
Abstract
Objectives:
Lymphocele development is the most frequently reported postoperative complication of pelvic lymph node dissection (PLND) performed with laparoscopic radical prostatectomy (LRP). This study evaluated the efficacy of a vessel-sealing device (VSD) for the prevention of lymphocele development.
Methods:
A total of 120 patients who underwent LRP with PLND were prospectively enrolled. The patients were randomly assigned to one of the two groups: PLND using a conventional technique (group 1), and PLND performed with VSD (group 2). All patients underwent computed tomography (CT) scanning 1 month postoperatively to evaluate the maximum sectional area of the lymphoceles.
Results:
Lymphoceles developed in 63 cases (52.5%). One case (0.8%) was symptomatic with infection, and drainage tube placement was required. In the other 62 patients, the lymphoceles developed asymptomatically and were detected by CT scanning. There was no significant difference in the lymphocele development ratio between the two groups. However, when we defined a lymphocele over 1500 mm2 as being a significant size, lymphoceles were present in 16 of 60 patients in group 1 and 4 of 60 patients in group 2. The incidence of significant lymphoceles over 1500 mm2 in the group using VSD was much lower than that of the group without VSD (p<0.01). Multivariate analysis demonstrated that VSD was the only independent factor that had an effect on preventing the development of lymphoceles over 1500 mm2 (p<0.01, odds ratio=4.96).
Conclusion:
The results indicate that the development of large lymphoceles can be prevented by using VSD in LRP with PLND.
Introduction
The occurrence of lymphoceles is the most frequently encountered postoperative complication after lymph node dissection. 6,7 The rate of lymphocele development reported after open PLND ranges from 1.3% to 60%. 8,9 The incidence of lymphoceles after LRP and robot-assisted radical prostatectomy may be higher because of the difficulty associated with binding lymphatic vessels. Infection of lymphoceles often requires hospital care, and causes a significant reduction in a patient's quality of life. However, a reliable method for preventing lymphocele development has not yet been established. Simonato et al studied the efficacy of TachoSil® (an equine collagen patch coated with fibrin glue components) for preventing lymphocele development, 10 while Scholz et al demonstrated that fibrin glue did not reduce lymphocele development. 11 Some case reports have documented the efficacy of vessel-sealing devices (VSD); however, to the best of our knowledge, there have been few prospective studies of the efficacy of VSD. In this study, we therefore prospectively evaluated a VSD (EnSeal®) as a treatment for reducing lymphocele development.
Materials and Methods
This was a prospective study. A total of 120 patients who had undergone LRP with PLND that was approached via an extraperitoneal space from April 2010 to July 2011 were prospectively enrolled. Approval from the Institutional Review Board of the Keio University Hospital was obtained, and patients involved in the study signed a written informed consent form to participate before enrollment. All patients were randomly assigned to one of two groups: PLND using a conventional technique (group 1) and PLND performed with VSD (EnSeal) (group 2).
All surgical procedures were performed by 3 high-volume surgeons (A.M., M.H., and T.T.). The lymphadenectomy was always performed according to the same procedure.
Surgical technique
Laparoscopic PLND was performed via an extraperitoneal approach using five ports. Insufflation pressure was typically maintained at 10 mm Hg during an operation. The bilateral dissection was limited to the lymph nodes along the external iliac vein and the obturator fossa. Ultrasonic cutting and a coagulating system (SonoSurg®) were used to perform cutting and coagulation simultaneously in PLND, and we routinely used ultrasonic cutting and a coagulating system to occlude blood and lymphatic vessels before transection of the tissue. In the group in which a VSD was used, VSD was used as an alternative to the ultrasonic cutting and coagulating system.
At the end of surgery, an 8-mm drainage tube was placed in the prevesical space. The tube was removed when the drainage volume decreased to <100 mL per day, and in many cases was removed on postoperative day 1.
Endpoints
All patients underwent computed tomography (CT) 1 month postoperatively to evaluate the sizes of the lymphoceles. When a lymphocele was detected by CT, we measured the area in the maximum plane of the lymphocele, and defined a lymphocele over 1500 mm2 as being of significant size. Prophylactic antibiotic administration (levofloxacin hydrate 500 mg/day for 14 days) was started in patients with lymphoceles over 1500 mm2. All the patients were followed-up for at least 6 months. The median follow-up period was 14.8 months.
Statistical analysis
The correlation between lymphocele development and various factors [age, body–mass index (BMI), prostate weight, operation time, estimated blood loss (EBL), number of lymph nodes removed, positive lymph node status, PSA, preoperative Gleason score, clinical stage, presence of nerve sparing, and the use of VSD] was analyzed by the chi-square test or the Student's t-test. Multivariate analysis was used to identify independent factors that were associated with significant lymphocele development by logistic regression analysis. A two-sided p<0.05 was considered to be statistically significant.
