy
Ex-vivo URS was done with a pediatric cystoscope (6F). The pediatric cystoscope has the advantage of better stability and maneuverability due to its short shaft length. The longer length of the semirigid ureteroscope prevents free movement of the ureteroscope. The procedure was done after the graft was perfused on the recipient back bench. Perfusion was considered to be adequate and the onset of cold ischemia was confirmed when the outflow of saline from the vein was clear. Throughout the procedure, the kidney was placed immersed in cold saline. Fluoroscopy was used in none of the cases. The stones were removed intact. The average procedure time was 20 minutes. The graft was kept immersed in ice slush throughout the procedure. In contrast to ureteroscopy in an orthotopically placed kidney, the graft kidney does not exhibit narrowing as in a normal ureter; thus, the kidney can be manipulated to facilitate the angle of entry into the desired calix (Fig. 2). In two of our cases, we attempted ex-vivo URS; however, the ureter was narrow and did not allow dilation. In these cases we performed an ex-vivo Pyl.
Ex-vivo ureteroscopy. A 6F pediatric cystoscope is used for graft retrieval. Complete clearance of stone is ensured by removal with dormia basket.
The irrigation during ex-vivo manipulation was kept to minimum. 1 There have been concerns with retrograde pyelovenous and pyelolymphatic backflow. After the completion of procedure, a Double-J stent was placed in all.
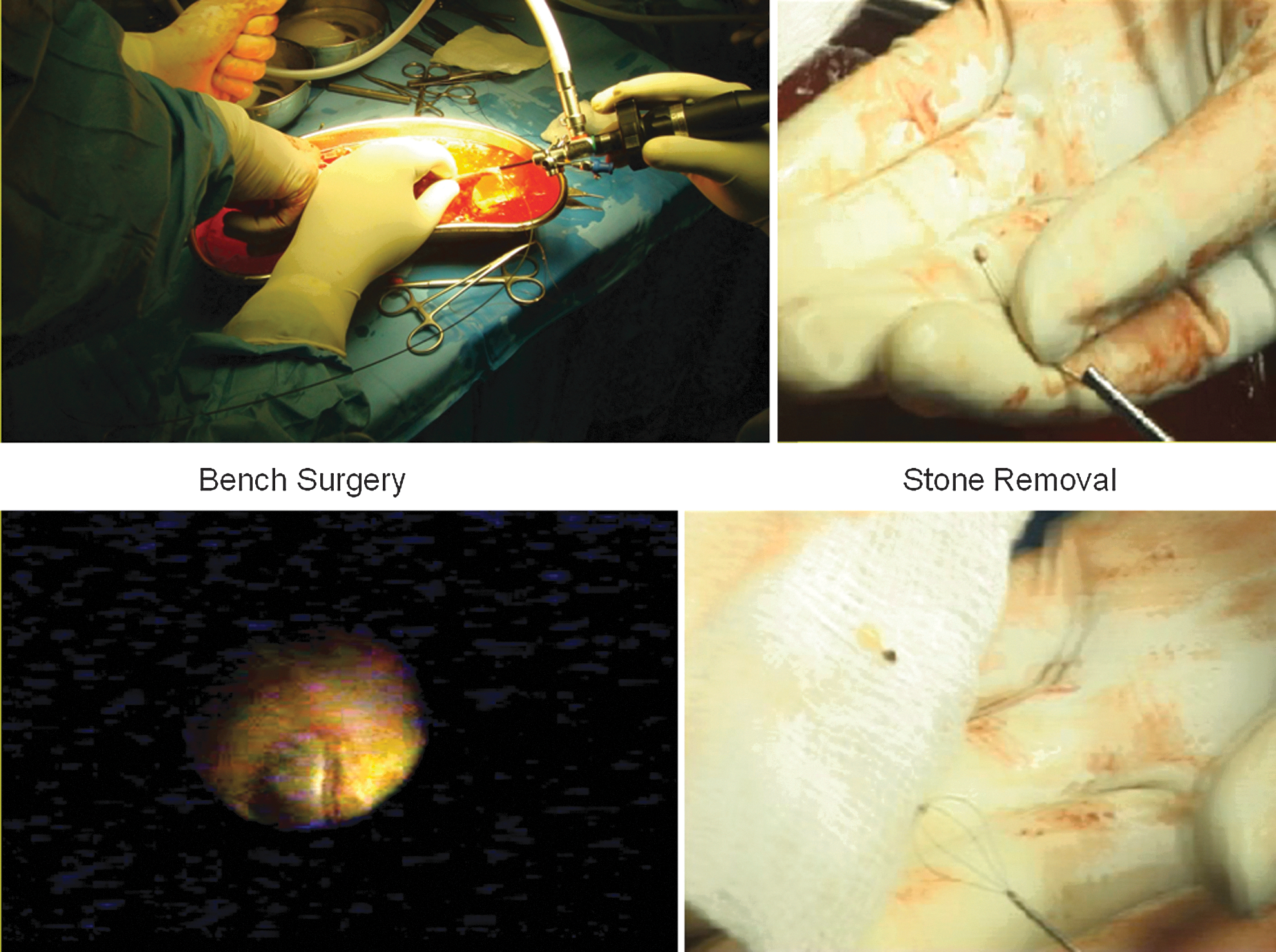
Ex-vivo pyelolithotomy
Cold saline perfusion was done on the bench. The procedure was done under cold ischemia. An attempt was made to negotiate a pediatric cystoscope, but this was not possible. Hence, a pyelotomy was done between stay sutures. The pyelotomy offers a safe conduit for negotiating the instrument safely without injuring the ureter in select cases. The stay sutures help in stabilizing the pelvis. The assistant held the graft, thus stabilizing and preventing its rotation. We preferred to use a dormia basket for stone retrieval. The pyelotomy was closed with absorbable sutures. This helped in intact removal of stone. None of the stones were fragmented. A 12F nephroscope was used to retrieve the stone intact with dormia basket. A stent was placed at the completion of the procedure (Figs. 3 and 4).
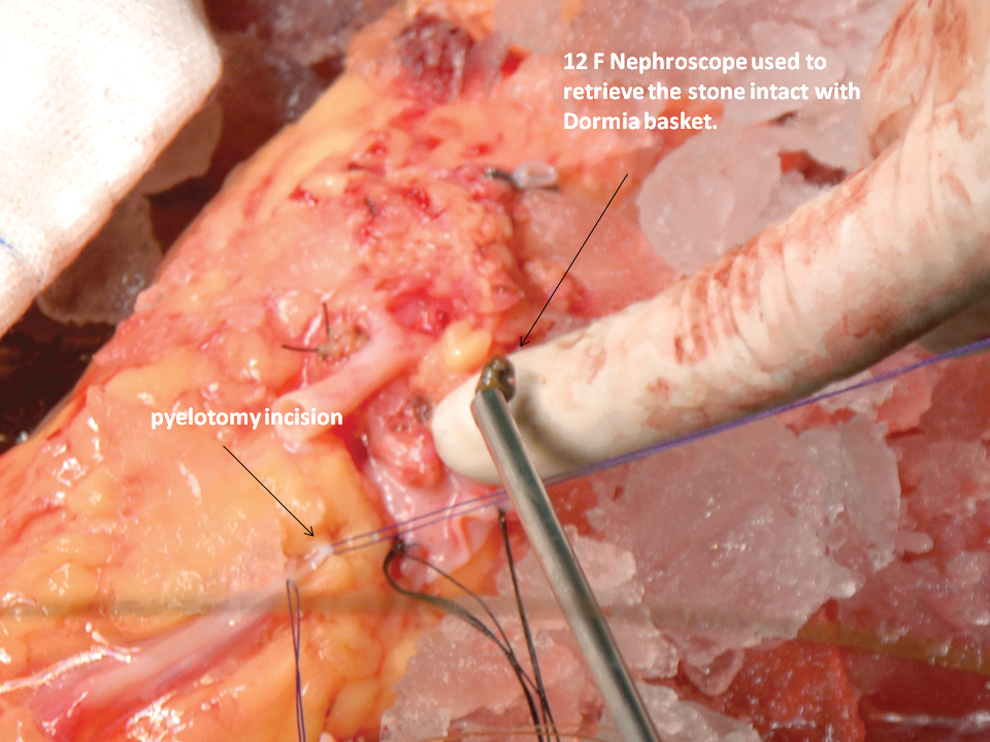
Ex-vivo pyelolithotomy. An attempt was made to pass a ureteroscope on the bench, as the ureter was tight. A pyelotomy was made and the stone was removed with a 12F nephroscope.

