
Abstract
Purpose:
To evaluate the effect of hyaluronic acid (HA) and carboxymethylcellulose (CMC) instillation after transurethral resection of the prostate (TURP) on preventing urethral stricture.
Patients and Methods:
A total of 180 patients underwent TURP for benign prostatic hyperplasia. Recruited patients were randomly divided into two groups: Groups A and B. Patients in group A (90 patients, experimental group) received HA/CMC instillation, and patients in the group B (90 patients, control group) received lubricant instillation after TURP. Each patient was evaluated at 4 weeks (V1), 12 weeks (V2), and 24 weeks (V3) after the surgery. The effectiveness of HA/CMC instillation was evaluated based on the International Prostate Symptom Score/Quality of Life, peak urine flow rate, voided volume, and postvoid residual volume. The visual analogue scale (VAS) pain score and degree of satisfaction were also determined for each participant.
Results:
Among 180 initial participants, 80 patients in group A and 81 patients in group B had completed the experiment. VAS pain scores were 0.75±0.75 and 1.75±1.37 (P<0.001), and degrees of satisfaction were 0.63±0.66 and 0.91±0.51 in group A and group B at 1 month after surgery (P=0.002). By retrograde urethrography, urethral stricture after TURP was seen in 1 of 80 subjects in group A and 7 of 81 subjects in group B.
Conclusions:
HA/CMC instillation after TURP decreased the incidence of urethral stricture. In addition, HA/CMC was effective at reducing pain during the early postoperative period, with no adverse effects.
Introduction
Currently the most popular and effective treatment for patients with LUTS/BPH is transurethral resection of the prostate (TURP). 3,4 TURP, however, is associated with postoperative complications such as bleeding, a prolonged inpatient period, pain, and infection as well as late complications including urethral stricture, incontinence, erectile dysfunction, retrograde ejaculation, and bladder neck contraction. 5 Other methods have been studied to reduce occurrence of post-TURP urethral stricture by performing TURP with small diameter resectoscopes or with warm saline. 6,7
Recently, synthetic physical barriers have been developed to supplement cases in which the natural barrier has been damaged. Of these, representative substances are hyaluronic acid (HA) and carboxymethylcellulose (CMC).
HA is an anionic polysaccharide demonstrating high levels of polymerization, hydrophilicity, and nonimmunity as well as viscoelastic properties. As the active ingredient of the extracellular matrix, it coats the mucosal surface and provides lubricating action. From such actions of coating mucosal surface, the possibility of trauma reduction on the surgery site is being recommended. 8 CMC is also an anionic polysaccharide, which is an inducer of more hydrophilically modified cellulose with the glucosidic hydroxyl group having been carboxymethylationized, and has been used as an excipient, viscosifier, lubricans, and stabilizer for pharmaceutical products, cosmetics, and food. 9 HA and CMC (HA/CMC) has been used in surgical procedures for preventing postoperative adhesion. 10
No study, however, has examined the preventive effects of using HA/CMC for prevention of urethral stricture after TURP. To this end, this study aimed to identify the effectiveness of HA/CMC in preventing urethral stricture formation after TURP for treatment of spatients with LUTS/BPH.
Patients and Methods
Patients and study design
For this study, 180 patients with LUTS/BPH who underwent TURP from June 2010 to May 2011 were recruited. This was a randomized, single blinded, multicenter, prospective study undertaken by 10 surgeons at seven participating medical institutions. Each surgeon performed an equal number of TURP (experiment: 9, control: 9). The study was implemented after obtaining the approval of the Institutional Review Board.
Included subjects (1) underwent TURP after clinical diagnosis with BPH, and (2) were willing and able to participate. Excluded from the study were patients with diagnoses of (1) prostatic hypertrophy treated with endoscopic or invasive procedures of prostatectomy, (2) urethral stricture, which was diagnosed by cystoscopy, (3) neurogenic bladder, or (4) a urinary tract infection.
A simple block randomization method was used to assign patients to either (1) an experimental group (90 patients; group A), whose patients received HA/CMC instillation after TURP, or (2) a control group (90 patients; group B), whose patients received lubricant instillation after TURP.
The primary end point was the occurrence rates of urethral stricture; secondary end points of voiding symptoms, satisfaction, and degree of pain were evaluated.
Before enrollment (V0), information regarding illness duration and medical history was collected. Routine hematologic tests and urinalysis were performed. Patients were assessed during visits at postoperative week 4 (V1), week 12 (V2), and week 24 (V3).
