
Abstract
Background and Purpose:
Because of the limited working space available during retroperitoneal laparoscopic radical nephrectomy (LRN), the body habitus of the patient is likely to affect the risk of operative difficulties. This study sought to determine whether anthropometric measurements based on CT and abdominal radiography could be used to predict operative difficulties during retroperitoneal LRN.
Patients and Methods:
Between August 2004 and January 2012, 96 consecutive patients with preoperative CT and abdominal radiography examinations underwent retroperitoneal LRN for a T1 or T2 stage renal tumor at our institution. The association between anthropometric measurements and demographics of patients and operative duration, estimated blood loss (EBL), and perioperative complications were retrospectively analyzed. Multivariate analysis was performed, and P<0.05 was considered significant.
Results:
Anterior perirenal fat distance (P=0.016) and distance from the 12th rib to the iliac crest (P=0.038) were independently associated with operative duration. Only anterior perirenal fat distance (P=0.001) was independently associated with EBL. No intraoperative complications and reoperations occurred. The occurrence or severity of postoperative complications was not significantly associated with anthropometric measurements. Body mass index ≥25.0 kg/m2 was not significantly associated with operative difficulties.
Conclusion:
The anterior perirenal fat distance and the distance from the 12th rib to the iliac crest can be used to predict operative difficulties during retroperitoneal LRN.
Introduction
Several studies have recently demonstrated a relationship between operative difficulties and patients' body mass index (BMI) in LRN, 4 –6 while other studies have not found this relationship. 7,8 Therefore, we suggest that some factors other than BMI may affect the operative difficulty of LRN. Anderson and associates 9 demonstrated that increased perirenal fat, as opposed to abdominal fat, increases the operative duration of hand-assisted laparoscopic donor nephrectomy. 9 Because of the small working space of the retroperitoneal approach, the body habitus of the patient, which includes factors such as body fat and skeletal structure around the kidneys, is likely to affect operative difficulty. No studies, however, have specifically assessed the surgical difficulties of the retroperitoneal approach associated with the body habitus of patients.
The aim of the present study was to investigate whether patients' body habitus affects the operative difficulty of the retroperitoneal LRN. Therefore, the associations between body habitus and adverse outcomes of surgery, including bleeding, operative duration, and perioperative complications, were evaluated.
Patients and Methods
Patient selection
Ninety-six patients underwent retroperitoneal LRN for clinical stage T1 and selected T2 RCC at our institution between August 2004 and January 2012. Preoperative CT and abdominal radiography were performed on all patients. The transperitoneal approach was not used; only the retroperitoneal approach was used in RCC patients with clinical stage T1 and selected clinical stage T2 who were undergoing endoscopic surgery during the period of this study. Among the RCC patients with clinical stage T2, open radical nephrectomy was sometimes performed in cases of tumor size exceeding 10 cm, as well as projected tumor lateral from the kidney. In RCC with clinical stage T2, however, the final decision concerning whether to perform laparoscopic or open surgery was left to the attending physicians and patients. One patient, whose surgery was converted to open surgery because of severe adhesion between the tumor and the peritoneum, was excluded from the analysis. The Institutional Review Board for research involving human subjects approved this retrospective analysis.
Operative technique
With minor modifications, retroperitoneal LRNs were performed as previously described. 1,10 The patient was positioned in the flank position while the surgeon and endoscopist stood at the patient's dorsal and contralateral sides, respectively. Retroperitoneal LRN was performed using four ports. The first trocar was placed near the tip of the 12th rib by open laparoscopy. A 12-mm blunt-tip port was placed in a retroperitoneal space created by balloon dilation. The second 12-mm port was placed at the junction of the 12th rib and the erector spinae muscle. The third 12-mm port was placed at the midaxillary line. For purposes of retracting the kidney and/or peritoneum, the fourth port was inserted between the blunt-tip port and the third port.
An insufflation pressure of 8 mm Hg was used. Hem-o-lok XL or L size clips were used to ligate the renal artery, vein, and ureter. The kidney was dissected outside of the Gerota fascia. Retroperitoneal LRN was performed by or under the supervision of two surgeons (TY and NH), board-certified in urologic laparoscopy by the Japanese Endoscopic Surgical Qualification System.
