
Abstract
Background and Purpose:
Considering the potential impact of warm ischemia time (WIT) on renal functional outcomes after robot-assisted partial nephrectomy (RAPN), many techniques that reduce or eliminate WIT have been studied. We present our institutional experience and progression using one such technique—off-clamp RAPN—as well as the results of this technique in the management of complex cases.
Patients and Methods:
A retrospective chart review of 65 patients undergoing off-clamp RAPN was performed, 15 of whom underwent off-clamp RAPN for 26 complex tumors. Complex features included hilar location, completely endophytic growth, and ipsilateral multifocality. In all cases, hilar vessels were dissected but not clamped.
Results:
Mean tumor size was 2.5 cm (standard deviation; [SD]=1.4), while mean nephrometry score was 8.7 (SD=1.5). One (7%) intraoperative complication occurred. Mean estimated blood loss was 403 mL (SD=381), mean operative time was 190 minutes (SD=68), and WIT was 0 minutes in all cases. Mean length of stay was 1.8 days (SD=0.9), with one patient needing a postoperative blood transfusion (Clavien II complication). Final pathology results demonstrated clear-cell carcinoma (n=16), papillary carcinoma (n=4), angiomyolipoma (n=1), oncocytoma (n=2), and cystic nephroma (n=3). Margins were negative for tumor for 96% (25/26) of resected masses. Estimated glomerular filtration rate (eGFR) decreased by an average of 3.1 mL/min/1.73m2 (SD=9.8, P=0.24), at a mean follow-up of 177 days (SD=296). Five patients with radiographic follow-up of at least 6 months have no evidence of disease recurrence.
Conclusions:
Off-clamp RAPN can be safely and effectively performed even in the case of complex tumors, but occurs with higher estimated blood loss. Minimal changes in eGFR were experienced by patients undergoing off-clamp RAPN at an average follow-up of roughly 6 months. Longer follow-up and direct comparison with conventional clamped RAPN technique are needed to establish the efficacy of off-clamp RAPN in complex cases.
Introduction
Renal hilar clamping during minimally invasive NSS is typically performed under warm ischemia conditions. Recognizing the importance of limiting warm ischemia time (WIT) on potential preservation of long-term renal function, 4 –6 various surgical techniques that reduce or eliminate WIT have been described. 7 –13
Over the last 5 years, our institution has performed RAPN without clamping of the renal hilum in selected patients. As our experience has grown, we have applied this technique to increasingly challenging cases. We present our institutional trends regarding off-clamp RAPN and highlight our experience with this technique in the management of complex renal tumors.
Patients and Methods
Retrospective chart review was performed with Institutional Review Board approval. A total of 65 cases of off-clamp RAPN for suspected renal-cell carcinoma (RCC) were identified between August 2007 and May 2012. Among these patients, 15 underwent off-clamp RAPN for 26 “complex tumors” between January 2009 and May 2012. Complex tumors were defined as those with hilar location, completely endophytic growth, and/or multiple ipsilateral masses, following the same criteria as in previously published studies. 14,15 Preoperative CT or MRI demonstrated enhancing renal masses that were suspicious for RCC in all patients. Treatment options were discussed with patients, and selection of off-clamp RAPN was based on tumor size, tumor location, patient comorbidities, and surgeon and patient preference. One patient had known von-Hippel-Lindau syndrome and had undergone previous renal surgery consisting of laparoscopic cryoablation of tumors in the contralateral kidney. No other patients had previous renal surgery.
Surgical technique
In general, RAPN was performed using a transperitoneal approach for anterior tumors and a retroperitoneal approach for posterior tumors. The kidney was mobilized, and perinephric fat overlying the tumor was excised. As a precaution, the renal hilum was exposed, and bulldog clamps were placed in the surgical field to enable prompt vascular control. Of note, the renal hilar dissection included only the main renal vessels; no segmental arteries were dissected. No hilar, segmental, or selective arterial occlusion was performed. Tumor depth was assessed with the aid of intraoperative robotic ultrasonography (Aloka, Wallingford, CT), in conjunction with the da Vinci Surgical System TilePro feature (Intuitive, Sunnyvale, CA).