Results
The characteristics of the patients are shown in Table 1. The mean (range) patient age was 65.2 (49–75) years, and the mean PSA level was 9.4 (2.4–19.6) ng/mL. The mean operation time and EBL were 234 (108–362) minutes and 284 (50–1050) mL, respectively. The average time required for PLND was 20 minutes, which corresponded to 7% of the entire operation time. The mean number of lymph nodes removed was 11.2 (4–43); the mean number was 5.1 on the right side and 6.1 on the left side. The number of patients with a Gleason score of 5–6, 7, and 8–10 in the postoperative pathology was 26, 77, and 17, respectively. The clinical stage was T1c in 35 and T2 in 85. The overall incidence of positive lymph nodes was 2.5% (3 cases). The patient characteristics in the two groups are shown in Table 2. There were no significant differences in the patient characteristics between the two groups.
BMI=body–mass index; EBL=estimated blood loss; LN=lymph node; PSA=prostate-specific antigen.
CT scanning at 1 month after operation detected lymphoceles in 63 (52.5%) patients. Lymphocele development was on the right side in 49 cases, left side in 32 cases, and bilateral in 18 patients. Only one (0.8%) patient in group 1 required drainage tube replacement as an inpatient due to a symptomatic infectious lymphocele; the other lymphoceles developed asymptomatically.
Lymphoceles developed in 35 patients in group 1 (58.3%), and in 28 patients in group 2 (46.6%) (Table 3). There was no significant difference in the lymphocele development ratio between the two groups (Fig. 1).
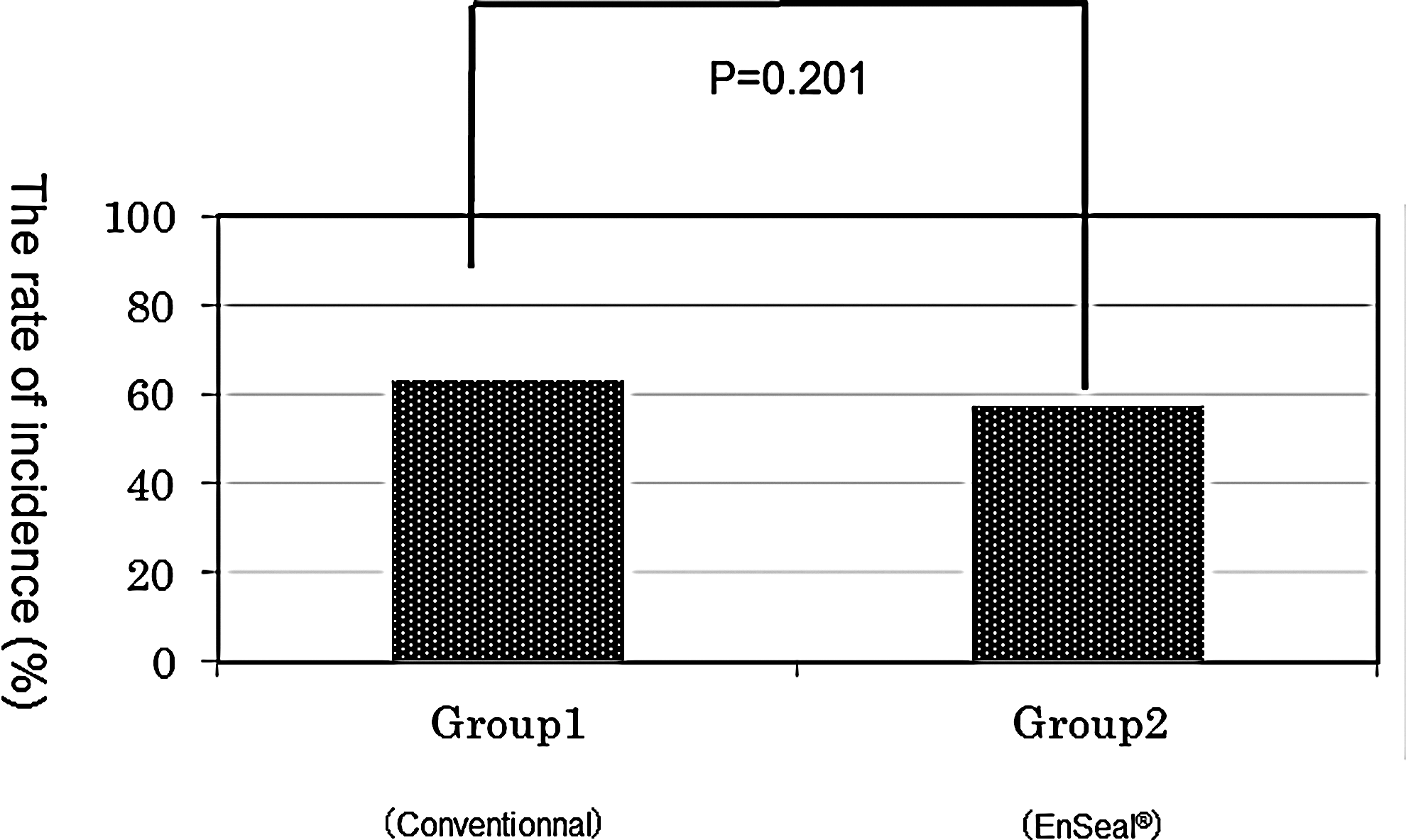
Lymphoceles developed in 35 patients in group 1 (58.3%) and in 28 patients in group 2 (46.6%). There was no significant difference in the lymphocele development ratio between the two groups.