Parameters assessed
CT scans and abdominal radiography films were reviewed by a blind reviewer (AH) to assess the radiographic anatomic parameters 9,11,12 outlined in Table 1 and represented graphically in Figure 1 A, B, C. With the exception of sagittal abdominal diameter (SAD), anatomic parameters on the CT scans were measured at the midpoint of the main renal vein entering the hilum. Several clinicopathologic factors including age, sex, height, weight, side of disease, number of renal arteries, tumor size, and history of upper abdominal operation were verified through patient records. BMI, the ratio of weight in kilograms divided by the square of height in meters, was calculated for each patient. In this series, patients with a BMI equal to or in excess of 25.0 kg/m2 were defined as obese. 13
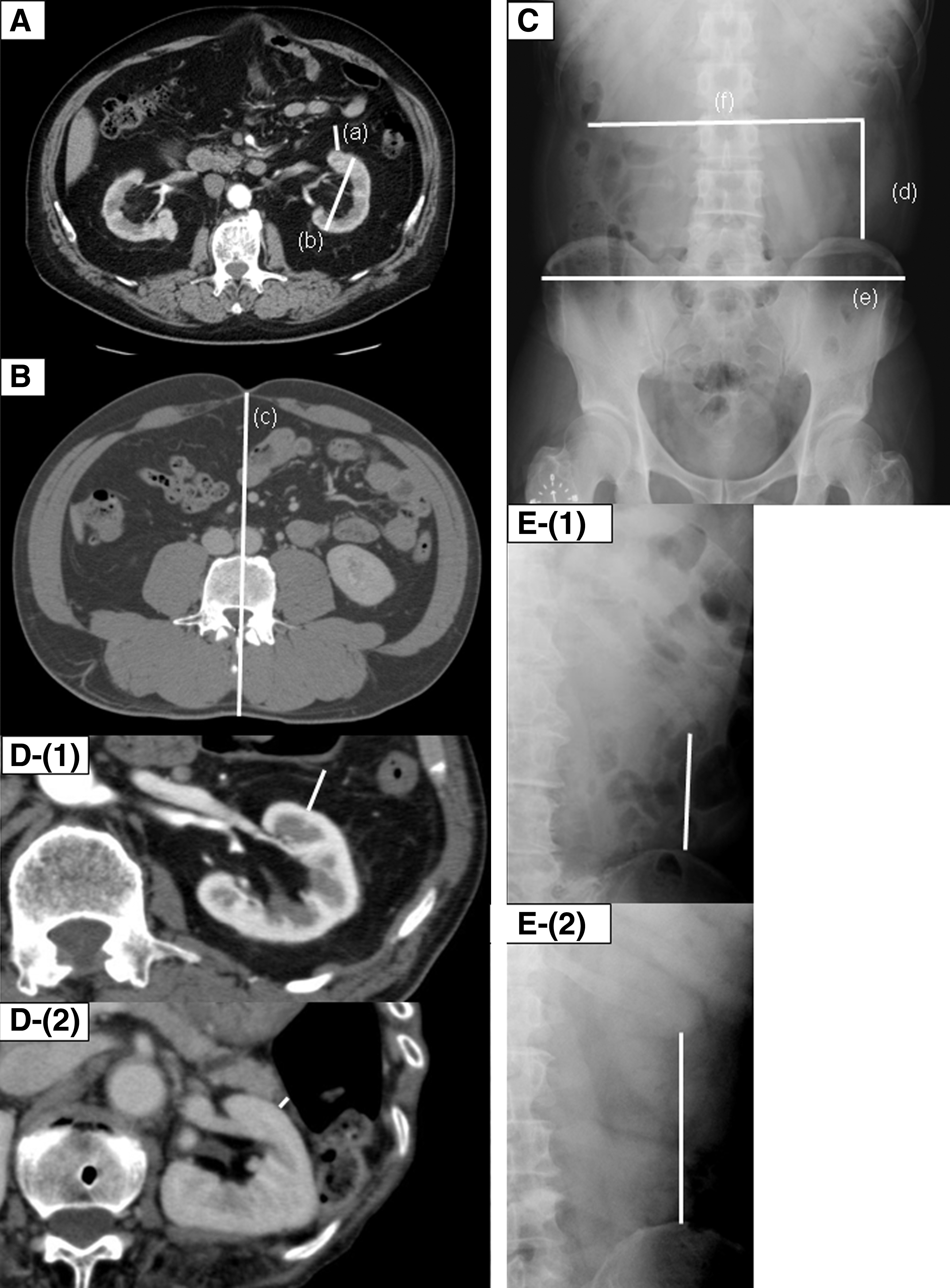
Radiographic anatomic parameters on computerized tomography scans and abdominal radiographic films.
Evaluation of operative difficulty
Operative duration, estimated blood loss (EBL), and perioperative complications were recorded as surrogate markers of operative difficulty. Perioperative complications were graded according to the Clavien classification system. 14
Statistical analysis
All values are presented as means±standard deviation. A two-sided Mann-Whitney U test was used to determine significant differences in binary variables. The correlations between continuous variables were investigated by simple regression analysis using the Spearman rank correlation coefficient. Multivariate analyses were performed using multiple linear regression to identify the risk factors associated with operative difficulties. P values <0.05 were considered significant. Analyses were performed with Stat View version 5.0 software (Abacus Concepts, Berkeley, CA).