With monopolar electrocautery set to 35 W, the resection site was demarcated circumferentially and tumor excision was performed. Tumor excision was started nearest to the largest vessels, and the mass was mobilized away, presumably leading to diminished tumor perfusion as excision progressed. As the plane of dissection was advanced, the resection base was meticulously cauterized to ensure hemostasis. If during resection vessels were seen directly entering the tumor from the resection bed, they were selectively clipped with Weck Hem-o-lok clips (Teleflex, Research Triangle Park, NC). In addition, if large vessels within the resection bed remained patent despite electrocautery, then the resection bed vessel was temporarily occluded using the Prograsp forceps (Intuitive, Sunnyvale, CA), followed by direct application of the robotic bulldog clamp to the resection bed.
Once tumor resection was completed, the patent vessels within the resection bed were identified and ligated with 2-0 polyglactin or Weck Hem-o-lok clips. If the collecting system was entered, repair was performed with a running 2-0 polyglactin suture, which was secured with intracorporeal knots. Reapproximation of the renal parenchyma was performed using the sliding-clip renorrhaphy technique. 16 Hemostasis of the resection bed was carefully assessed by decreasing the insufflation pressure to 5 mm Hg. In a few instances where slow venous bleeding continued, Floseal (BioSurgery, Deerfield, IL) and/or Surgicel Nu-knit (Ethicon, Cincinnati, OH) were applied to enhance hemostasis. Tumors were extracted with an Endo Catch specimen bag (Covidien, Mansfield, MA). The gross margins of the tumor were inspected intraoperatively, and then the specimen was sent for permanent section.
Data collection and analysis
Patient demographics, tumor characteristics, perioperative information, and postoperative serum creatinine level were recorded. Baseline comorbidities were assessed using the American Society of Anesthesiologists (ASA) classification and the Charlson Comorbidity Index (CCI). 17,18 Nephrometry score was calculated for all tumors. 19 Nephrometry scores of 4 to 6 were considered low, 7 to 9 were considered mid, and 10 to 12 were considered high. Estimated glomerular filtration rate (eGFR) was calculated using the Chronic Kidney Disease Epidemiology Collaboration formula. 20 Postoperative complications were recorded and classified by Clavien-Dindo grade. 21 The t test was used to compare pre- and postoperative eGFR. Statistical analysis was performed using QuickCalcs (GraphPad Software, La Jolla, CA).