Surgical technique
TURP was performed in the following sequence of directions: 6 o'clock, 3 o'clock, 12 o'clock, and 9 o'clock. We used a 26F resectoscopic sheath, 30-degree telescope, and bipolar resector. A three-way, 30-cc balloon, 22F urethral Foley catheter was inserted, and the catheter was pulled back to block the bladder neck. Thereafter, 5 mg of HA/CMC (Guardix-sol,® Hanmi Medicare, Seoul, Korea) or 5 mg of lubricant (chlorhexidine gel) was instilled using an 18-gauge catheter inserted between the urethral lumen and the Foley catheter (Fig. 1). Postinstillation traction was retained for 1 day before removal. While keeping the traction of the Foley catheter, the patients were kept on bed rest.

Instillation of HA/CMC on urethra using an 18-gauge catheter.
Assessment of efficacy and safety
Efficacy of HA/CMC was assessed to prevent urethral stricture at each postoperative visit by determining the International Prostate Symptom Score (IPSS) and by measuring the peak urine flow rate (Qmax), and the postvoid residual (PVR) urine volume. The quality of life (QoL) score was also determined. During the postoperative inpatient period, assessments were made of the indwelling time of the Foley catheter, degree of pain, and level of satisfaction. Constrictive uroflow curves or a maximum flow rate ≤10 mL/s by uroflowmetry was considered to indicate the occurrence of a urethral stricture.
To distinguish urethral stricture from bladder neck contracture, urethral stricture was confirmed by urethroscopy and urethrography. Assessment of pain and satisfaction level were conducted with the 0 to 10 point Likert scale visual analogue scale (VAS) pain score and a 0 point (very satisfied) to 3 point (very unsatisfied) Likert scale. The safety of HA/CMC treatment was assessed at V1, V2, and V3 by taking patient history, performing a physical examination, and recording adverse effects.
Statistical analysis
The occurrence of the urethral stricture rate was evaluated by per protocol analysis based on the number of patients who completed the study. Preoperative characteristics, including prostate volume, and perioperative outcomes were evaluated by intent-to-treat analysis. Voiding symptoms, Qmax, and PVR were compared by using the Student paired t test. The patients who had no occurrence of urethral stricture were compared with those who had occurrence in terms of voiding symptoms, pain scale, and degree of satisfaction. SPSS software v.18.0 was used for statistical analysis, and a P value<0.05 was considered to be statistically significant.
Results
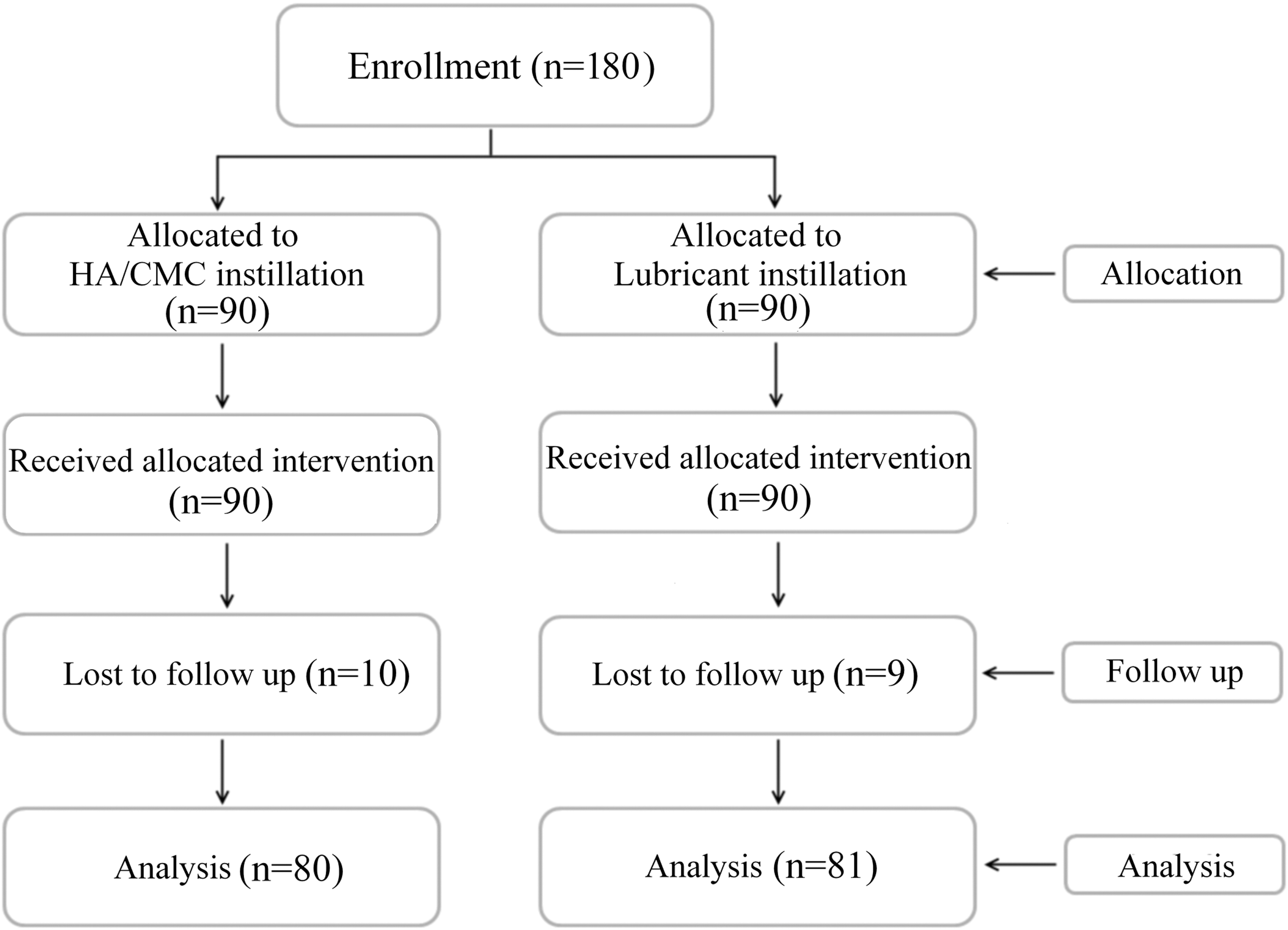
