
Abstract
Robot-assisted laparoscopic radical cystectomy (RARC) was initially described in 2003 and has since been gaining popularity as a minimally invasive technique in both men and women of all ages with muscle-invasive bladder cancer, selected cases of high-risk nonmuscle invasive disease, and selected cases with advanced disease.1,2 RARC offers the patient the benefits of less blood loss, shorter hospital stay, less postoperative pain, and early recuperation with improved cosmesis. For a surgeon, it facilitates fine dissection and intracorporeal suturing in a visually conducive three-dimensional environment with ergonomic comfort. For residents, fellows, and novice surgeons, RARC can shorten the learning curve in comparison with pure laparoscopic procedures. In selected cases, nerve-sparing, vaginal-sparing, uterus-sparing, and prostate-sparing RARC can be undertaken to maintain functional outcomes and fertility. We aim to succinctly describe the indications and contraindications, preoperative workup, preoperative preparation, instrumentation needed, surgical steps, postoperative care, and management of intraoperative and postoperative complications. New advances in technique and a summary of the major published series for RARC are also reported.
Methods
Indications and contraindications
Preoperative work-up
A thorough history and physical examination are critical. All medical comorbidities should be optimized before surgery. A basic laboratory workup should include serum chemistries, liver function tests, and complete blood cell counts. Imaging should include chest radiography and axial imaging of the abdomen and pelvis. A bone scan should be considered in any patient with new onset bone pain or elevation of the alkaline phosphatase level in the serum. Endoscopic assessment includes evaluation of the size and location of the tumor, bimanual examination under anesthesia, and evaluation of the urethra for orthotopic neobladder and assessment for simultaneous urethrectomy. The pathology slides must be reviewed at the center where cystectomy is being used.
Patient preoperative preparation
Patients who travel from a distance prefer being admitted the day before surgery for preanesthesia checkup, to meet with the enterostomal therapist for marking and teaching, clean intermittent catheterization teaching for patients undergoing continent urinary diversion, mechanical bowel preparation, and a clear liquid diet. Some patients do not undergo a mechanical bowel preparation and come for surgery the same day.
Instrumentation
For nondisposable, disposable, and optional instrumentation, see Table 1.
Surgical Steps
Preparations and port placement
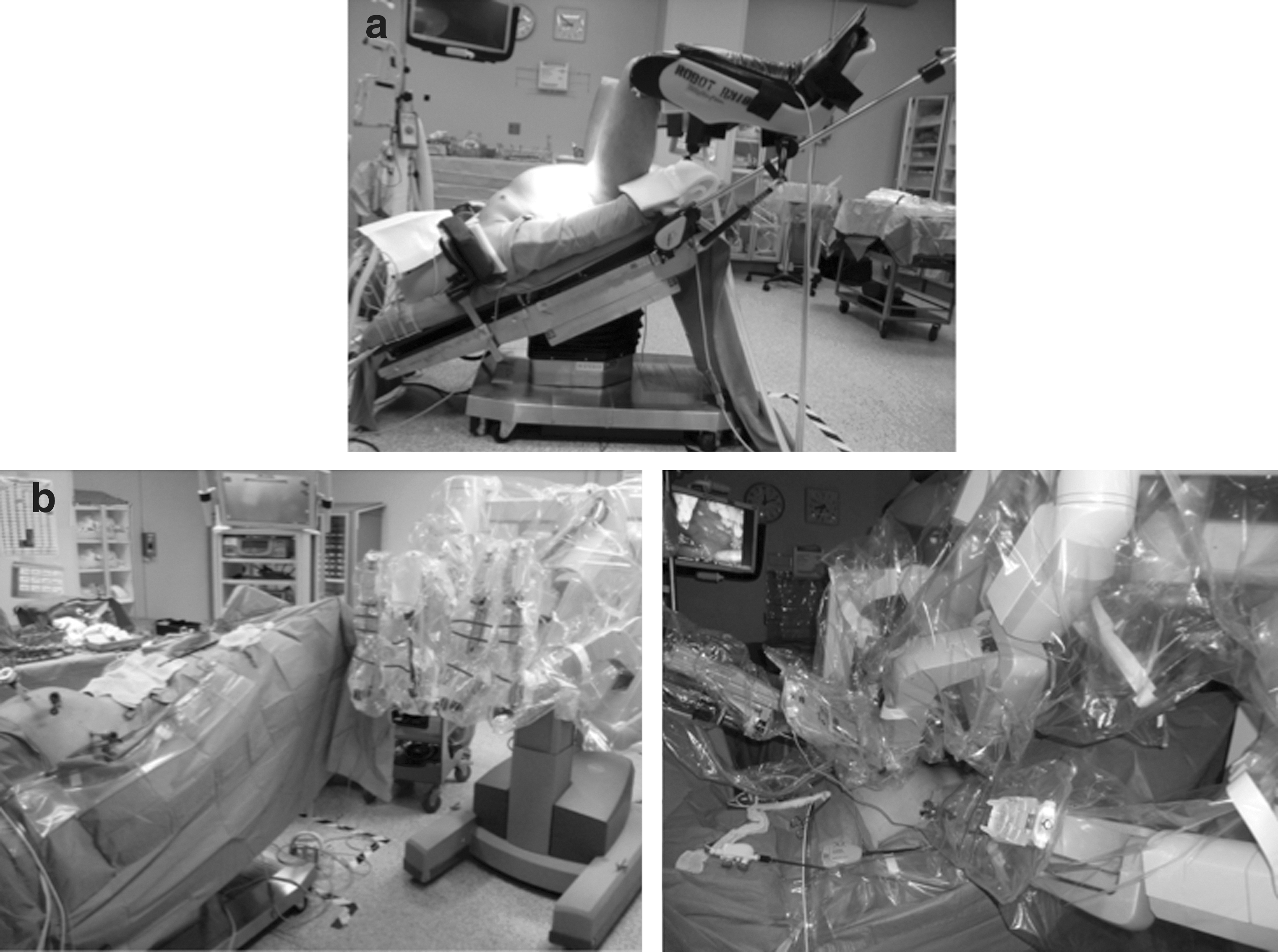
The patient is positioned in the dorsal lithotomy position with the arms tucked ensuring adequate padding of all extremities to avoid potential compartment syndrome and/or neuropraxia. 3 The patient is adequately secured to the table and placed in a steep Trendelenburg (20–45 degrees) (Fig. 1a). Alternatively, the patient can be left supine, and the robot can be side-docked to avoid a prolonged lithotomy position (Fig. 1b). After induction of general anesthesia, the patient is prepped and draped in the usual sterile fashion. A gastric tube is inserted, and a Foley catheter is placed on the sterile field.
