
Abstract
Pelvic organ prolapse is a common problem faced by many women, resulting in significant morbidity and negatively impacting quality of life. Sacrocolpopexy can treat women with vaginal vault prolapse, multicompartment prolapse, and/or a history of failed prolapse procedures. The transabdominal sacrocolpopexy has been shown, on multiple studies, to have one of the highest long-term success rates for repair of severe vault prolapse. The goals of surgical repair of vaginal vault prolapse include restoration of proper anatomy, maintenance of sexual function, and durability. Recently, there has been a push toward decreasing morbidity and recovery time associated with operative repair. Therefore, the robot-assisted sacrocolpopexy was developed and has gained widespread acceptance, given the excellent reproducible results, minimal complications, and high patient satisfaction. Our technique for robot-assisted sacrocolpopexy is presented.
Methods
Indications/contraindications
Relative contraindications for robot-assisted sacrocolpopexy would be similar to most laparoscopic procedures and would depend on the surgeon's experience and the complexity of the case. These typically include multiple previous abdominal or pelvic procedures, severe chronic obstructive pulmonary disease, and morbid obesity. In addition, the surgeon should consider each relative contraindication in light of the patient's age and comorbid disease conditions.
Preoperative workup
The initial workup for any patient considering surgery for treatment of pelvic organ prolapse should include a careful history and physical examination. Key points to be addressed during the history include any symptoms experienced, degree of bother, and concurrent urinary symptoms, particularly related to incontinence. A thorough past medical and surgical history is imperative. Physical examination should focus on the abdomen and genitalia. A complete pelvic examination is essential to identify the compartments involved and the degree of prolapse. In addition, attempts to elicit stress incontinence should be performed both at baseline and with the prolapse reduced. This should be performed with the patient in the lying and standing positions. No imaging studies are needed preoperatively. A urinalysis is important to exclude infection in any patient being considered for a concurrent midurethral sling.
Preoperative preparation
No specific preoperative preparations are needed before robot-assisted sacrocolpopexy. We do not routinely administer a preoperative bowel preparation to our patients.
Instrumentation
Nondisposable
• Veress needle
• 12-mm robotic port
• 12-mm laparoscopic port
• Two 8-mm robotic ports
• 5-mm laparoscopic port
• 30 degree robotic camera
• Two robotic needle drivers
• Robotic scissors
• Robotic grasping forceps
• Laparoscopic scissors
• Laparoscopic grasping forceps
• Handheld vaginal retractor
Disposable
• Laparoscopic suction
Surgical Steps
Patient preparation and positioning
The patient is placed in the dorsal lithotomy position. Either a nasogastric or orogastric tube is placed, and both arms are tucked at the patient's side. A face-shield plate may be used to protect the endotracheal tube and the patient's face from potential trauma from the robotic scope, which is larger than a standard laparoscopic scope. The patient is prepped from the nipples to proximal thigh, including the vagina.
Placement of instruments
Pneumoperitoneum is obtained after gaining access to the peritoneal cavity using a Veress needle at the umbilicus. After obtaining pneumoperitoneum, ports are placed beginning with placement of a 12-mm periumbilical port. This may be placed under direct vision to avoid visceral or vascular injury. The remaining ports, as shown in Figure 1, are placed as follows: One 12-mm port right subcostal lateral to the rectus muscle, one 5-mm port one handbreadth inferior-laterally, and two 8-mm robotic ports placed lateral to the rectus muscle two fingerbreadths superior to the iliac crest. It is important to make sure that there is enough space between the robotic ports so that the robotic arms will not collide. One method for this is to verify that ports are spaced a handbreadth or 8 to 9 cm apart. The patient is placed into a steep Trendelenburg position, and the robot is docked with the base positioned at the foot of the bed (Fig. 2).