Significant at 5% level (p≤0.05).
The mean of the maximum sectional area was 1335±1457 mm2 (mean±SD). It was greater in group 1 than in group 2, and there was a significant difference (p=0.049). When we defined lymphoceles over 1500 mm2 as being a significant size, the incidence of significant lymphocele development in group 2 was much lower than that in group 1 (p<0.01; Fig. 2).
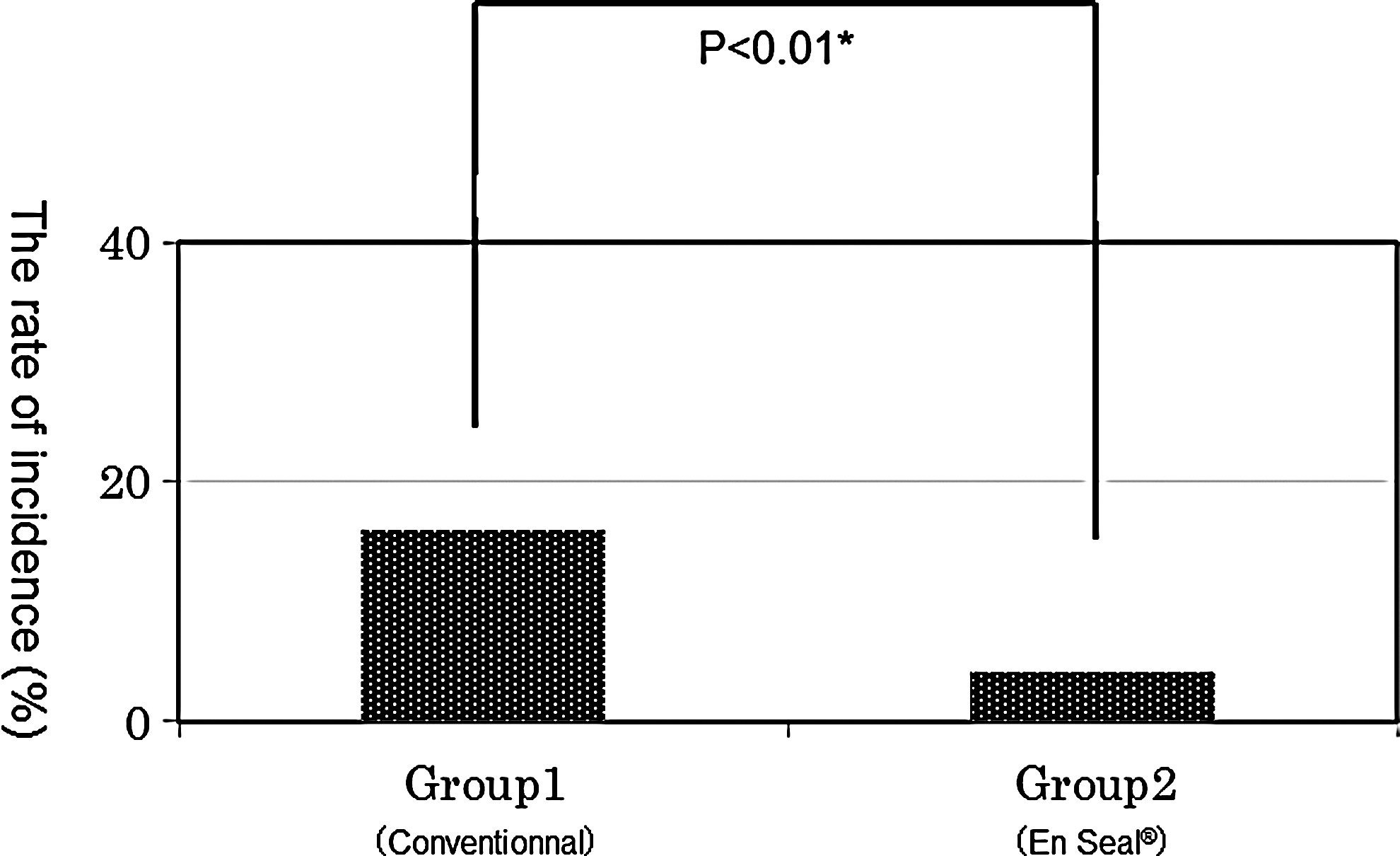
Lymphoceles exceeding 1500 mm2 developed in 16 of 60 patients in group 1 (26.6%) and in 4 of 60 patients in group 2 (6.7%), and the incidence of significant lymphocele development in group 2 was much lower than that of group 1 (p=0.003).