Using a Veress needle, the abdomen is insufflated to 15 mm Hg. An ENDOPATH® XCEL™ 12-mm bladeless bariatric trocar is inserted 2 inches above the umbilicus. The camera is then inserted, and the abdomen and pelvis are inspected for injuries to structures from insertion of the Veress, adhesions, and metastatic disease. Under endoscopic guidance, the remaining three 8-mm robotic ports and the two assistant ports are placed.
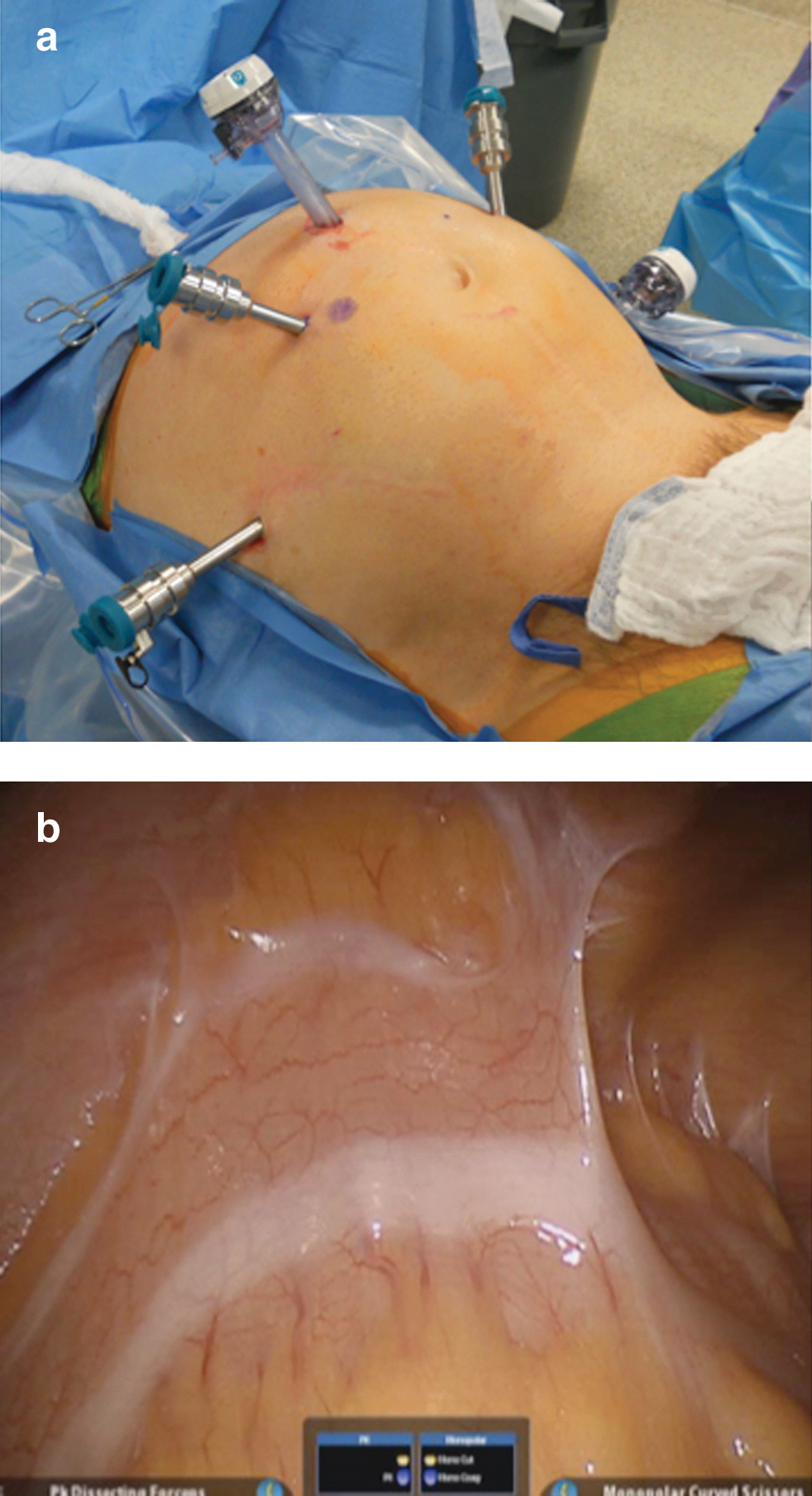
Two robotic ports are placed on each side of the camera port approximately 7 to 10 cm lateral and about 2 cm below the umbilicus. The third robotic port is placed in the left lower quadrant of the abdomen approximately 7 to 10 cm lateral to the left-sided robotic port and 5 to 7 cm superior to the iliac crest (Fig. 2a). In cases where we perform robotic intracorporeal urinary diversion, however, the third robotic port is placed on the right side. An ENDOPATH XCEL 15-mm bladeless trocar is then inserted on the left side for the assistant, because this provides a better angle for working with the bowel. A second assistant port can be placed through the premarked stomal site when an ileal conduit is contemplated. The robot is then docked.
