
Abstract
Background:
Although many studies address the learning curve for robot-assisted laparoscopic prostatectomy (RALP), little is known concerning the results for pelvic lymph node dissection (LND) during RALP.
Patients and Methods:
Between 2006 and 2011, two surgeons performed 904 RALP procedures. LND was performed in 440 (48.6%) cases based on the European Association of Urology guidelines. Both surgeons had extensive experience with open LND for both prostate and bladder cancer. Clinical data were prospectively recorded into an online database. Complications were reported using the Clavien-Dindo system and documented prospectively.
Results:
For both surgeons, the operative time for LND decreased over time during the first 150 LND procedures. After that, a mean plateau of operative time of 49 minutes for LND was reached. Nodal yield increased from a mean of 10 nodes for the first 50 cases to 14 for cases 351 to 400. The percentage of positive nodes increased significantly in these intervals from 4% to 23.1% (P<0.001, Mann Whitney U test). Overall complications by grade were not significantly different between RALP with or without LND. In 440 LND cases, 5 (1.5%) grade IIIb complications occurred. All were infection related with bowel perforation in one. Symptomatic lymphoceles necessitating drainage were present in five (1.5%) men. Thromboembolic events (0% vs 1.5%) and anastomosis dehiscence (0.2% vs 1.1%) were more common in men with LND. During the learning curve, the incidence of Clavien grade I and II but not grade III and IV complications decreased.
Conclusion:
An improvement pattern for LND during RALP is observed for operative time, nodal yield node positivity rate, and complication rate during the first 400 cases of LND.
Introduction
Many studies have evaluated the different aspects of the learning curve of RALP (Table 1). Although extended LND was shown to be possible during RALP, 5,6 no data are available on the learning curve effects of the introduction of robot-assisted surgery to LND. We assess the improvement pattern of pelvic LND during RALP in a single center. The following end points were analyzed: Operative time for LND, number of removed nodes, percentage of patients with detected nodal metastases, and percentage of men with complications.
OR=operating room.
Patients and Methods
The robot-assisted surgery program using the da Vinci S Surgical System (Intuitive Surgical, Sunnyvale, CA) started in 2006. Two surgeons were trained in robotic surgery in dry laboratory conditions and corpses, and both had performed more than 50 open prostatectomy procedures but had no previous experience with laparoscopic prostatectomy. Patients with localized prostate cancer were offered the options of surgical and radiotherapeutical treatment. All prostatectomies performed in the study period at our hospital were done by RALP. LND was performed with the consent of the patient after assessing the nodal metastases risk (>7%) based on the Roach 7 risk calculator and the Briganti nomogram 8 ; the highest risk score of the two nomogram predictions was used. Patients were informed of the side effects of LND in combination with the prostatectomy such as an increased operative time of 1 hour, increased risk of lymphocele formation, and a possible risk of the need for longer drainage.
LND
The LND was performed after removal of the prostate but before reconstruction of the bladder-urethral anastomosis. Node dissection was aimed at removal of nodes at the following locations: (a) External iliac artery area (medial from the genitofemoral nerve, distal from the ureteral crossing, proximal to the epigastric vessels); (b) the obturator/internal iliac area (medial and dorsal from the external iliac, onto the internal iliac artery proximal, down to the endopelvic fascia remnants distally, and dorsally up to the perirectal fat).
Tissue from nodal dissection areas was submitted for pathology analysis in two packages (left and right). The pathologist manually isolated the nodal tissue from their surroundings. Fragmented nodal tissue was counted as one node in the package. The periprostatic tissue was examined for the presence of lymph nodes manually. When nodes were present, these were added to the nodal yield value.
After reconstruction of the bladder-urethral anastomosis, a drain was placed from right to left in the prevesical space and left in place until drain production was less than 50 mL per 24 hours. Patients received a transurethral catheter for 7 to 10 days. Cystography was performed, and, when leak free, the transurethral catheter was removed. Imaging diagnostics were considered in patients with fever or abdominal pain in the postoperative period.