Results
A summary of off-clamp RAPN cases performed at our institution by year and organized by nephrometry score is provided in Table 1.
RAPN=robot-assisted partial nephrectomy; neph.=nephrometry.
Year to date (January to May 2012).
The tumor features associated with each complex case are summarized in Table 2. Preoperative imaging of representative complex off-clamp RAPN cases are provided in Figure 1.
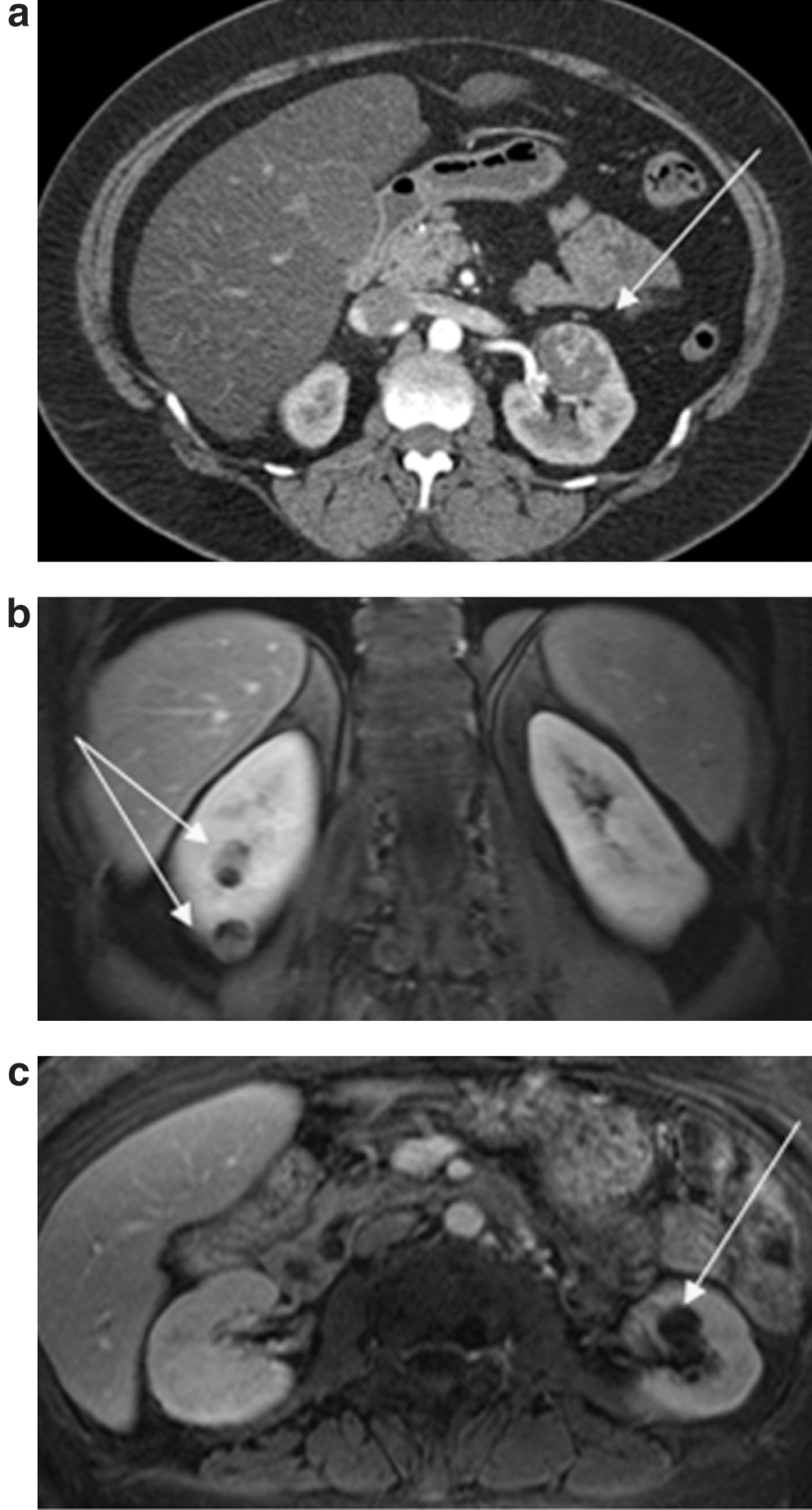
The above images represent complex robot-assisted partial nephrectomy cases performed using the off-clamp technique.
Patient and tumor characteristics for complex and non-complex cases are summarized in Table 3. For the complex cases: Mean patient age was 59 years ([SD]=11, range 37–73), mean ASA classification was 2.5 (SD=0.6), mean CCI was 2.4 (SD=1.1), mean preoperative eGFR was 81.8 mL/min/1.73 m2 (SD=25.3, range 23.8–128), mean tumor size was 2.5 cm (SD=1.4, range 0.8–5.5), and mean nephrometry score was 8.7 (SD=1.5, range 6–11).
SD=standard deviation; BMI=body mass index; ASA=American Society of Anesthesiologists; CCI=Charlson Comorbidity Index; eGFR=estimated glomerular filtration rate.
Perioperative, functional, and oncologic outcomes for complex and noncomplex cases are summarized in Table 4. WIT was 0 minutes in all cases. For the complex cases: Mean operative time was 190 minutes (SD=68, range 106–353), mean estimated blood loss (EBL) was 403 mL (SD=381, range 50–1500), intraoperative complication rate was 7% (1/15), mean hospital stay was 1.8 days (SD=0.9, range 1–4), postoperative complication rate was 7% (1/15), and surgical margins were negative in 25/26 (96%) tumors. The intraoperative complication consisted of a patient going into atrial fibrillation near the end of the case. She had a known history of intermittent atrial fibrillation. She was taken to the intensive care unit on completion of the case, medically converted to sinus rhythm, and discharged after 2 days. The postoperative complication consisted of a patient with eight ipsilateral masses (EBL=1500 mL) necessitating a postoperative blood transfusion (Clavien II).