We typically use three instruments: Hot Shears™ in the right robotic arm, PK® dissecting forceps in the left robotic arm, and ProGrasp™ forceps in the third robotic arm. The technique we describe can be performed entirely with these three instruments to help cut down on operative costs. The 0-degree camera lens can be used for a majority of the dissection, but the 30-degree down lens may be helpful for dissecting deep within the pelvis and for the expended pelvic lymph node (LN) dissection. The 30-degree up lens may at times be helpful for dissecting behind the prostate, retroapical dissection, and for dropping the bladder.
Adhesiolysis
A large proportion of patients with BC who are being considered for ARRC are likely to need adhesiolysis 4 (Fig. 2b). Major complications can be avoided by following a few important principles. First, insufflation and initial port placement should be well away from previous abdominal scars to avoid potential underlying bowel or adhesions. Once initial access is attained, the remaining ports can be safely placed under direct vision away from other adhesions. If needed, the initial adhesiolysis can be performed laparoscopically using limited thermal energy. In our experience, as soon as the robotic camera port and one to two robotic ports are placed, we feel more facile to use adhesiolysis robotically with the added ergonomic comfort afforded by the robot. Alternatively, access can be obtained using an open Hassan technique for camera port placement with subsequent laparoscopic placement of the other ports.
LN dissection
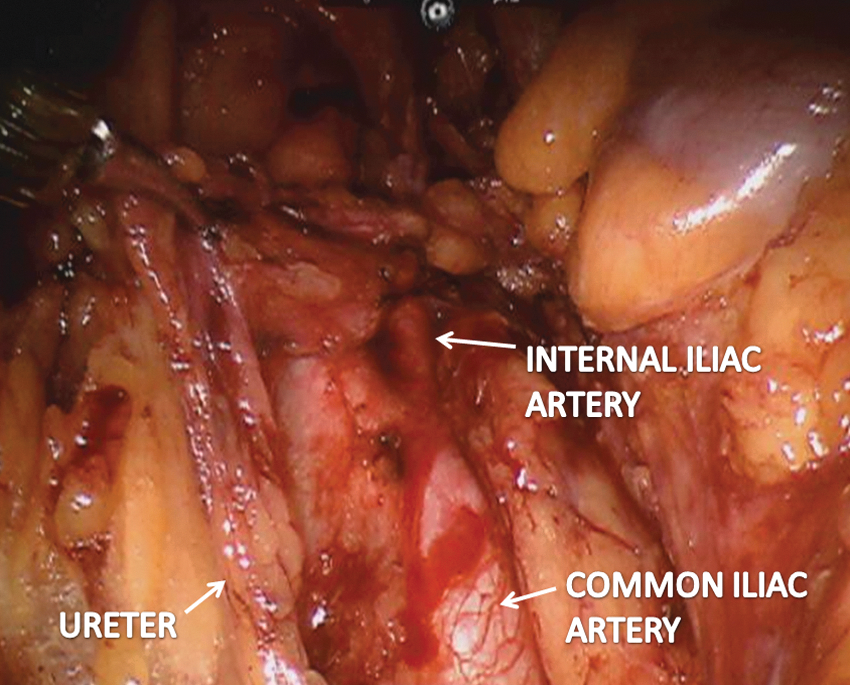
The LN dissection can be performed before cystectomy or once the cystectomy is completed. An incision is made in the posterior peritoneum, and the ureter is identified as it crosses anterior to the bifurcation of the common iliac artery. The ureter is dissected proximally and distally to the level of the bladder making sure to maintain the periureteral fatty tissue intact to avoid devascularization (Fig. 3). The ureter is clipped using a large tagged Hem-o-lok® clip and divided at the level of the bladder with a distal margin sent for frozen section analysis. This step has three advantages. First, by sending the distal ureter for frozen section analysis, it allows one to rule out cancer in the distal ureter. Second, clipping the ureter early allows for passive dilation of the ureter that can aid in the ureterointestinal anastomosis. Third, having the ureter out of the way allows for free handling and manipulation of the bladder angle for easier performance of the nerve-sparing dissection. Alternatively, the ureters can be left intact until the end with the advantage being continuous drainage of urine.
Lymph node dissection.