Ex-vivo pyelolithotomy. Pyelotomy closure.
Pretransplant ESWL or RIRS
The factors that influence the decision for pretransplant ESWL and RIRS are the size and density (Hounsfield units) of the stone, pelvicalyceal system anatomy, and the side to be selected for donation. The energy, frequency, and the power of lithotripsy were kept at minimum for this group of patients. The compliance of the patient is a crucial factor in deciding the treatment modality. Imaging should show complete clearance of stone prior to transplantation (Fig. 5). The procedural details are given in Tables 1 and 2.

A computed tomography scan showed evidence of 8-mm right middle calix calculus. Eight hundred fifty shocks were given and a left donor nephrectomy stone was completely cleared.
RK=right kidney; MC=middle calyx; ESWL=extracorporeal shock wave lithotripsy; F+U=fluoroscopy and ultrasound; LK=left kidney; LC=lower calyx; USG=ultrasound; RIRS=retrograde intrarenal surgery.
Ex-vivo URS=ex-vivo ureteroscopy; ex-vivo Pyl=ex-vivo pyelolithotomy; HU=Hounsfield units; MC=middle calyx; UC=upper calyx.
Results
Twelve renal donors were included in the analysis. The male and female ratio was 4:8 and average age was 52.3 years (38–71). In the pretransplant ESWL group, an average of 740 shocks (600–1500) was given. The power was not ramped up beyond 12 kV and the frequency was kept at 60 per minute. Ex-vivo URS was performed on bench with 6F pediatric cystoscope, while in the ex-vivo Pyl, a 12F nephroscope was introduced via a pyelotomy and stones were retrieved intact with a dormia basket. A postoperative ultrasound at one month revealed complete clearance of stones in all except one donor. In this donor, a Double-J stent was placed and he was planned for observation. A follow-up ultrasound showed a persistent stone. At a mean follow-up of 36 months (10–58), there was no stone recurrence in donor or recipient (Table 2). The recipient outcome at follow-up is as shown in Figure 6. The bench procedures added 20 minutes of time after onset of cold ischemia. As the ex-vivo procedures were done after the onset of cold ischemia, they did not affect the overall outcome.
