
Abstract
Background and Purpose:
Increasing numbers of patients are receiving a diagnosis of thrombophilic conditions necessitating chronic anticoagulation therapy. The best management approach for such patients needing percutaneous nephrostolithotomy (PCNL) has not been established. Discontinuing anticoagulation therapy before PCNL is needed to prevent hemorrhage, placing some of these patients at risk for thromboembolic events. We describe the use of removable inferior vena cava filters (RIVCF) in patients undergoing PCNL who are at risk for a venous thromboembolic event.
Patients and Methods:
A retrospective study of outcomes of PCNL with RIVCF placement was conducted.
Results:
Four patients underwent PCNL with RIVCF placement on the same day of the procedure. The mean age was 49 years (range 35–69 years). PCNL was performed on a total of six renal units with a mean of 2.2 (range 1–3) operations per renal unit. Five of six (83%) renal units were rendered stone free. There were no complications associated with either the PCNL or RIVCF placement. No patient had a thromboembolic event or received blood products. Two of the four patients underwent successful removal of the RIVCF, and one elected to keep the device in place. The device could not be extracted in the other patient. The average length that the filters were in place was 52.5 days. Patients resumed anticoagulation therapy shortly after RIVCF removal.
Conclusion:
RIVCF placement is a safe and effective method of preventing venous thromboembolic complications in thrombophilic patients needing PCNL. Patients should be informed, however, that RIVCF removal is not always possible.
Introduction
The insertion of a removable inferior vena cava filter (RIVCF) is reported to be an effective method of preventing venous thromboembolic complications in thrombophilic patients who need to stop anticoagulation therapy for invasive procedures. 5,6 We report the use of this approach for the treatment of such patients needing PCNL.
Patients and Methods
After approval from the Institutional Review Board at Wake Forest University, the records of four patients needing PCNL who were receiving chronic anticoagulation therapy for prevention of venous thromboembolic events (VTE) were reviewed. RIVCFs were inserted before PCNL by either an interventional radiologist or a vascular surgeon. Bard G2® RIVCFs were used. PCNL was performed using standard techniques with access to the collecting system performed by the urology team. The tract was dilated using a balloon device, and stone removal was undertaken using rigid and flexible nephroscopy, pneumatic/ultrasonic lithotripters, and holmium laser fragmentation.
Nephrostomy tubes were inserted at the end of the cases. Stone-free status was assessed with noncontrast CT. Anticoagulation therapy was restarted 5 days after the last PCNL procedure. Filter removal was performed after nephrostomy tubes were removed and the tracts healed. Screening studies for postoperative deep venous thrombosis (DVT) were not undertaken.
Results
A total of four patients, two men and two women, underwent RIVCF placement. the mean age was 49 years with a range of 35 to 69 years. All patients had a history of recurrent DVT and pulmonary embolism (PE). One patient had a prothrombin gene mutation, one patient was morbidly obese and immobile because of a spinal cord injury, one had immobilization because of spina bifida, and the other had no definable risk factors for VTE. Two patients had unilateral large volume renal stones, and the other two had such stones bilaterally (Figs. 1A, 1B). All patients were receiving warfarin, which was stopped 5 days before PCNL and underwent RIVF placement via a transjugular approach on the day of the PCNL (Fig. 2).

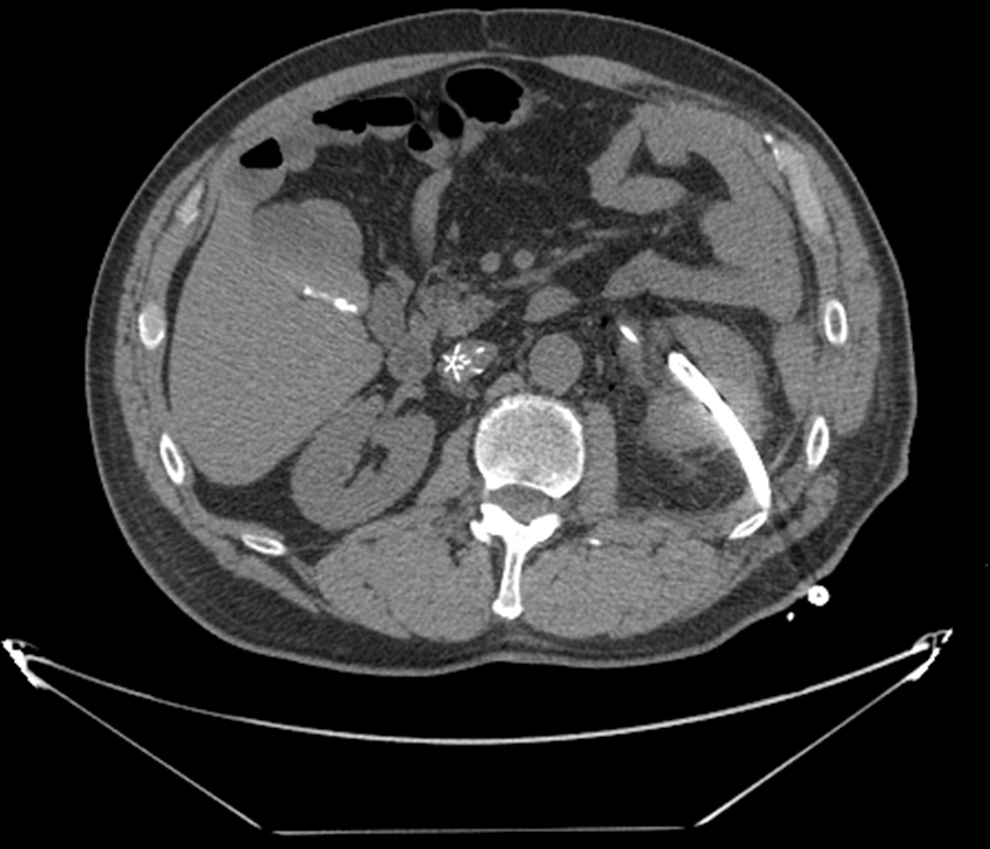
Computed tomography scan performed the day after the procedure demonstrating removable inferior vena cava filter in place.