The fibrofatty and lymphatic tissue is then dissected as proximal as the aortic bifurcation or at least 2 cm above the bifurcation of the common iliac artery, distally down the hypogastric artery and external iliac artery, to the distal most LN of Cloquet. We prefer clipping lymphatics or dividing after fulguration with bipolar energy for lymphostasis. The obturator nerve and vessels are identified posterior to the external iliac vein with full exposure of the intrapelvic course of the obturator nerve (Marcille triangle). Care should be taken to not injure the hypogastric nerves during the LN dissection, because these nerves course along the dorsolateral sigmoid/rectal wall. Lateral to the external iliac artery, the genitofemoral nerve and pelvic side wall are encountered, which is the lateral limit of the LN dissection.
ARRC in men
Posterior dissection
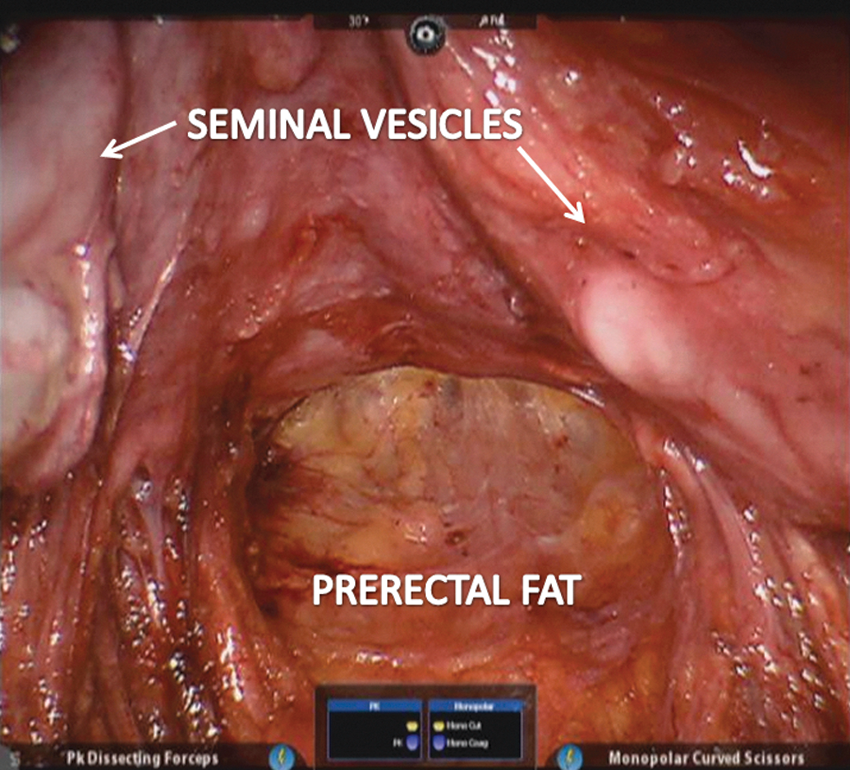
An incision is made in the posterior peritoneum just above its reflection over the rectum to develop the retrovesical space. The incision is carried laterally to connect with the previous incisions in the peritoneum made for the dissection of the ureters. The goal is to mobilize the base of the bladder and prostate off of the anterior surface of the rectum (Fig. 4). The seminal vesicles (SVs) and vasa deferentia (VD) are identified, dissected, and small vessels can be clipped or fulgurated. If performing a nerve-sparing procedure, minimal cautery should be used while dissecting the tip of the SVs. With the SVs held superiorly by the third robotic arm, an incision is made in Denonvillier fascia to establish a plane above the prerectal fat. This dissection is carried as far distally as possible to the apex of the prostate. Furthermore, a 30-degree upward lens is helpful during this dissection.
Posterior dissection.
Perivesical dissection
A critical step is developing the perivesical space between the bladder and lateral pelvic side wall. An incision is made lateral to the medial umbilical ligaments, and using blunt dissection and cautery, this is carried distally to the Cooper ligament (Fig. 5). The bladder should not be dropped at this point, because suspension to the anterior abdominal wall assists in controlling the pedicles.
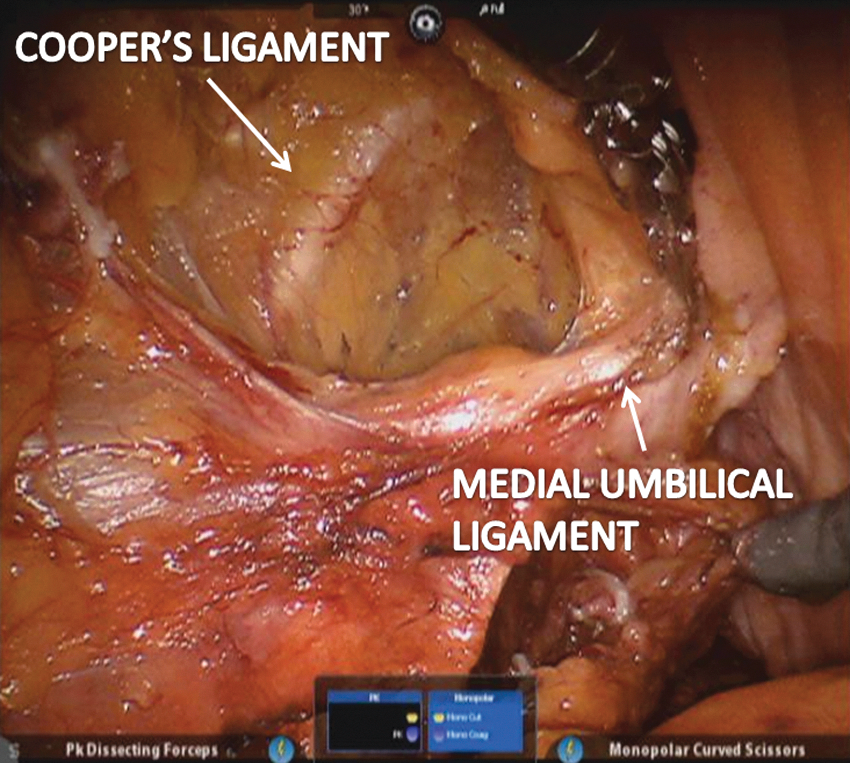
Perivesical dissection.