Of 180 total patients, 10 in group A and 9 in group B were lost to follow-up and were excluded. Analyses were performed using data collected from the records of 80 patients in group A and 81 patients in group B, who fulfilled the follow-up period (Fig. 2). There was no statistically significant difference in the baseline characteristics and perioperative outcomes between the patients lost to follow-up and those completing the study.
The 26-week study with a 2-week screening period and a 24-week treatment phase.
One patient in group A experienced intraoperative capsule perforation, and one patient in group B needed an intraoperative transfusion (P=0.316). Three patients in group A and two patients in group B experienced postoperative clot retention (P=0.642), while two patients in group A needed a postoperative transfusion (P=0.154). One patient in group B experienced the onset of epididymo-orchitis (P=0.322). Nine (11.25%) patients in group A and 19 (23.46%) in group B experienced a urethral stricture according to uroflowmetry (P=0.041). According to retrograde urethrography, one patient in group A and seven patients in group B had a confirmed urethral stricture (P=0.031) (Table 1). The stricture site occurred in the bulbous urethra in one patient in group A, and in the bulbous urethra in three patients, the pendulous urethra in one patient, and the fossa navicularis in three patients in group B.
Preoperative characteristics were well balanced between the groups. Resected prostate volumes, indwelling days of the Foley catheter, and length of stay had no significant difference between both groups (Table 2).
Student t test
Group A: HA/CMC instillation, Group B: lubricant instillation.
BMI=body mass index; PSA=prostate-specific antigen; TRUS=transrectal Ultrasonography; IPSS=International Prostate Symptom Score, QoL=quality of life; Qmax=peak urine flow rate; PVR=postvoid residual volume.
At each visit after surgery, the patients showed no significant difference of voiding symptoms between groups. At postoperative week 4 (V1), the satisfaction levels were 0.63±0.66 for group A and 0.91±0.51 for group B (P=0.002), while VAS pain scales were 0.75±0.75 for group A and 1.75±1.37 for group B (P<0.001) (Fig. 3).

Surgical outcomes of the experimental group and the control group after transurethral resection of the prostate at each follow-up time point. IPSS=International Prostate Symptom Score; Qmax=peak urine flow rate; VAS=visual analogue scale.
Discussion
This study aimed to assess the effects of HA/CMC instillation into the urethra after TURP at the onset of urethral stricture. We found that HA/CMC was effective for prevention of urethral stricture with no specific side effects. In addition, it improved the postsurgical outcomes by helping to reduce pain during the early postoperative period, thereby increasing patient satisfaction levels.