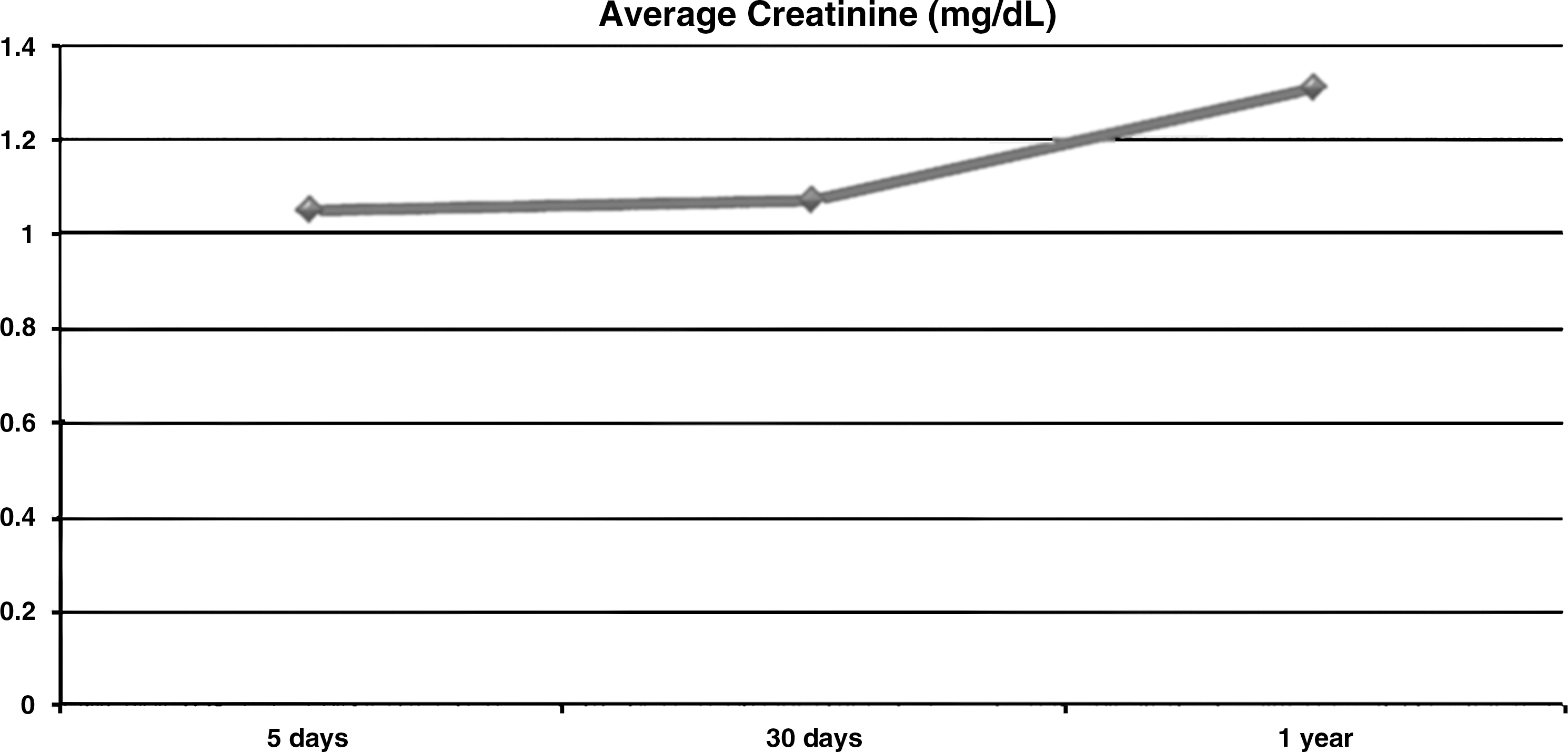
The trend in serum creatinine in recipients.
Discussion
In living donors, the surgeon is bound by the principle that “first do no harm” to the donor. 2 With the advent of CT angiography as a modality in the work-up of living donors, the incidence of detection of small asymptomatic calculi has exponentially increased. It is also a known fact that stone formers have a tendency to form recurrent stones. In one study, 50 patients were followed up for longer than 5 years post-unilateral nephrectomy for nephrolithiasis. About 30% developed recurrent stones. Patients with metabolic stone disease had a higher recurrence rate compared with those with infection as the cause of stone formation (37% v 13%, respectively). 4,5 This data assumes importance in a healthy donor with a history of stone.
In our series, the decision to perform either an ex-vivo endourologic manipulation or treat the stone prior to the transplant was taken depending on the angiography findings (single or double vessels), location size, and density of the stone.