Division of bladder pedicles
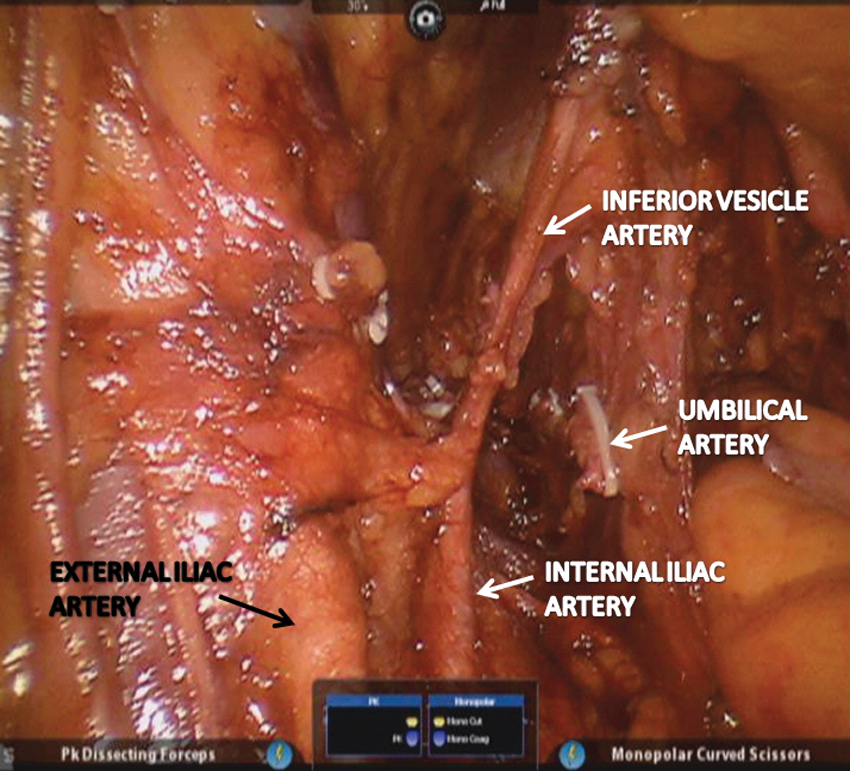
The bladder pedicles can be easily identified at this point (Fig. 6). The anterior division of the internal iliac artery is traced distally, and the umbilical artery and inferior vesical artery are ligated between several Hem-o-lok clips and divided. Other small vessels can be controlled using the PK® dissecting forceps. All of the pedicles can be ligated using Hem-o-lok clips as an additional cost-saving measure. Alternatively, the anterior and/or posterior pedicles can be ligated and divided using numerous other techniques or a combination of these techniques: • Suture ligation • Hem-o-lok clips • LigaSure Atlas™
• Enseal® Tissue Sealing • EndoWrist® Vessel Sealer • Harmonic ACE® Curved Shears 8 mm • Stapling • EndoWrist® Stapler • Echelon Flex™ Powered ENDOPATH® Stapler • Endo GIA™ Ultra Universal Stapler
Division of bladder pedicles.
Dropping the bladder
The bladder can be dropped by making an incision lateral to the left and right medial umbilical ligaments and joining them in the midline to divide the median umbilical ligament (urachus) just below the umbilicus and entering into the avascular space of Retzius (Fig. 7). An incision is made in the endopelvic fascia from the base of the prostate to the puboprostatic ligaments. The levator muscle fibers covered with fascia are gently swept away from the lateral aspect of the prostate.
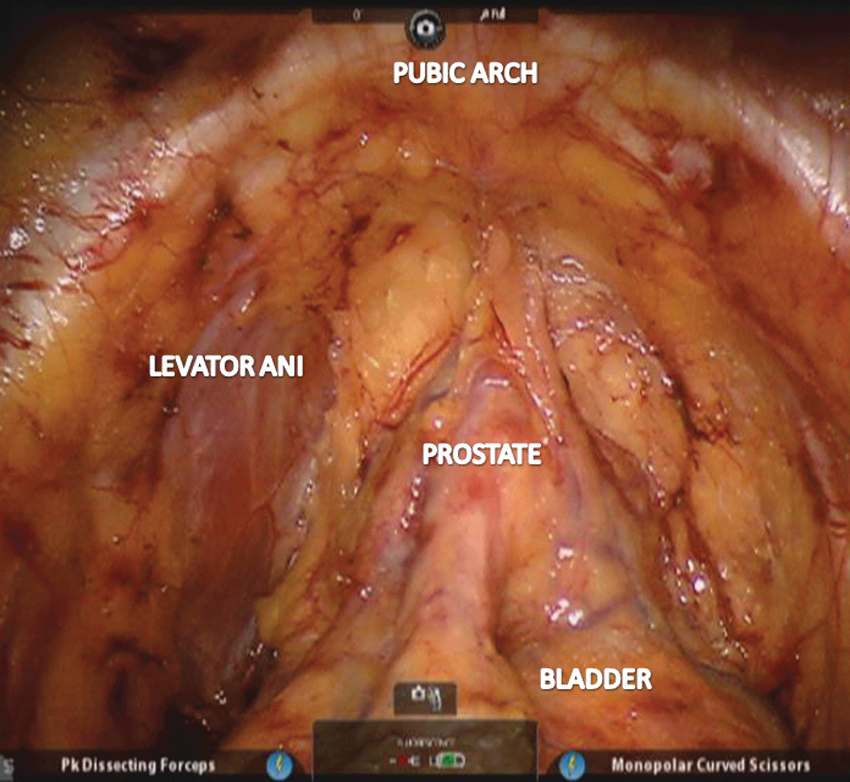
Dropping the bladder off the anterior bladder wall.
