
Abstract
The retraction of the liver is essential to obtain a better laparoscopic view in right nephrectomy. A simple technique for liver retraction during laparoscopic right renal surgery using surgical cotton is presented. The advantage of the presented method is that this technique is simple, does not require special equipments, and eliminates the need for any additional ports.
Introduction
Technique
Under general anesthesia, the patient is placed in a semilateral position. The camera port is inserted via an infraumbilical incision, and two additional trocars are placed in a triangular shape. This retraction method requires a surgical cotton tape 8 cm long and 1 cm wide. Two silk sutures in 15 cm lengths are tied to the two different ends of the cotton tape (Fig. 1). The tape is then inserted into the peritoneal cavity through a 10-mm trocar, and placed below the gallbladder and liver bed. Under laparoscopic visual control of the abdominal wall, a Carter Thompson needle is inserted in the midline epigastrium directly below the xiphoid (Fig. 2). Next, one end of a silk suture is grasped by the Carter Thompson needle and the suture is pulled back up through the abdominal wall. The end of the suture is then fixed snugly on the abdominal wall with a clamp (Fig. 3). Subsequently, the other end of the suture is also exteriorized. A gentle palpation of the posterior chest wall before the needle insertion will help decide exactly where the needle should be entered. With moderate traction applied to the two ends of the suture, the right lobe of liver is pulled up to the anterior abdominal wall (Fig. 4). At the end of the surgery, the cotton tape can be easily retrieved by declamping the hemostats.
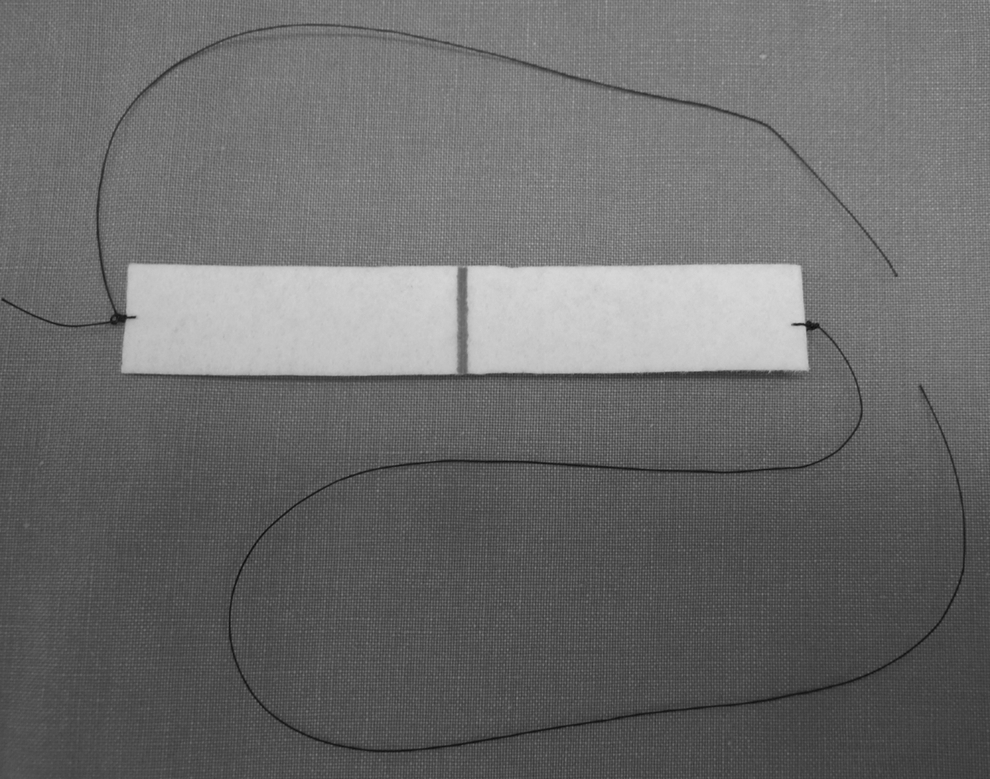
8×1 cm cotton tape tied with silk sutures.