Statistics
For analysis of the performed LND, the population was analyzed sequentially in patient groups containing 50 men for the following end points: Operation (console) time for LND, number of removed nodes, percentage of patients with detected nodal metastases. The operative time for both prostatectomy and nodal dissection was recorded separately, and the number of nodes removed, as assessed by pathologic analysis, was obtained from the pathology report. For analysis of complications, Clavien-Dindo 9 scoring was used within the 90 day postoperative period. To compare numbers of removed nodes during the first 440 cases, a regression analysis was applied. No routine imaging for lymphoceles was conducted, but imaging diagnostics (abdominal ultrasonography or CT/scan) were considered in patients with fever or abdominal pain in the postoperative period. Because we assumed that the performance of LND would benefit from experience gained by doing a RALP without LND, the data were analyzed for both total number of RALPs performed as well as number of robot-assisted LNDs performed.
Results
The patient characteristics are given in Table 2. From the population of n=904 RALP procedures, 440 (48.6%) men underwent LND. Over time, neither a significant difference in case-mix with respect to d'Amico risk group nor a change in percentage of men with LND was observed (Fig. 1). Despite this absence of a significant difference, Figure 1 shows a tendency to lower nodal dissection rates in the first 100 RALP cases. No significant difference in operative time (median and interquartile range [IQR]) (median 82 [59–124], 92 [67–131] min, P=0.63, Mann-Whitney U), lymph node yield (median 12.9 [6–19] vs 11.2 [7–18] nodes, P=0.06), and complication rate between the two surgeons was observed (number of prostatectomies: n=720, n=184; number of LNDs: n=363, n=77). The initial prostate-specific antigen (PSA) value at the first postoperative follow-up (interval 2–4 mos) was not significantly different for study groups of 50 consecutive patients (P=0.642, Kruskal Wallis test for comparing first postoperative PSA values among the seven sequential groups of patients).
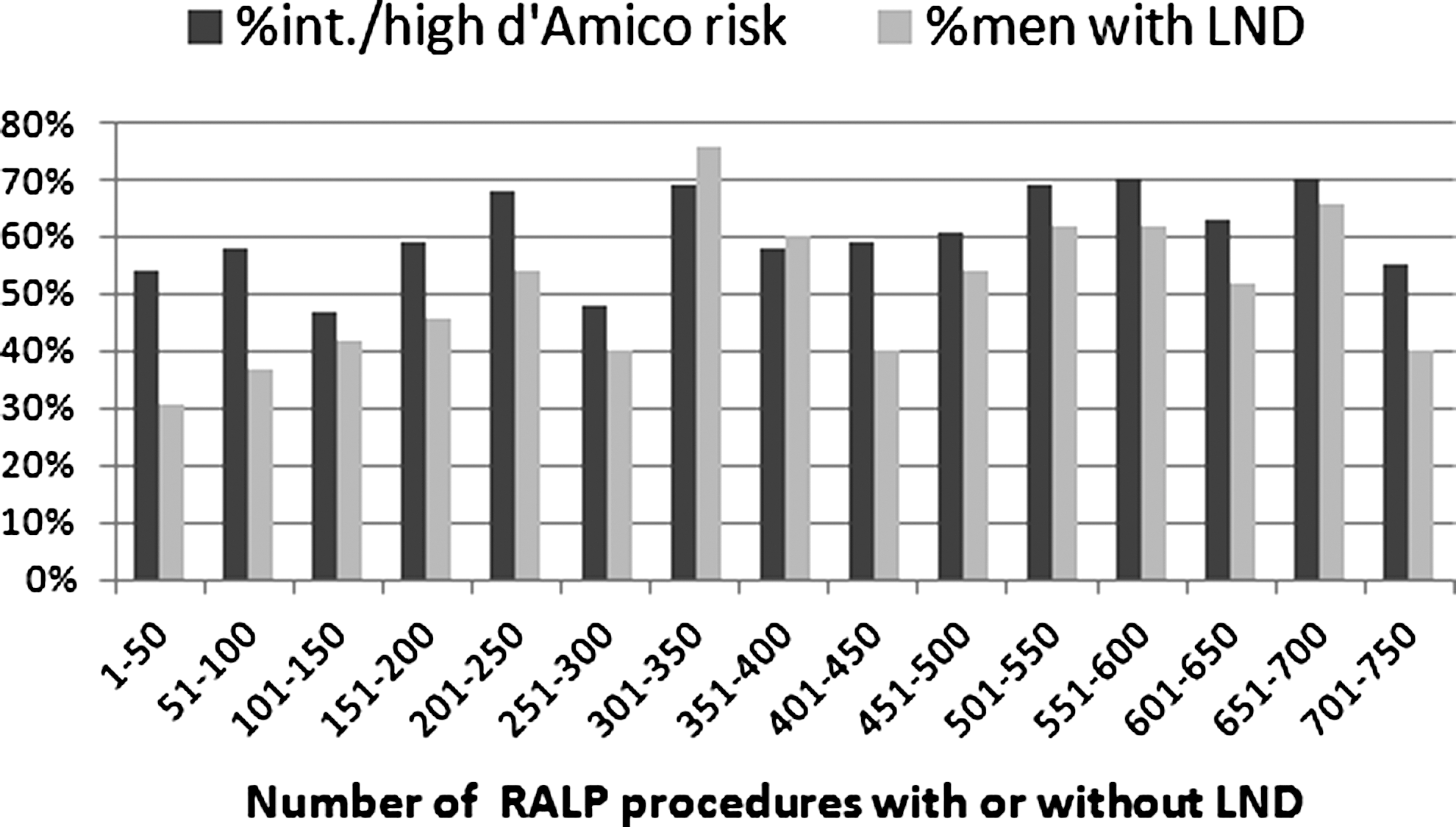
Percentage of patients with intermediate and high d'Amico risk group tumors and percent of men who underwent lymph node dissection by learning curve subgroup.
LND=lymph node dissection; PSA=prostate–specific antigen.
Operative time
The mean operation (console) time for LND of both surgeons improved during the first 200 RALP cases and 150 LND procedures (Fig. 2). The median time for LND decreased from 108 minutes (IQR: 31–133) to 49 minutes (IQR: 27–61) after 150 cases and subsequently remained stable.
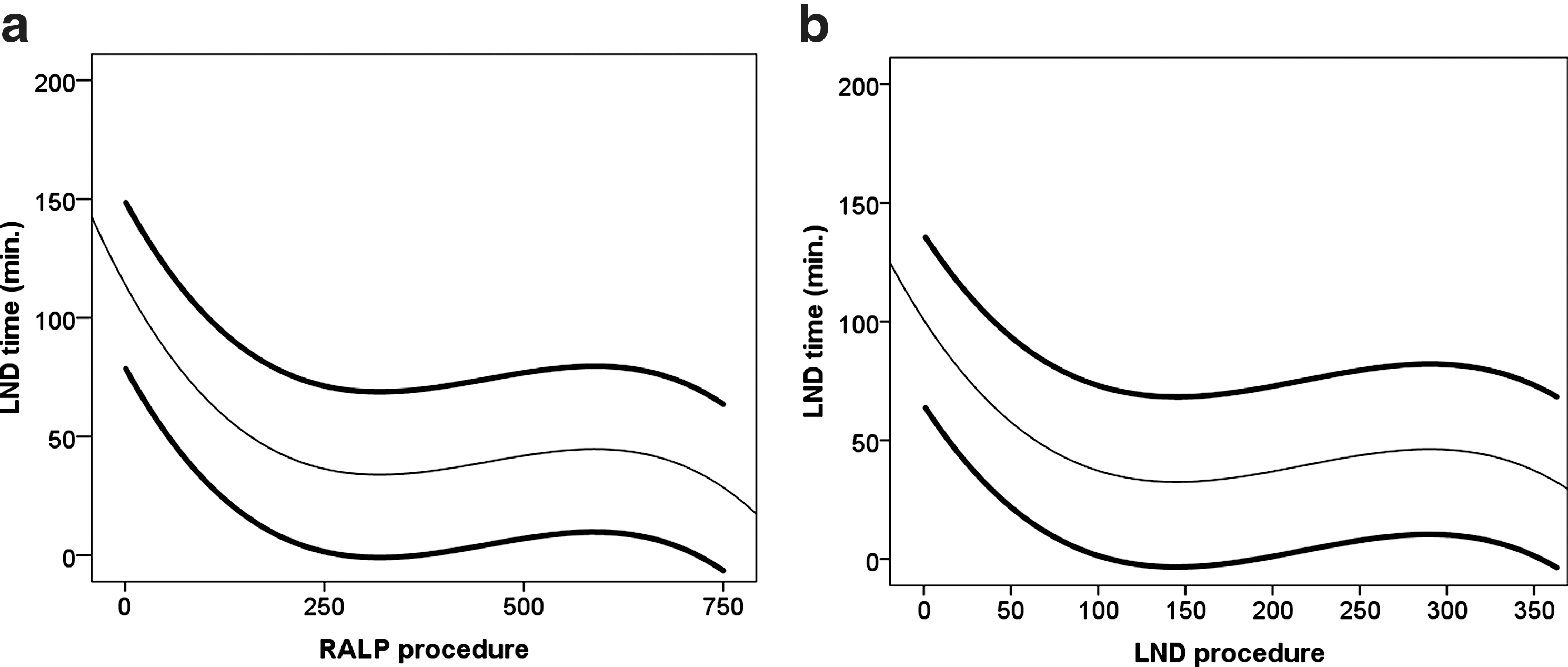
Operative time (min) for lymph node dissection (LND) during robot-assisted laparoscopic prostatectomy (RALP) for the entire population
Number of removed nodes
The number of removed nodes increased gradually over the study period from a median 10 (5–30) in the initial 50 cases to 18 (6–22) in case numbers 351 to 400. Variation in removed nodes among RALP procedures remained large from beginning to end of the study period, but the median value stabilized around 14 (11–19) after 250 cases of RALP with LND (Fig. 3a).