Results
A total of 95 patients were enrolled in this study, including 63 (66.3%) men and 32 (33.7%) women. The mean patient age was 64.7±10.4 years (range 35–84 years), while the average BMI was 23.6 kg/m2 (range 14.8–35.1 kg/m2). According to preoperative imaging, the mean tumor size was 35.5±18.4 mm (range 13.0–130.0 mm). The tumor was on the left side in 50 (52.6%) patients and on the right side in 45 (47.4%) patients. The mean operative duration for all patients was 273±59 minutes (range 163–450 min). The mean EBL was 83±127 mL (range 2–685 mL). Body dimensions measured by CT scans and abdominal radiographyare shown in Table 2b.
The 12th rib–iliac crest=distance from the 12th rib to the iliac crest. The 12th rib–the 12th rib=distance from the 12th rib to the 12th rib.
P<0.05
N=number of patients; SD=standard deviation; BMI=body mass index; EBL=estimated blood loss; C.C=correlation coefficient.
Obesity, SAD, anterior perirenal fat distance, anteroposterior renal diameter, and distance from the 12th rib to the iliac crest were all significantly associated with operative duration on univariate analyses (Table 2). On multivariate analyses, anterior perirenal fat distance and distance from the 12th rib to the iliac crest were independently associated with operative duration (Fig. 1-D-E, Table 3). BMI ≥25 kg/m2 and anterior perirenal fat distance were significantly associated with EBL during retroperitoneal LRN on univariate analyses (Table 2). Anterior perirenal fat distance was the only independent predictor of EBL on multivariate analysis (Figure 1D-E, Table 3).
Denotes statistical significance at P<0.05 level.
EBL=estimated blood loss; β=standard partial regression coefficient; the 12th rib–iliac crest=distance from the 12th rib to the iliac crest; BMI=body mass index.
No intraoperative complications occurred and no reoperations or intra- or postoperative blood transfusions were needed. The 10 postoperative complications that were noted included wound infection (grade I) in three patients, atrial fibrillation (grade IIa) in two patients, and paralytic ileus (grade I) in two patients, as well as pulmonary atelectasis (grade I), bleeding from the postoperative wound (grade IIa), and acute epididymitis (grade I) in one patient each. The presence and severity of these complications were not associated with patient characteristics and anthropometric measurements (data not shown).
Discussion
Although the experience of the surgeon may be a more decisive factor affecting surgical outcome, one cannot completely exclude the impact of a patient's physique on the technical difficulty of performing LRN. Indeed, several reports have demonstrated an association between anthropometric measurements and adverse events associated with pelvic surgery. 15 –17 Few studies, however, have assessed the relationship between patients' body habitus and adverse surgical events of retroperitoneal LRN for renal masses.
In the present study, patients with a BMI equal to or in excess of 25.0 kg/m2 were defined as obese, as per the recommendation for Asians by the Western Pacific Regional Office of the World Health Organization. 13 Using this criterion, no significant differences in operative duration and EBL were observed between BMI ≥25 kg/m2 and BMI <25 kg/m2 on multivariate analysis. Prentice and colleagues 18 showed, however, that BMI did not reflect regional body fat distribution. Indeed, for certain body types, such as those with increased muscle mass, BMI is a poor predictor of percent body fat. 19 SAD was introduced as a means of estimating visceral obesity. 20 SAD, however, was not significantly associated with operative duration and EBL on multivariate analysis. Therefore, BMI and SAD appear to be poorly associated with the surgical difficulties of retroperitoneal LRN.
This study demonstrated that anterior perirenal fat distance was independently associated with operative time and EBL. This finding is in accord with a previous study of hand-assisted laparoscopic donor nephrectomy. 9 Retroperitoneal LRN has much less working space than transabdominal LRN, 1 which limits the approach significantly. Theoretically, a large amount of perirenal fat could further exacerbate the limited working space, obscure anatomic landmarks, and make the identification of renal vessels and their tributaries more difficult. 9 In addition, a large amount of anterior perirenal fat could impede visualization of the organs on the anterior aspect of the kidney. Hence, careful surgical dissection may be needed to avoid injury to the organs anterior to the kidney, such as the peritoneum, vena cava, or duodenum. As a result, the operative duration may increase because of a large amount of anterior perirenal fat.