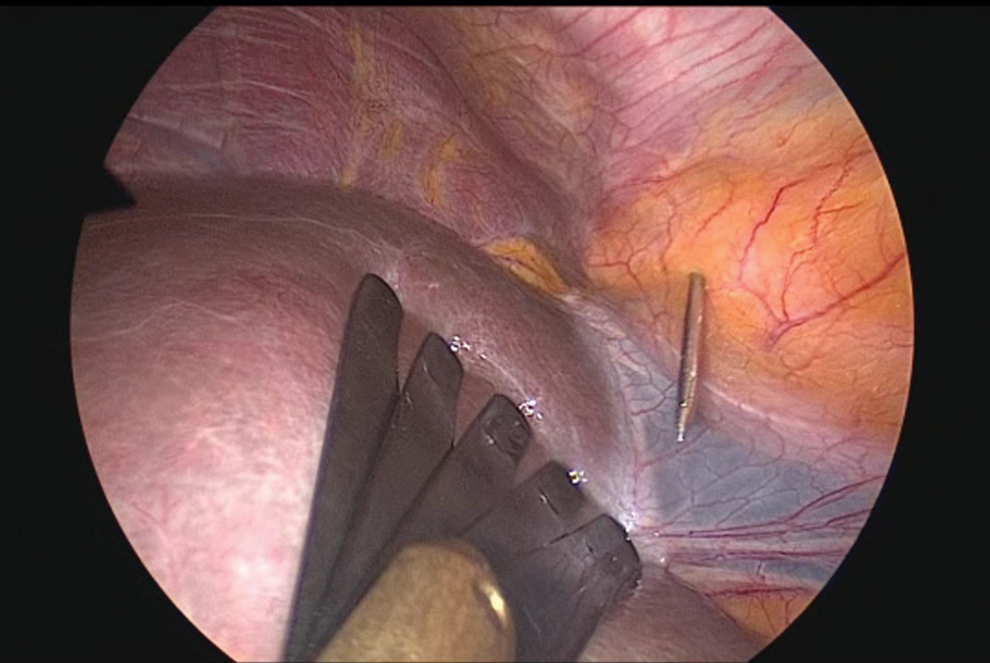
A Carter Thompson needle is inserted in the midline epigastrium directly below the xiphoid.
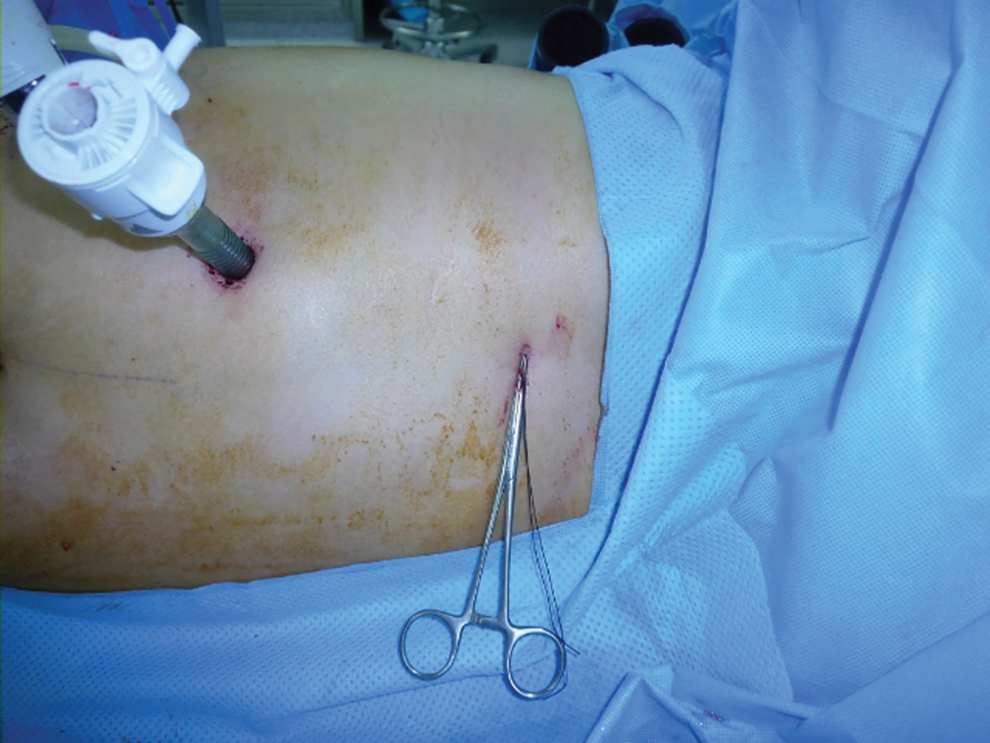
External view of the surgical field during laparoscopic right renal surgery. A silk suture is fixed with clamp.