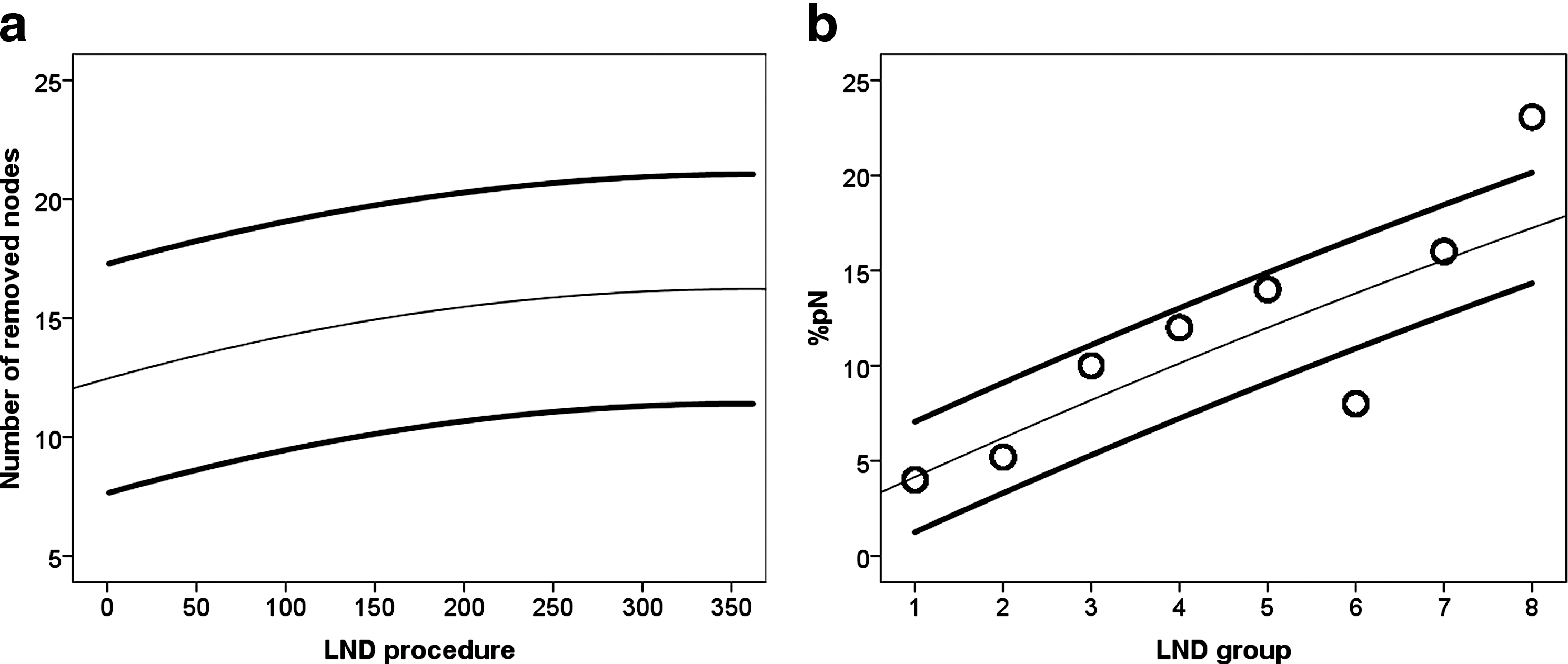
Number of removed lymph nodes by sequential procedure
Node positivity rate
Overall nodal metastases were found in 37 (8.4%) men of those who underwent RALP with LND. The percent of men with positive nodes increased from 4.0% in the initial 50 cases to 23.1% in cases 351 to 400 (P<0.0001, Mann Withney U test comparing the nodal metastases rate in the first 50 men with the last 50 men of the series, Fig. 3b). In a multivariate logistic regression analysis, cT and the number of removed nodes were independent predictors of detection of nodal metastases (Table 3).