PCNL was performed in six renal units with a mean of 2.2 procedures per renal unit. One access was used in two patients, two accesses were used in two patients, and three were used in the other. Five of the six (83%) renal units were rendered stone free. The residual stone in the patient who was not rendered stone free was nephrocalcinosis. There were no perioperative complications. Stone composition was uric acid in one, calcium oxalate in one, and struvite in two patients. An attempt at urinary pH manipulation therapy in the patient with uric acid stones was undertaken before PCNL but was not successful.
RIVCFs were placed in all patients without complications. Two of the four patients had successful removal of the filter after their stone treatments on days 34 and 71. Removal of another filter was attempted on day 115 but was not completed for technical reasons. One patient elected not to have the filter removed. There have been no thrombotic complications in the two patients whose filters remain in place.
Discussion
Patients with large volume renal stones and thrombophilia who need stone removal present unique management challenges because these patients are typically receiving anticoagulant therapy to limit the risk of thromboembolic events, which can eventuate in mortality. Some patients with large stones can be treated with shockwave lithotripsy (SWL), but coagulation status and platelet function must be normal when this is undertaken. The timing of restarting anticoagulation after SWL has not been firmly established, but there is a risk of severe hemorrhagic complications if it is restarted shortly after SWL. 7 A flexible ureteroscopic approach with the patient maintained on anticoagulant therapy is another option. A number of case series have demonstrated success in this patient cohort using this technique, but the mean stone sizes were less than 2 cm. 8 –10
While ureteroscopy is reported to be effective in patients with large renal stones, outcomes in patients maintained on anticoagulant therapy are unknown. PCNL is usually the most effective means of removing large renal stones. Similar to SWL, patients must have normal coagulation and platelet function at the time of the procedure. Kefer and associates 11 reported on 27 patients who were receiving anticoagulation or antiplatelet therapy including warfarin, clopidogrel, or cilostazol who underwent PCNL. Warfarin was discontinued 5 days before surgery, and enoxaparin bridging was undertaken. Warfarin therapy was resumed 5 days after PCNL. Clopidogrel and cilostazol were discontinued 10 days before PCNL and resumed 5 days afterward. Five needed two PCNL procedures, and one patient needed three. Twenty-five were rendered stone free. Seven percent had significant bleeding, and one had a thromboembolic event.
We have used an alternative strategy for our cohort—RIVCF placement at the time of the procedure. Our study demonstrates that this may be an effective method of treating these high-risk patients. There are some limitations to this approach, which are subsequently discussed.
Placement of an RIVCF has most commonly been used in patients who have sustained certain types of traumatic injury, who are also at risk for PE, and who are not candidates for prophylactic anticoagulation. This includes patients with severe closed head injury, incomplete spinal cord injury with paraplegia or quadriplegia, complex pelvic fractures associated with long-bone fractures, or those with multiple long bone fractures. 12 TRIVCF has also been used as a prophylactic measure in other cohorts at risk for PE including persons undergoing bariatric surgery. 13
There are a variety of RIVCF devices available that can be inserted percutaneously via the internal jugular or femoral vein. These devices should be removed when the risk of a thromboembolic event has subsided, and this can be safely undertaken even when patients are receiving anticoagulation therapy. 14 Timing is important, because a time interval of greater than 90 days between implantation and attempted removal is associated with retrieval failure. 15 This was illustrated in our series in which retrieval was successful in two patients whose RIVCFs had been in place less than this interval, and retrieval failure occurred in the one patient in whom this interval was exceeded.
Certain complications can occur during and after insertion of an RIVCF device including perforation of the inferior vena cava, filter migration or embolization, filter fracture, and thrombosis or occlusion of the inferior vena cava. 16 A review of 37 studies comprising 6834 patients deemed at high risk for VTE in whom an RIVCF was placed demonstrated that the rate of PE after insertion was only 1.7%. 17 The rates of filter migration and IVC thrombosis were 1.3% and 2.8% in this study.
The 10-year risk of recurrent VTE is reported to be 30%. 18 The risk of mortality from recurrent PE is 11% and 2% for recurrent DVT. 18 Therefore, special precautions need to be taken with patients who have had recurrent VTE. A study comparing the use of enoxaparin and RIVCF for prevention of recurrent VTE has, to our knowledge, not been performed. A study of permanent IVC filter insertion vs enoxaparin therapy in those with proximal DVT, however, demonstrated a significant reduction in the risk of PE (1% vs 4.8 %), no differences in overall mortality, but a higher risk of recurrent DVT in those with the permanent filter. 18 A potential risk in the use of enoxaparin bridging in those undergoing PCNL would be the promotion of hemorrhagic complications. These issues need to be taken into consideration when choosing strategies for preventing recurrent VTE in those undergoing this procedure.
Conclusions
Our limited experience suggests that use of an RIVCF in those undergoing PCNL who are at high risk of a VTE is a feasible option for selected patients. Patients must be informed that these devices may not be retrievable, and there are other potential problems associated with their placement.
Footnotes
Disclosure Statement
No competing financial interests exist.