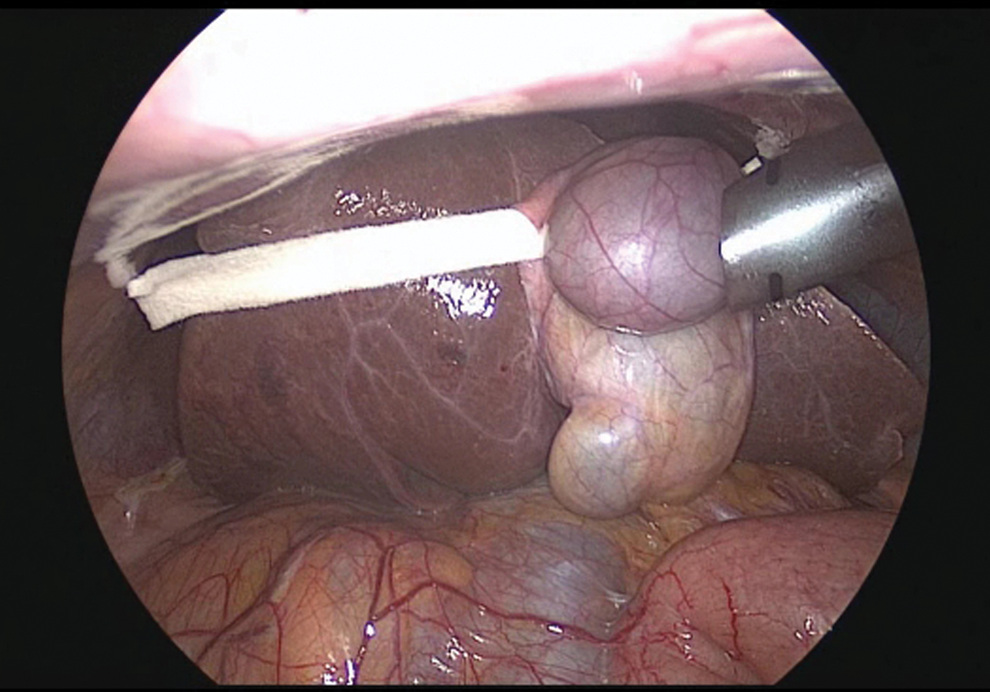
Laparoscopic view showing status after liver retraction using a cotton tape.
To judge the location of puncture site and cotton tape is critical point of this technique. First, mechanical retractor is used to retract the liver to confirm the most appropriate status of retracted liver. Second, puncture site of Carter Thompson needle is confirmed after appropriate location of cotton tape has been determined. This can be performed by placing the cotton tape at a location where liver and gallbladder is well elevated and does not slip (Supplementary Video S1 is available online at
Equipment
A 10-mm, 30-degree video laparoscope (Olympus Surgical, Orangeburg, NY), surgical cotton tape tied with silk suture, Carter Thompson needle, hemostat clamp, atraumatic forceps, laparoscopic fan retractor, and an ultrasonic cutting and coagulating system (Harmonic Scalpel; Ethicon EndoSurgery, Cincinnati, OH).
Role in Urologic Practice
To perform the right-sided renal surgeries effectively, it is important to lift up the liver to obtain a favorable field of view of the kidney and the vena cava. To retract the right lobe of the liver, some surgeons use a laparoscopic retractor or 5-mm-locking graspers. These methods require an additional port and an extra assisting hand. 4 –6
Before using our current retraction technique, we routinely employed an additional 5-mm subxiphoid port and a 5-mm self-locking forceps was used to lift the liver with the forceps tip secured to the posterior diaphragm. Although these mechanical retractors provide an effective and efficient liver retraction, they have several limitations as well. First, their insertion requires a 5-mm incision, inducing more pain and leaving a visible scar at the subxiphoid area. 7 Second, to fix the retractor, the forceps tip that secures the diaphragm sometimes injures the tissues and causes bleeding. Further, the locked grasper, once positioned optimally, may not remain in place; therefore, frequent manipulation and repositioning of this forceps is often required during the operation. Third, the subxiphoidal trocar occasionally impedes the surgeon's hand, thus limiting the surgeon's freedom of movement outside of the abdominal cavity. Finally, the addition of more disposable instruments also adds to the overall cost of the procedure.
In our study, the diameter of the Carter Thompson needle used to pick up the suture attached to the cotton tape was only 1 mm. Further, it did not leave a scar or cause pain after a skin puncture. So far, we have utilized this technique in 20 cases (16 radical nephrectomies and 4 donor nephrectomies). This series also included 2 cases of laparoendoscopic single-site transumbilical surgery. The mean operative time required to complete the liver retraction was 6 minutes 15 seconds (range, 4–15 minutes). No increase in either the aspartate aminotransferase or alanine aminotransferase level after the operation was observed. A conversion to conventional liver retraction procedures was required in one case. There was no perioperative complication related to this technique.
This technique, although simple, may require repetitive needle punctures to accomplish the optimal retraction of the liver. In patients with a hypertrophic right lobe, the liver may not be retracted sufficiently to provide optimal working space. Further, use of this technique sometimes mandates puncturing the diaphragm to provide the optimal liver traction. In such cases, use of traditional 5-mm locking grasper should be preferred rather than our technique.
Our liver traction technique with a cotton tape is safe and simple in laparoscopic right renal surgery. This procedure avoids the need for an additional trocar puncture and can be performed by anyone without requiring any specific techniques. This alternative procedure also has potential applications in single-incision laparoscopic procedures.
Footnotes
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.