CI=confidence interval; PSA=prostate-specific antigen.
Complications
No significant difference was observed concerning the incidence of Clavien-Dindo graded complications between men with and without lymph LND within 90 days of surgery (P=0.147, chi square). Over the study period, the percent of men who underwent LND and experienced a Clavien-Dindo grade I and II complication decreased whereas the percent of men with >grade II complications remained similar over time (Fig. 4). One patient experienced a grade IV complication after perforation of a sigmoid diverticulum 1 week after surgery. The complications more frequently observed in the lymphadenectomy group were symptomatic hematoma (2.1% vs 3.5%), symptomatic lymphocele (0% vs 1.5%), thromboembolic event (TEE) (0% vs 1.5%), anastomosis dehiscence (0.2% vs 1.1%), prolonged ileus (0.2% and 0.3%). The incidences of these complications were too low to analyze the effects during the study period.
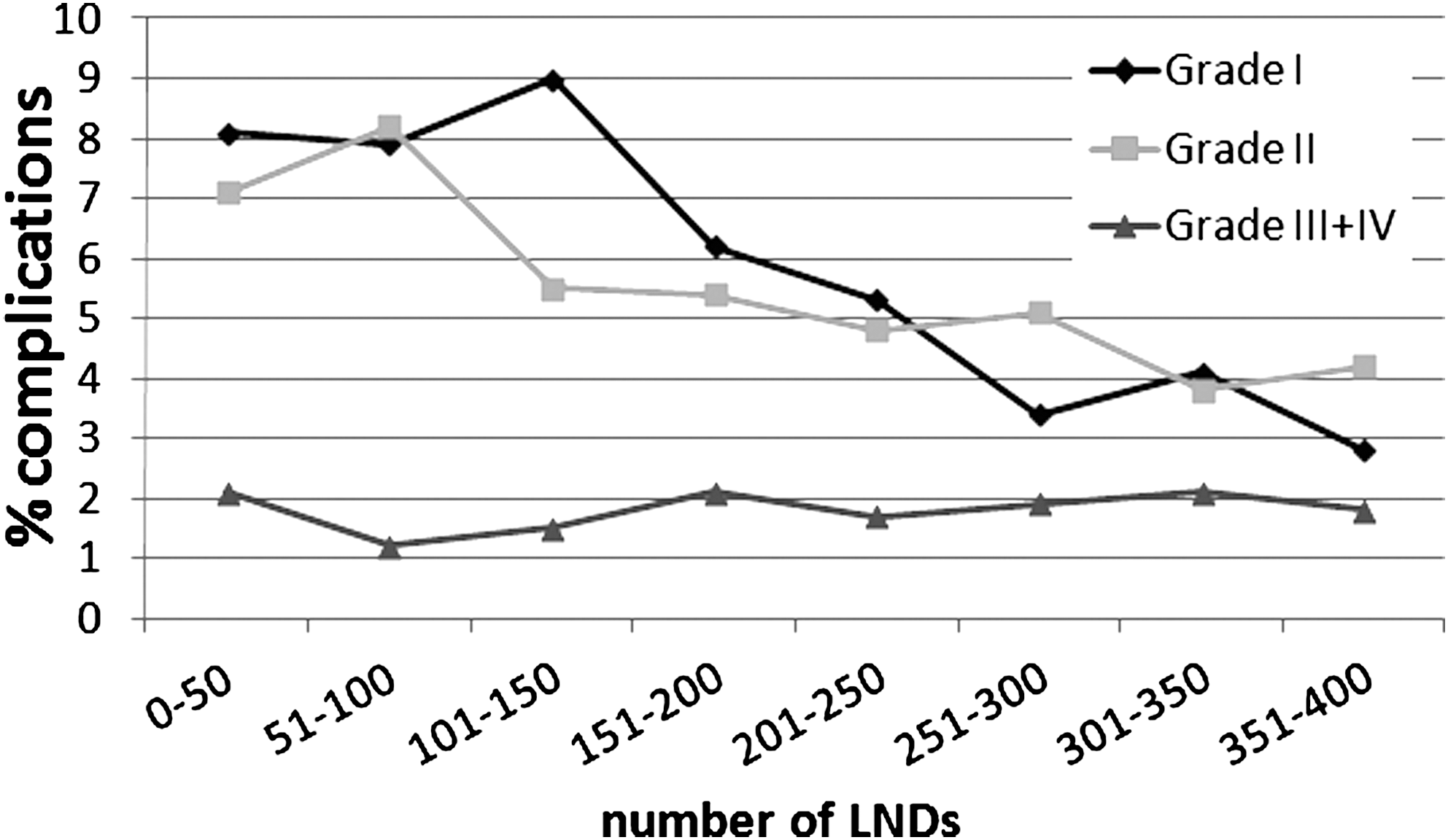
Complications by Clavien-Dindo grade classification and learning curve subgroup. LND=lymph node dissection.
Discussion
For prostatectomy, learning curve studies suggest improvement on various outcome measures during the initial 50 to 1500 cases (Table 1). Learning curve data for LND during robot-assisted prostatectomy has, to our knowledge, not been reported. Here we show that different outcome measures result in different improvement patterns for LND. Most importantly, we observed an increased number of removed nodes during the first 440 cases and a strong association between number of removed nodes and nodal positivity. Stabilization of the number of removed nodes was obtained after 250 cases with a median value of 14 removed nodes. Earlier studies found improved nodal staging and possible survival with more extended LND at prostatectomy. 10
The number of nodes recommended to be present in an extended LND is 20. 1,5,11,12 Despite an increase during the study period, we were not able to obtain this number of resected nodes. One may therefore argue that the learning curve has not yet been completed. Recent data from our institute, however, showed that in bladder cancer, the number of removed nodes from the same surgeon varied widely depending on the pathologic institute in which the samples were evaluated. 