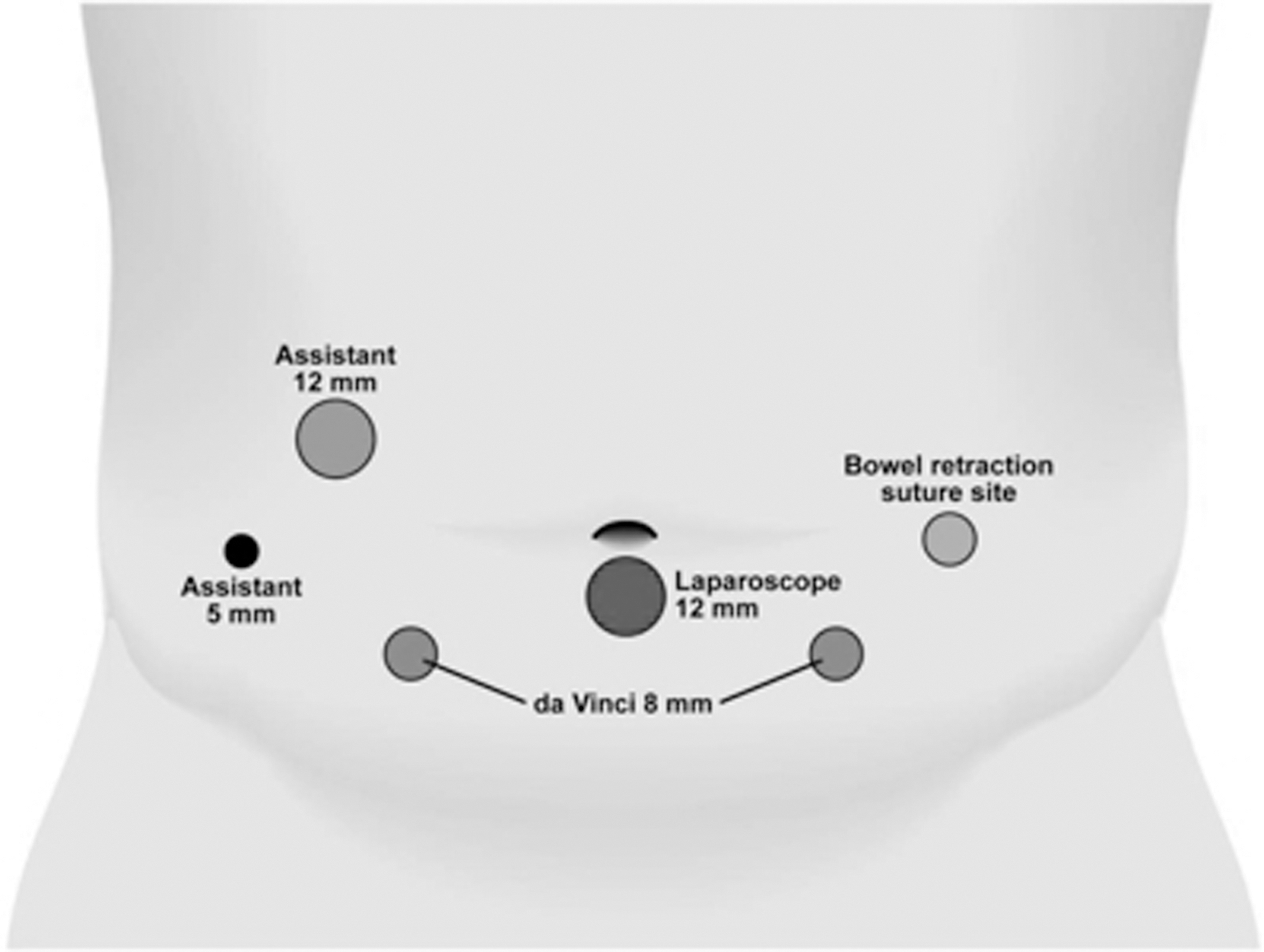
Example of port configuration for robotic sacrocolpopexy. The bowel retraction suture (far right circle) is also a potential site for a third robotic arm.

With the patient in steep Trendelenburg position the robot is docked with the base positioned at the foot of the bed.
Gaining exposure
The abdomen and pelvis are first inspected. Any problematic adhesions are taken down robotically. The sigmoid colon is identified and accessed. We prefer to retract the sigmoid to gain better access to the sacrum. Therefore, a Keith needle is used to pass a retracting suture into the abdomen through the skin. Using the robotic arms, a retracting suture is placed through the sigmoid tenia to help expose the sacral promontory. This suture is then passed back through the skin next to the entry site. This is gently secured at the skin level with a clamp. The sigmoid colon is reflected cephalad and to the left followed by incision of the posterior peritoneum exposing the sacral promontory. Alternatively, the third arm can be used to provide traction.
The next step is dissection of the bladder from the anterior vaginal wall using forceps and scissors with cautery. A customized handheld vaginal retractor manufactured at the Mayo Clinic

A customized vaginal retractor.
Both of these dissections should be performed as distal (toward the introitus) as possible to maximize the support provided by the Y-graft. It is important to have the assistant place the vaginal retractor in toward the head of the patient and angled slightly inferiorly to better visualize the plane between the bladder and vagina. This will help facilitate precise dissection to avoid vaginal or bladder entry.
After adequate vaginal mobilization, attention is turned to the sacral promontory where the dissection should expose the periosteum. The peritoneal reflection overlying the sacral promontory is gently scored with cautery to begin the dissection, which is then carried through the underlying tissues to visualize the sacral promontory. Care must be taken to avoid injury to the presacral veins, which can cause significant bleeding and impair visualization.