SD=standard deviation, RCC=renal-cell carcinoma, eGFR=estimated glomerular filtration rate.
=Among patients with imaging follow-up of at least 6 months.
Mean postoperative eGFR was 78.6 mL/min/1.73 m2 (SD=22.6, range 22.8–121) at a mean follow-up of 177 days (SD=296, range 1–1157) for the complex cases and was 75.4 mL/min/1.73 m2 (SD=27.6, range 8.2–131) at a mean follow-up of 259 (SD=302, range 1–1007) for the noncomplex cases. In both the complex and noncomplex groups, the mean change in eGFR represented a statistically insignificant decline (complex mean ΔeGFR=−3.1 mL/min/1.73 m2, P=0.24; noncomplex mean ΔeGFR=−2.0 mL/min/1.73 m2, P=0.17). Of patients with greater than a 6-month radiographic follow-up, none has evidence of recurrence or metastatic disease (0/27), with mean follow-up of 355 days (SD=298, range 191–887) for the complex cases and 492 days (SD=248, range 202–921) for the noncomplex cases.
Discussion
The adoption of robotic technology in the treatment of patients with renal tumors has helped surgeons overcome many technical limitations of LPN, facilitating wider use of minimally invasive NSS. 22 Without compromising oncologic control, RAPN has demonstrated shorter WIT compared with traditional LPN. 3 Nevertheless, because of the potential impact of even limited WIT on the preservation of long-term renal function, 23 methods to further diminish or eliminate WIT have been under investigation. 8 –13
As our experience with off-clamp RAPN has grown, we have used this technique in an increasing number of cases and increasingly challenging tumors. During 2007 to 2010, off-clamp RAPN was selectively applied at our institution—two in 2007, five in each year 2008 to 2010—comprising less than 10% of the total RAPN volume. In addition, during this time period, most off-clamp RAPN cases involved tumors with a low nephrometry score (82%). In 2011, a total of 21 off-clamp RAPN cases were performed, accounting for 13% of the total RAPN volume at our institution. Of the off-clamp RAPN cases, 57% (12/21) had mid or high nephrometry scores, and 33% (7/21) involved tumors with complex features. In 2012, a total of 27 off-clamp RAPN cases have been performed to date (January to May), accounting for 33% of the total RAPN volume at our institution. Of the off-clamp RAPN cases, 67% (18/27) had mid or high nephrometry scores, and 26% (7/27) involved tumors with complex features.
Although consensus definitions for tumor complexity continue to evolve, 19,24,25 we have used criteria found in previously published studies. 14,15 Endophytic growth, hilar location, and multifocal ipsilateral presentation are ostensibly challenging for RAPN and furthermore for off-clamp RAPN. Because these complex cases may represent an obstacle to the wider application of the off-clamp RAPN technique, we sought to examine our own results using this technique for complex tumors.
We expected that the perioperative results of these complex cases would differ from that of noncomplex cases within our off-clamp RAPN experience. The mean tumor sizes among our 50 noncomplex cases, however, were very similar to those of our 15 complex cases: 2.6±1.4 vs 2.5±1.4 cm, respectively. Mean operative time and EBL for noncomplex cases were 149 minutes and 195 mL compared with 190 minutes and 403 mL for complex cases. Still, this difference did not seemingly affect the immediate postoperative course of patients, because length of hospital stay was similar for both groups: 1.8±0.9 vs 1.9±1.0 days, respectively. In addition, postoperative complication rates were similar regardless of case complexity, 7% (1/15) for complex and 4% (2/50) for noncomplex cases. Furthermore, mean eGFR decline experienced by the complex group was not significantly different from the decline experienced by the noncomplex group (3.1 vs 2.0 mL/min/1.73 m2; P=0.7). This comparison, however, may be underpowered to detect a significant difference between these groups, and the increased eGFR decline in the complex group could be related to the increased EBL experienced by those patients (403 vs 195 mL).