Nerve-sparing dissection
A nerve-sparing dissection can be performed in a similar fashion as for robot-assisted radical prostatectomy. 5 Furthermore, the hypogastric nerves should be avoided during the LN dissection, because injury to these nerves can have a negative impact on erectile function. An incision is made in the periprostatic fascia and carried distally to the apex of the prostate. The periprostatic fascia is swept laterally, taking care to avoid thermal injury or undue traction on the neurovascular bundles (Fig. 8). The prostate is retracted laterally exposing the contralateral prostatic pedicle, which is divided between several Hem-o-lok clips. Alternatively, absorbable Lapro-clips™ can be used with excellent results, especially if considering orthotopic neobladder, to prevent complications related to erosion of nonabsorbable clips. This technique effectively preserves the lateral periprostatic fascia. We prefer to perform an intrafascial dissection, because these are not cases of prostate cancer, although prostate cancer is quite common in these patients; we have noted incidental prostate cancer in 42% of our patients. 6
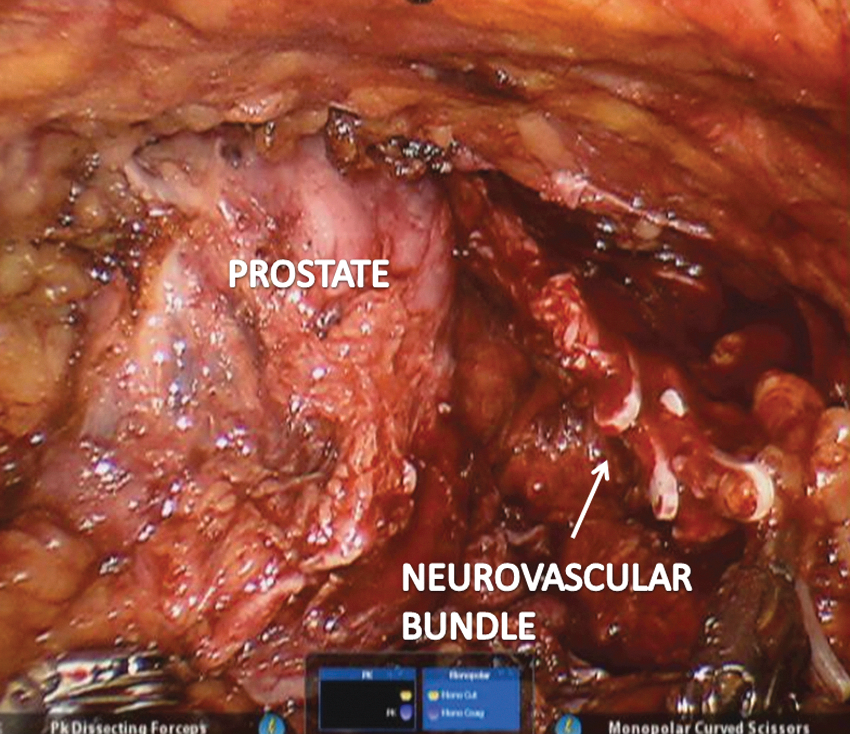
Nerve-sparing dissection.
Dorsal vascular complex (DVC) (Figs. 9a and 9b)
Anteriorly, the DVC is ligated using a 0-polyglactin on CT-1 needle. Needle drivers are not needed, because the PK dissecting forceps and ProGrasp forceps can be used to throw this stitch and save on the costs of the robotic needle drivers. Alternatively, the DVC can be divided using bipolar energy, a vessel-sealing device, or Echelon ENDOPATH 45-mm stapler.