13 Because all prostatectomy procedures were performed in the hospital with the lower number of retrieved nodes during cystectomy and the fact that the median number of retrieved nodes during the cystectomy procedures reported earlier was not significantly different (15) from the number of nodes found after the initial cases for prostatectomy LND, we assume that our nodal sampling is adequate at the end after a plateau was reached for the number of removed nodes in our series and is comparable to that obtained during open radical cystectomy for bladder cancer at our institute. During the study period, neither the pathologist nor the method of node analysis changed, but because nodal yield was found highly dependent on pathology analysis, the absolute numbers of nodes reported here may not be comparable to those of other studies.
The importance of experience for LND performance was confirmed by our observation that besides clinical stage, the number of removed nodes was the only independent predictor of detecting nodal metastases, and the number of removed nodes significantly increased during the learning curve. For prostatectomy, surgical margin rate as well as biochemical outcome have earlier been linked to experience. 14 Our data show that at least for detection of nodal metastases, surgeon experience similarly plays a role.
The strong association between nodal yield and detection of nodal metastases in our study suggests that with an increase in experience, the surgeon is likely to remove more lymph nodes, which improves detection of metastases. Surgeons should be encouraged to focus on removing as many nodes as possible to shorten their learning curve for LND and have early improvement in nodal metastases detection. In line with this observation is the fact that during the initial 100 RALP cases, we tended to have a relative undersampling, considering the slightly lower percent of men with intermediate- and high-risk tumors who underwent LND in this group (Fig. 1).
Although a subjective evaluation, we thought that some technical alterations in the node dissection during the initial 100 cases improved the outcome. The main change in technique came from the anatomic approach where we initiated with identification of the internal iliac vessels and separation of the nodal area from the bladder. Subsequently, the more proximal (common iliac) nodes are identified and removed after identification of the ureter. In the final step, the obturator and external iliac nodes are resected. This approach allows for removal of the nodes in one entire package while identifying the essential anatomic landmarks.