Comparison of our complex off-clamp experience with that of others performing traditional clamped RAPN for complex tumors may elucidate the major benefits and drawbacks to performing RAPN without hilar clamping in complex cases. Both Gong and associates 14 and Rogers and colleagues 15 report on their experience with traditional clamped RAPN for complex tumors. Mean operative times and EBL reported by Gong and associates 14 and Rogers and colleagues 15 were 197 and 192 minutes, 220 and 230 mL, respectively. Our experience with off-clamp RAPN for complex tumors demonstrates similar mean operative time (190 min) but substantially higher mean EBL (403 mL), which is to be expected with no occlusion of the renal hilum during resection. Importantly, despite the increased blood loss in our off-clamp series, only one (7%) patient needed a blood transfusion postoperatively. The mean declines in eGFR reported by Gong and associates 14 and Rogers and colleagues 15 were 4.5 and 5.6 mL/min/1.73 m2, respectively. The mean decline in eGFR after off-clamp RAPN in our series was 3.1 mL/min/1.73 m2, which may not represent a clinically or statistically significant difference.
Another difference between our series and that of Gong and associates 14 and Rogers and colleagues 15 was the positive surgical margin rate. All surgical margins were negative in their studies, using traditional clamped RAPN for complex tumors. The present study of off-clamp RAPN for complex tumors, however, had negative surgical margins in 25 of 26 tumors. The positive surgical margin occurred in the smallest tumor of the patient undergoing resection of three ipsilateral masses (2.1, 1.5, and 0.8 cm), which were found to be papillary RCC. The boundaries of the tumor were adequately visualized with intraoperative ultrasonography at the time of resection. After tumor excision, the resection bed was carefully examined, appeared to be free of tumor, and was thoroughly fulgurated. On extraction, the specimen was sectioned by pathology associates in the operating room, which grossly showed that the tumor was confined to its pseudocapsule; however, final pathology results demonstrated tumor abutting the inked margin. Studies have suggested that after LPN, positive surgical margins are not always indicative of residual disease. 26 The patient has elected monitoring, and cross-sectional imaging will be performed in 6 months.
Because many of our complex off-clamp RAPN cases were performed recently, oncologic outcomes are not yet mature in all of our patients. Five of the 15 patients have greater than 6-month follow-up imaging (mean follow-up of 355 days), and all five patients have no evidence of local tumor recurrence or metastatic disease.
Limitations to our study include limited renal functional follow-up and small sample size. To completely describe our perioperative outcomes, patients who were very recently treated with off-clamp RAPN for complex tumors were also included. Moreover, of our 65 total cases of off-clamp RAPN, application of this technique to complex tumors has been relatively recent, as we have continued to gain confidence with our experience. As a result, the length of renal functional follow-up for our cohort ranges from 1 to 1157 days. Our strict definition for tumor complexity as well as the aforementioned recent application of off-clamp RAPN to complex tumors has resulted in a small sample size, which may also limit broader interpretation of our results.
As we continue to gain more experience with off-clamp RAPN and apply this technique to increasingly complex tumors, larger studies should be performed to better and more fully determine the impact of tumor complexity on surgical outcomes. Multi-institutional collaboration to recruit sufficient numbers of patients may also be needed to facilitate this assessment. Importantly, distinguishing the impact of the off-clamp technique on perioperative, renal functional, and oncologic outcomes for complex tumors ideally requires a prospective, randomized comparison between off-clamp RAPN and conventional clamped RAPN. Finally, large prospective studies evaluating perioperative outcomes and complication rates after RAPN for the treatment of increasingly challenging tumors can be used to validate definitions of complexity.
Conclusions
Off-clamp RAPN for complex tumors resulted in minimal changes in eGFR at roughly mean 6-month follow-up. All patients with imaging follow-up greater than 6 months postoperatively showed no evidence of disease. Perioperative outcomes were generally similar between our complex and noncomplex off-clamp RAPN cases, except with greater blood loss in our complex group. Our results were also comparable to single institution series reporting outcomes of complex cases treated with conventional RAPN. Although blood loss is more substantial in our complex off-clamp RAPN cohort, we believe with more experience performing the off-clamp technique, case complexity minimally impacts perioperative and functional outcomes after off-clamp RAPN.
Footnotes
Disclosure Statement
No competing financial interests exist.