Management of stones after transplantation is more complex because the presentation is unusual. The diagnosis is often delayed; on most of the occasions, the patients do not present with colic due to severing of perinephric nerves during transplantation. The most common presentation is rising serum creatinine with hydronephrosis. The management of urolithiasis after transplantation depends on the site, size, and the presentation of the stone. Bhadauria et al. have described extracorporeal lithotripsy in a stone-bearing kidney after transplantation. 6 The management of anuria following a ureteral obstruction due to stone can be challenging in view of the lie of the transplanted ureter. Typically, the initial step would be percutaneous decompression of the pelvicalyceal system. Once the creatinine reaches nadir, the stone can be approached either with an antegrade or retrograde ureteroscopy depending on the size and location of the stone.
The utility of ESWL has been demonstrated in allograft with stones after transplantation. In an article by Wheatley and associates, they describe their experience of extracorporeal lithotripsy in allografts. Both of their patients did well after the procedure. 7 Contrary to belief, we did not notice any increased edema or friable tissue during laproscopic donor. Nephrectomy was done in donors who had undergone a pretransplant ESWL to clear the stone. We based our decision to use ESWL as the modality to treat stones depending on the Hounsfield units on CT scan. In one of our earlier studies, we noted that the results of ESWL were excellent if the Hounsfield unit was <1200. 8
We have electively stented all recipients with stones <4 mm. All, but one, recipients showed complete clearance of stones. Martin et al. noted that asymptomatic small stones can be followed up conservatively without any consequence. In this article, we evaluated the rate of spontaneous passage, development of symptoms, and change in the size of asymptomatic renal calculi in donor kidneys transplanted. 9 In a series by Devasia et al., all, except one, stones <4 mm passed spontaneously. All the five patients in this series had a good graft function at 5 years. 10
Percutaneous nephrolithotomy (PCNL) in allograft is well described. Large stones in a renal allograft need clearance with PCNL. PCNL in an iliac fossa transplant needs to be done in a supine position because of the position and lie of the kidney. The access point should be lateral as a more medial access would harbinger the risk of an intraperitoneal transgress. It would also be prudent to gain an upper pole access in such situations as this would make manipulations into the upper ureter and the renal pelvis easier if required; in addition, an upper pole access would decrease the chance of injury to the bladder, ureter, and major vascular structures.
Francesca et al. report a case of a staghorn calculus in a 45-year-old lady who was a recipient of a renal allograft. 11 There are concerns regarding the density of scar tissue and the difficulties in dilating the tract. To overcome the morbidity, larger instruments, and working sheaths in these patients, Del Pizzo et al. have used a modification for an O'Brien suprapubic peel off sheath for PCNL in these patients; this helped in decreasing the size of the nephroscopes. 12 The limitations of our study include retrospective design, lack of graft function/complication data, and lack of stone recurrence data.
To summarize, living-related donors suit the dictum best “primum non nocere.” Hence, these donors should be selected prudently. The “benchmark” should be to leave the best kidney with the donor. Endourologic intervention forms the cornerstone for rendering the donor stone free to enable successful engrafting. The decision to perform pretransplant or “on bench” intervention is decided by the side of the stone, the size, location, and number. ESWL/RIRS can be performed safely in the pretransplant setting. Ex-vivo URS and ex-vivo Pyl were equally safe and technically feasible, to render a stone-bearing kidney stone free without compromising ureteral integrity or renal allograft function. The risk-reduction strategies to be employed to prevent ureteral trauma during ex-vivo endourologic manipulations are as follows. (1) Minimal handling of the ureter. If ureter is tight, an ex-vivo Pyl is a viable option. (2) To prevent potential for pyelovenous and pyelolymphatic backflow, the influx of the irrigant fluid should be kept to minimum. (3) A short ureteroscope or a pediatric cystoscope is preferred because the shorter length of these instruments gives better stability and ease of removal. (4) Placement of a Double-J stent is useful in all cases after manipulations.
Long-term vigilant follow-up for both the donor and the recipient is essential.
Footnotes
Disclosure Statement
No competing financial interests exist.