Thus, the surgeon's vantage point could determine the degree of operative difficulty in the retroperitoneal approach, which may be sensitive to the perirenal fat and space limitations for direct visualization. In addition, the area of surgical dissection is determined by the amount of perirenal fat. In particular, dissection of anterior perirenal fat is likely to cause bleeding because of the presence of perforating vessels between anterior perirenal fat and the peritoneum. Hence, it is plausible that, as the amount of anterior perirenal fat increases, so does the extent of bleeding. On the other hand, because the dissection was performed outside of the perirenal fat, the size of the kidney did not affect the operative duration and EBL in the present study.
Hagiwara and coworkers 4 demonstrated that while tumor size was not associated with a prolonged operative time in transperitoneal LRN, it was a significant risk factor for prolonged operative time during open radical nephrectomy. This finding is in accordance with the results of the present study. The candidates considered for retroperitoneal LRN in the present study, however, included only persons with T1 and T2 RCC. If larger tumors had been operated on laparoscopically in this study, tumor size may have affected the operative duration.
Bony pelvic dimension has been found to be associated with the occurrence of operative difficulties during pelvic surgery. Some studies have shown that narrower pelvic width increases the operative difficulties in rectal cancer or prostate cancer. 15,17 Similarly, in the present study, whether abdominal girth or skeletal structure around the kidney may affect operative difficulty was examined. It was found that the distance from the 12th rib to the iliac crest was significantly correlated with operative time. This finding is somewhat counterintuitive because, as the distance from the 12th rib to the ilium increases, working space would be expected to increase as well. Thus, it is likely that this relationship is spurious.
During retroperitoneal LRN, positioning of the trocars tends to be restricted between the ribs and iliac crest. When the circumference of the kidney, specifically the upper pole of the kidney, is dissected outside the Gerota fascia, the tip of the forceps is deeply inserted into the retroperitoneal cavity. The increase in distance from the 12th rib to the iliac crest may increase the distance from the tip of the forceps to the body surface. Accordingly, the distance from the handle of the forceps to the body surface decreases, potentially leading to contact between the handle and abdominal wall. As a consequence, awkward hand positioning may result in increased operative time. In such circumstances, longer instruments may be useful.
Preoperatively determining issues that may arise during a procedure is useful for the surgeon. Complex patients with an abundance of anterior perirenal fat and a long distance between the 12th rib and iliac crest should be treated by other than the retroperitoneal approach to minimize perioperative complications. In particular, in cases with an abundance of anterior perirenal fat, whereas the retroperitoneal approach is restricted to direct visualization, the transperitoneal approach may improve direct visualization. In such cases, the transperitoneal approach or conversion to the transperitoneal hand-assist approach may be recommended, because that procedure provides better visualization and/or tactile sensation.
Several limitations of the present study must be considered. First, the current study was retrospective in nature and included a small sample size. It may have been underpowered to find the associations between patient characteristics and operative difficulties. In particular, because of a lack of intraoperative complications and subsequent reoperations, the association between body habitus and these outcomes could not be assessed. In addition, it may be plausible that the lack of significance of some variables, such as “anteroposterior renal diameter” or SAD, was due to the small sample size.
Next, patients with a BMI equal to or in excess of 25.0 kg/m2 were considered obese. A BMI scale that differs from the standards of Americans and some other parts of the world, where obesity is defined as BMI equal to or in excess of 30.0 kg/m2, was used. The prevalence of persons with a BMI ≥30.0 kg/m2 is only 3% in Japan and more than 30% in the United States. 21 In the present study, the rate of BMI ≥30.0 kg/m2 was only 4.1 % (four patients), in accordance with the above-mentioned report. Therefore, whether these conclusions are applicable to patients with a BMI defined by a stringent cutoff is still not known and, thus, should be clarified in the future.
Then, clear criteria for laparoscopic or open radical nephrectomy in clinical stage T2 RCC were not used. Hence, the choice of whether to perform laparoscopic or open radical nephrectomy depended on the preference of attending physicians and patients. A possible selection bias regarding the different surgical methods may have occurred. Next, the potential for intraobserver error during radiologic measurement should not be overlooked. Last, in this series, operative duration ranged between almost 3 hours and 8 hours, longer than in contemporary series. It seems unlikely, however, to have affected the results of the association between operative difficulty and anthropometric measurements.
Conclusion
The findings of the present study suggest the anterior perirenal fat distance is significantly associated with operative duration and EBL during retroperitoneal LRN. Conversely, obesity, as defined by the BMI, is not significantly associated with operative difficulties. In addition, the distance from the 12th rib to the iliac crest is significantly associated with operative time. The ability to predict the risk of operative difficulty by measuring the anterior perirenal fat distance and the distance from the 12th rib to the iliac crest may aid in minimizing perioperative complications.
Footnotes
Disclosure Statement
No competing financial interests exist.