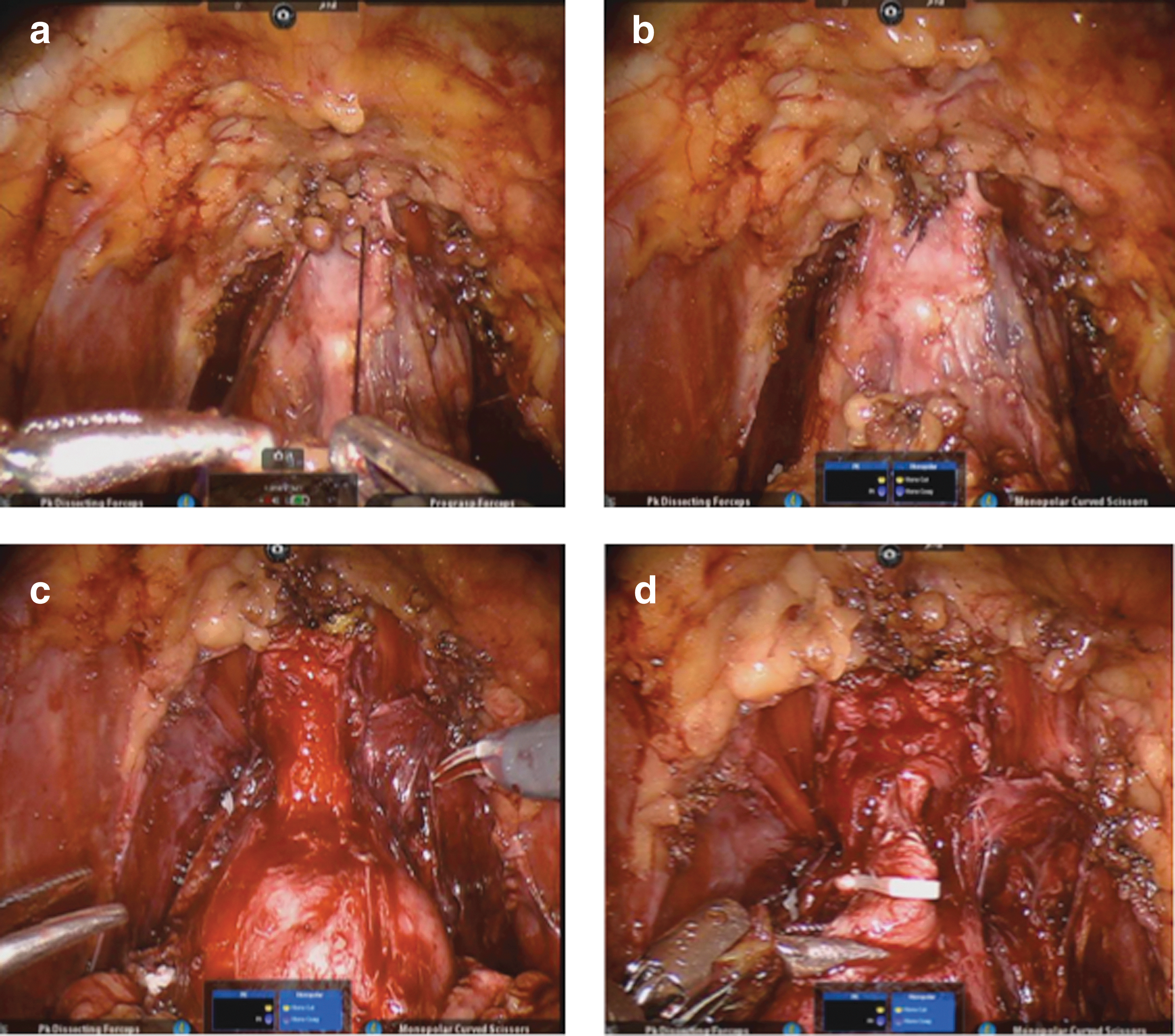
Apical dissection (Figs. 9c and 9d)
The apex of the urethra is divided, making sure enough length and sphincteric complex are maintained if orthotopic neobladder is being contemplated. The Foley catheter is then withdrawn, and a large 15-mm Hem-o-lok clip is placed on the urethra just distal to the apex of the prostate to avoid urine and/or tumor spillage. Alternatively, one can place a 15-mm Hem-o-lok clip over the Foley catheter with the balloon inflated, which aids in traction and counter traction. This is helpful for a bulky bladder mass and when the bladder and prostate are not completely freed. The specimen once freed is placed within an ENDO CATCH™ II 15-mm specimen pouch. The pelvis is irrigated and hemostasis is ensured (Fig. 10). A closed suction drain is placed through the lateral robotic port into the pelvis. Extending one of the port site incisions approximately 4 cm will allow retrieval of the specimen.

Depicting bilateral preservation of neurovascular bundles.
ARRC in women
Mobilization of ovaries, fallopian tubes, and uterus
If the ovaries, fallopian tubes, and uterus are in situ, robot-assisted laparoscopic anterior pelvic exenteration can be performed with some subtle modifications. The infundibulopelvic ligaments containing the ovarian vessels are divided using Hem-o-lok clips, bipolar energy, or a stapling device. The cardinal and uterosacral ligaments are divided allowing mobilization of the ovaries away from the pelvic side wall. The uterus can then be held superiorly by the third robotic arm.
Posterior dissection
An incision is made in the posterior peritoneum, thus opening the pouch of Douglas just beneath the junction of the uterus and posterior vaginal wall.
Vaginal dissection
A sponge-stick is placed per vagina, assisting in visualization of the vaginal apex. A horizontal incision is then made until the sponge-stick is visible within the vagina. The incision in the anterior vaginal wall is carried distally through the vesicocervical fascial fibers, the lateral pubovesical ligament, and the medial pubovesical ligament using the Echelon Flex™ Powered ENDOPATH stapler. This dissection is carried distally to the level of the bladder neck. Thus a strip of anterior vaginal wall is removed en bloc with the cystectomy specimen. The lateral sulcus of the vagina and the lateral wall of the urethra are important landmarks for preservation of the neurovascular bundles. If the surgeon is able to establish a plane between these two structures, one can preserve the vaginal arteries, clitoral nerve, perineal nerve, and inferior hemorrhoidal nerve. In all our female patients, we retrieve the specimen from the vagina.