Univariate analysis identified the use of VSD as a factor that correlated significantly with the occurrence of lymphoceles over 1500 mm2. Age, BMI, prostate weight, operation time, EBL, the number of lymph nodes removed, positive LN status, PSA, preoperative Gleason score, clinical stage, and presence of nerve sparing were not significantly different between the two groups. Multivariate analysis revealed that the use of VSD was the only independent factor to prevent the occurrence of significant lymphoceles (p<0.01, odds ratio=4.96). No other independent factors were identified (Table 4).
The factor that showed p<0.2 in univariate analysis was used to perform multivariate analysis (No. of LN removed, clinical stage, and use of VSD).
Significant at 5% level (p≤0.05).
VSD=vessel-sealing device.
Discussion
Lymphocele development after PLND is the most common surgical complication. 6,7 Augustin et al reported that clinical lymphoceles occurred in 6% of patients who underwent PLND and that 2.9% of them needed drainage. 12 Orvieto et al reported that the incidence of lymphocele development was 51% in a study of lymphoceles after robot-assisted PLND via a transperitoneal approach. 13 They reported that symptomatic lymphoceles occurred in 15.4% of patients and 1.3% needed drainage. Gotto et al evaluated 776 patients who underwent PLND during LRP and found that the incidence of symptomatic lymphocele development was 8.1%. 14 In a study by Solberg et al, the incidence of lymphoceles after open PLND performed via an extraperitoneal route was 61%, and the incidence after laparoscopic PLND via a transperitoneal approach was 37%. Symptomatic lymphoceles occurred in 3.2% of patients, all in the open PLND group. In this study, we evaluated the incidence of lymphoceles after laparoscopic PLND via extraperitoneal approach, and found a 54.1% incidence of lymphoceles and a requirement for drainage in 0.8% cases. Like other reports, most lymphoceles remain asymptomatic in spite of the high incidence after PLND. Although the incidence of symptomatic lymphoceles is not high, once they occur, lymphoceles may cause the patient to suffer from fever and pain. Geoffrey et al reported that 76% of the patients with symptomatic lymphoceles visited an ER, and readmission was required in 57%. 14 Some studies have described the relationships between lymphoceles and deep venous thrombosis and pulmonary embolism. Eifler et al evaluated 770 patients who underwent LRP, and reported that the overall incidence of venous thromboembolism (VTE) was 7 of 770, and that all 7 patients in whom VTE developed had undergone PLND, while none in whom PLND was omitted experienced VTE. 15 The decrease in large lymphoceles by using VSD may lead to decreases in the number of both symptomatic lymphoceles and potential VTE.
Our analysis indicates that there was no significant difference in the number of lymphoceles between the two groups. However, in the VSD group, the development of lymphoceles over 1500 mm2 decreased significantly. This result suggests that VSD may be able to seal a portion of the lymphatic vessels, thereby reducing the leakage of lymph. Several reports have assessed the risk factors for the development of lymphoceles. 14,16 However, to the best of our knowledge, only a few studies, in particular prospective studies, have examined VSD for the prevention of lymphocele development.
In the present study, we measured the sizes of the lymphoceles by a computer, and defined a lymphocele over 1500 mm2 as being a significant size, because the average was 1335 mm2. A few studies stratified the lymphoceles according to size, and most of these articles defined the size of a lymphocele as the major axis or the major axis×minor axis. 8,10,17 However, there are lymphoceles whose size cannot be approximated based on an oval shape, and their evaluation is less accurate compared to measuring the area by a computer.
It was reported that the number of lymph nodes removed can help predict the development of lymphoceles. 14,18 However, there was no significant correlation between the number of lymph nodes and lymphocele development in our univariate and multivariate analyses. Similarly, there was no significant difference between the number of lymph nodes and the development of lymphoceles >1500 mm2. The number of lymph nodes removed in the present study was compatible with other reports 15,18 Further data will be needed to assess the influences of the quantitative and qualitative aspects of lymph nodes upon the development of lymphoceles.
Conclusion
The present results indicate that the development of large lymphoceles can be prevented by using VSD in LRP with PLND.
Footnotes
Disclosure Statement
None of the authors have any conflicts of interest or financial ties that should be disclosed.