BPH occurs by histologic proliferation of smooth muscle and epithelial cells in the prostatic transitional zone. 11 The objective in LUTS/BPH treatment is to improve the QoL and to treat and prevent complications including urinary tract obstruction, urinary retention, and infection. Therapeutic methods are largely divided into watchful waiting, medical management, and surgical management. 12 Of these, watchful waiting is applicable to patients with mild symptoms or with moderate-to-severe symptoms but no complications. This treatment necessitates annual measurement of prostate volume as well as assessment of flow rate. 13
For medical management, representative drugs are alpha-adrenergic blockers and 5 alpha-reductase inhibitors (5ARI). 5ARI lowers serum dihydrotestosterone and reduces prostate volume to relieve symptoms. 14 Alpha-adrenergic blockers do not affect prostate volume or prostate-specific antigen values but improve symptoms through the relaxation of smooth muscle cells in the prostate. 15 When patients show moderate-to-severe symptoms accompanied by complications such as infection, hematuria, or upper urinary tract obstruction, or when they do not improve with medical management, however, indications suggest surgical management. Moreover, surgical management is increasingly being offered for control of lower urinary tract symptoms. 16
Surgical management technique includes open prostatectomy, transurethral vaporization, TURP, transurethral holmium laser ablation/enucleation, holmium laser resection, photoselective vaporization, and transurethral incision, but TURP is still the gold standard for surgical treatment of LUTS/BPH. 13 In TURP, the prostate is resected using radiofrequency energy. Despite advancements in surgical techniques and instruments, TURP faces many challenges such as morbidity, a long inpatient time, and long indwelling time of the Foley catheter in addition to infection, bleeding, incontinence, reterograde ejaculation, and urethral stricture. 17
Urethral stricture after TURP is a considerable complication with an incidence rate of 1.2% to 29%. 5,18,19 Large variation in the prevalence of urethral stricture is seen because of the absence of clear descriptive criteria for urethral stricture. According to Desmond and associates, 20 peak urine flow reduced to ≤10 mL/s is the diagnosis for urethral stricture. In present study, urethral stricture was defined as constrictive uroflow curves or a maximum flow rate ≤10 mL/s by uroflowmetry and when the stricture site was observable by urethroscopy or urethrography. Occurrence rate of urethral stricture was 8.64% in present study; this relatively high number of occurrences may related to the fact that we used only a 26F resectoscopic sheath, which is a relatively larger size, even though there was no resistance of resectoscope passage. The location of the urethral stricture site, however, was not analyzed statistically in the present study because of the small number of patients affected. Moreover, no randomized studies have been performed to analyze the association between the urethral stricture site and the size of the resectoscope.
Urethral stricture often occurs after TURP, and the triggering factors reported include infection, mechanical injury, and indwelling of the Foley catheter. 21 During TURP, the instrument moves into the urethra a mean of 800 times, causing mechanical injury. In addition, indwelling of the Foley catheter causes ischemia of the urethra, or the catheter itself might cause mechanical injury. 22 During tissue development, remodeling, and wound healing of the mechanical injury site, urethral stricture is caused by scar formation and fibrosis. In these cases, extracellular matrix regulation plays a prominent role in this process, which sodium hyaluronate may inhibit to reduce unwanted scar tissue by 50% or more. 23 In addition, animal studies by Hong and colleagues, 10 reported that fewer fibrous tissues were observed by histologic test on a group postoperatively coated with HA/CMC.
Several natural barriers including the peritoneum, omentum, and amnion prevent adhesion between tissues. 24 When this barrier is damaged after surgery, however, synthetic physical barriers are needed to separate the injured tissue surface from the surrounding organs. 25 These include film barriers, solution barriers, and recently developed sol-gel transition barriers. 26 Among these, solution barriers and sol-gel transition barriers can be used for post-TURP instillation between the urethra, bladder neck, and Foley catheter. HA/CMC is a liquid type synthetic physical sol-gel barrier with viscosity from 2500 to 3500 cP. 10 In this study, HA/CMC was used to reduce the incurrence of post-TURP urethral stricture based on the results of previous studies about the usefulness and scar formation inhibition properties of HA/CMC as a solution synthetic physical barrier for internal urethrotomy. 27
No differences were seen in the test group treated with HA/CMC and the control group for IPSS, QoL, or uroflowmetry among patients in whom no urethral stricture had occurred. Thus, HA/CMC did not appear to affect postoperative voiding symptoms. Significant differences were seen, however, in the postoperative pain scale and occurrence rate of urethral stricture. HA/CMC is a solution synthetic physical barrier with high viscosity that is expected to be effective, because it maintains a long contact time when coated onto a tissue surface. HA/CMC instillation during TURP might reduce the postoperative occurrence of urethral stricture because of its efficacy to prevent fibrosis and scar formation during the healing of the stricture resected site and mechanical injury inside the urethra. Moreover, reducing the pain of the experimental group may come from longer sustaining of lubrication between the prostatectomy site, urethra injury site, and Foley catheter than the control group.
Limitations of this study were the relatively short follow-up and absence of an animal study. We did not perform a power calculation. Moreover, the use of a relatively large resectoscopic sheath may limit the generalizability of the findings reported in the present study. This is the first prospective, randomized controlled study to identify the usefulness of HA/CMC for reducing the incidence of post-TURP urethral stricture formation, however. Whether the efficacy of HA/CMC can be maintained persistently through long-term follow-up observations must be determined, and identification of the histologic actions of the post-TURP use of HA/CMC necessitates animal studies.
Conclusion
The results of our study indicate that use of HA/CMC in the urethra during TURP decreases the incidence of urethral stricture. It showed effectiveness in reducing postoperative pain with no side effects and improved patient satisfaction.
Footnotes
Acknowledgments
This study was sponsored by Hanmi Medicare, Seoul, Korea.
Disclosure Statement
No competing financial interests exist.