Mesh placement
Next, three or four 2.0 Gore-Tex sutures, cut to approximately 7 cm, are placed horizontally into the sacrum above the level of S2. The sutures are placed deep enough into the sacral promontory to withstand moderate traction with the robotic grasper. These sutures with needles attached are left in the abdomen in preparation for mesh fixation. Outside the patient's body, the polypropylene Y-graft (Fig. 4) is trimmed to the appropriate size, which is estimated visually based on the distance between the vagina and the sacral promontory. The anterior flap of the Y mesh graft is temporarily sutured back to the tail of the graft. This maneuver helps keep the graft from obscuring the surgeon's view and allows easier suturing of the posterior flap to the posterior vaginal canal.

A macroporous Y-mesh graft is used to restore apical support.
The graft is then placed into the abdomen through the assistant port. The graft is sutured with interrupted full thickness sutures at the vagina using 2.0 Gore-Tex suture with the 30-degree lens and vaginal retractor to maximize exposure for placement of the sutures. The posterior arm of the Y-graft is attached first, because this tends to be more difficult. Four to six sutures are used on the posterior flap of the Y mesh graft to obtain best support of the apex and posterior vagina. The holding suture in the graft is then cut to allow the anterior flap to be manipulated to the anterior vagina. It is then secured in a similar fashion. The long arm of the Y mesh graft is then secured with the previously placed sutures within the sacral periosteum, with careful attention to avoid any undue tension on the vagina. This is best accomplished with the assistant using the vaginal retractor to place the vagina at the appropriate distance to the sacral promontory without excessive stretch and then the surgeon at the console securing the graft to keep this approximate position. Finally, the posterior peritoneum is closed over the mesh graft with a running absorbable suture to retroperitonealize the graft.
Placement of a suprapubic sling
It is our preference to place a prophylactic midurethral sling in all patients undergoing robot-assisted sacrocolpopexy. After complete evacuation of gas from the abdomen, we proceed with suprapubic sling placement in the usual fashion.
Management of anatomic variants
Frequently, the most challenging part of this procedure is dissection of the plane between the bladder and vagina. Therefore, this is often attempted as the first part of the procedure such that we are able to determine whether completing the procedure robotically will be possible. We have found that careful manipulation of the handheld vaginal retractor by the assistant can greatly aid in this dissection. In addition, for patients with a redundant and/or floppy sigmoid colon, the retracting suture is essential for exposing the sacrum.
Another critical step, dissection of the sacral promontory, can be fraught with difficulty if care is not taken to identify and avoid the presacral veins, which can be the cause of significant bleeding. If bleeding does occur, this can often be controlled with electrocautery. If significant bleeding ensues, then placement of clips by the assistant is often necessary.
Postoperative management
The nasogastric tube is removed at the end of the procedure. Patients are started on a clear liquid diet immediately postoperatively, which is advanced as tolerated. Pain control is accomplished with as needed intravenous (IV) ketorolac, IV narcotics, oral narcotics, and acetaminophen. A Foley catheter is typically left overnight and removed early the next morning. Patients are typically dismissed on postoperative day 1 after tolerating a general diet, ambulating, and voiding spontaneously.
Management of intraoperative complications
A potential intraoperatively identified complication would be entry into the bladder or vagina during dissection to create a plane between them. In our experience, this can be managed by meticulous closure in two layers to ensure a watertight closure. If successful closure is achieved, then we will proceed with the procedure. We leave a Foley catheter for 1 week postoperatively in this situation, however. Another potential complication encountered may be bleeding from the presacral veins. This is often controlled successfully with a combination of electrocautery and Hem-o-lok clips applied by the bedside assistant. If bleeding persists, then open conversion may be needed.
Management of postoperative complications
Mesh erosion is a rare complication of this procedure (Table 1). When this occurs, often it can be managed with transvaginal excision of the mesh. Other complications include urinary tract or wound infection, which can be managed with oral antibiotics. Although rare, port site hernias may occur and often necessitate open reduction and repair. Lastly, as with any transperitoneal surgery, small bowel obstruction may occur and can be managed conservatively with bowel rest and nasogastric decompression.
SBO=small bowel obstruction.
Robot-assisted sacrocolpopexy is an effective and durable treatment alternative to abdominal sacrocolpopexy. Robot-assisted sacrocolpopexy offers certain advantages over the traditional abdominal sacrocolpopexy, including less blood loss and shorter hospital stay, 1 while maintaining equivalent results for prolapse repair. 2 Many surgical case series have reported excellent short 3 and long-term results 1,4 primarily based on anatomic improvements in vaginal vault prolapse. Overall failure and complication rates of the procedure remain low, with excellent overall patient satisfaction. 1,2,5 –8
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviation Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.