Silberstein and associates 3 suggested that individual surgeon's skills and dedication may be more important for LND than surgical approach. Despite the minimally invasive nature of (robot-assisted) laparoscopic surgery, LND comes with a price. Earlier data suggested that increasing nodal yield over 10 significantly increased the risk of complications. 15 –19 In our series, low grade (Clavien I–II) complications decreased during the learning curve, but specific complications attributed to LND remained high during the learning curve. Moreover, the rate of higher grade complications (Clavien III–IV) remained stable during the first 400 LNDs.
Several complications were more frequently encountered in men who underwent RALP compared with RALP with LND. Clearly LND was associated with symptomatic lymphoceles in a 1.5% of men. The actual incidence of lymphoceles remains unknown, because imaging was only performed in case of symptoms. Management of lymphoceles was primarily performed by percutaneous drainage and antibiotic therapy when infection occurred (Clavien grade IIIa complication). Open drainage of infected lymphoceles because of multilocular lymphoceles was needed in two patients (Clavien grade IIIb complication).
TEEs occurred in 1.5% of cases and were only observed in men who underwent LND. Pulmonary embolisms were diagnosed in two men at 3 and 6 weeks after surgery. Antiembolic measures such as anticoagulants and stockings in the perioperative period were applied but were insufficient to prevent all TEE despite the fact that men were mobilized from day 1 after surgery. Our incidence of TEE is in line with earlier reports and clearly stresses the importance of antiembolic measures in men who undergo a (minimally invasive) prostatectomy in particular when LND is applied. The earlier mobilization and hospital discharge clearly did not prevent TEE in our population.
Interestingly, anastomotic dehiscence after surgery, defined as more than half a circumference of loose anastomotic stitches, was observed five times more often in men who underwent LND. Mobilization of the bladder for LND may be related to this complication. Moreover, dehiscence was secondary to a local hematoma (n=1) and a symptomatic lymphocele (n=1). In three cases, anastomotic dehiscence occurred without any other complication. In all instances of anastomotic dehiscence, conservative management with a longer interval of transurethral catheter use resolved the problem. Because LND was performed before the anastomosis, preoperative strain on the anastomosis is not likely to be the explanation of this higher incidence of anastomotic problems.
It remains speculation as to the causes of the reduction in grade I and II complication rates during the initial cases in our series. First, part of it may be explained by the shortened operative time during the learning curve. Second, we changed patient positioning from leg rests to French position after 800 cases. Antibiotic prophylaxis (cefazolin 1 g 15 minutes before surgery) for LND patients was initiated after 150 patients and may have contributed to the reduction in infection rate; however, the infection rate already decreased in the first 150 cases.
Limitations of our analysis are those inherent to the retrospective setup. First, in general, it can be stated that the current criteria for nodal dissection during prostatectomy are limited by the fact that nomograms may not be uniformly applied between patient populations. Although data were obtained prospectively and the indications for LND and case mix remained similar during the study interval, not all men underwent LND, and experience obtained during RALP may have impacted on the learning curve for LND. Second, the limited number of surgeons participating in this analysis and the overall number of robot procedures performed during the study interval may affect the learning curve, and surgeons with a higher or lower number of procedures may experience different learning curves. Third, the short follow-up (median <3 years) renders evaluation of oncologic outcome differences during the learning curve for LND not reliable. With respect to this, it can be of note that the percentage of men with normal PSA values after surgery (PSA<0.1 ng/mL) at the initial analysis after 3 months did not change during the learning curve. Fourth, during the study period, neither the pathologist nor the method of node analysis changed, but because nodal yield was found highly dependent on pathology analysis, the absolute numbers of nodes reported here may not be comparable to those of other studies.
Conclusions
Improvement patterns for LND during RALP were observed during the first 150 cases for operative time, 250 for nodal yield, 300 for node positivity rate, and 400 for complication rate (Clavien grade I and II complications). Although the overall complication rate was not different between men who underwent RALP with and without LND, specific complications such as TEE, symptomatic lymphoceles and hematomas, and anastomotic dehiscence were more frequent in men who underwent LND. Whether further improvement of results can be obtained remains to be determined, but the high variation of nodal yield among patients suggests that a more stable nodal yield is desirable. In light of this, it is important to conclude that the true “learning curve” still needs to be defined.
Footnotes
Disclosure Statement
No competing financial interests exist.