Vaginal closure
A meticulous closure and reconstruction of the vagina is imperative to prevent postoperative leakage per vagina and pelvic organ prolapse. We recommend a multilayered vaginal closure with unidirectional barbed suture: 1-0 or 2-0 12″ V-Loc. 7 In addition, the reconstructed vagina should be suspended to the uterosacral ligaments. Paravaginal fixation can also be performed to the arcus tendinus and paravaginal structures.
Salvage ARRC
Some patients with BC opt for bladder-sparing protocols to maintain their native bladder in situ. Furthermore, men with previous treatment for prostate cancer may present with invasive BC or recalcitrant bladder neck contracture that may necessitate surgical extirpation. ARRC has been shown to be feasible in these challenging patients. Radiation has the potential to create fibrosis and difficult tissue planes, but the excellent visibility afforded by the robotic platform allows for precise intraoperative dissection.
Palliative ARRC
When a patient presents with either locally advanced or metastatic BC, cure is often not feasible. Many of these patients, however, have terrible local symptoms, including hematuria, lower urinary tract symptoms, pain, and upper/lower urinary tract obstruction. ARRC is feasible in these patients for palliation of local symptoms and improved renal drainage.
Prostate sparing cystectomy
This technique is largely considered experimental for the management of BC. For super selected patients with concern for potency and fertility, prostate-sparing cystectomy is feasible. The VD are identified, isolated, and preserved. The VD are dissected to the anterior surface of the SVs. The anterior prostate is incised 3 to 5 mm distal to the prostatovesical junction. The incision is carried down through the posterior prostate, and the entire specimen is freed. The bladder opening should be closed immediately using a clip or stitch to prevent tumor or urine spillage.
Vaginal- and/or uterus-sparing ARRC
In selected patients, this technique may be appropriate to optimize sexual outcomes and/or fertility. With a sponge-stick per vagina, the apex of the vagina can be easily visualized during the posterior bladder dissection. A plane is established between the anterior vaginal wall and the posterior bladder wall. This plane is carried distally to the level of the bladder neck. The specimen will have to be retrieved through one of the port sites, because the vagina is never opened.
Postoperative care
All patients follow our institutional ARRC postoperative pathway. The gastric tube is typically removed at extubation, unless there is an indication to leave it in, such as prolonged operative time, adhesiolysis, or suspicion of bowel injury. Aggressive pulmonary toileting is encouraged with the assistance of incentive spirometry. Patients are kept nothing per os until postoperative day (POD) 2, at which point a clear liquid diet is started if the patient does not have abdominal distention. The diet is then advanced as tolerated. A bisacodyl 10-mg suppository is given twice per day starting on POD 2 to stimulate bowel function. Colace 100 mg by mouth twice per day and once daily glycerin or Fleet® enema is started on POD 3. Patients are encouraged to ambulate beginning on POD 1. In addition, bilateral sequential compression devices are used as deep venous thrombosis (DVT) prophylaxis. Furthermore, subcutaneous enoxaparin or heparin is administered beginning on POD 1 for additional DVT prophylaxis, depending on the patient's comorbidity and/or ability to ambulate.
Perioperative systemic antibiotics are discontinued after 24 hours postoperatively. Pain control is with narcotics via patient-controlled analgesia pump and transitioned to oral narcotics on POD 2-3 when a liquid diet is started. Intravenous ketorolac is also a useful adjunctive agent to administer to help reduce narcotic need and is given for the first 48 hours after surgery if not contraindicated. Once tolerating oral intake, ibuprofen is then prescribed. Closed suction drains are removed when the output is generally <100 mL per 24 hours. Patients are discharged to home when they are ambulating without difficulty, tolerating a regular diet, and have adequate pain control.
Management of intraoperative complications
Carbon dioxide (CO2) embolus
A CO2 embolus can occur from the pneumoperitoneum, especially if an injury occurs to a vein. If a large CO2 embolus occurs, the presentation can be quite dramatic with hypotension, hypoxemia, and cardiovascular collapse. If the CO2 embolus is small, the first sign can be an abrupt decrease in end-tidal CO2, which is a sign of decreased cardiac output. When this occurs, the blood pressure will subsequently plummet. Needless to say, when CO2 embolism occurs, the first step is release of pneumoperitoneum and hemodynamic support by the anesthesiologist. If cardiovascular collapse occurs, the robot should be undocked, the patient placed in the left lateral decubitus position, and supportive measures should be performed.
Vascular
Major vascular injuries can also occur during robotic LN dissection. When these happen, the anesthesiologist should be made aware immediately for the potential need for blood products, and a consultation with a vascular surgeon might be prudent. Repair of these injuries can be performed robotically by the experienced robotic surgeon. If the decision is made to convert to open surgery, however, the injured vessel should be grasped with an atraumatic robotic instrument to not only tamponade the bleeding but also assist as a landmark in identification of the injured vessel.
Bowel injury
The surgeon should always be cognizant of the location of the bowel in relation to the working field. A thermal injury to the bowel can go unrecognized at the time of surgery, and the patient may present several days postoperatively with peritonitis. This can be avoided with careful handling of the bowel and avoidance of thermal energy in close proximity to the bowel. Rectal injury can also occur during the posterior dissection of the bladder and prostate with an increased incidence postradiation therapy. A rectal injury can usually be diagnosed at the time of surgery. If there is suspicion for such an injury, a digital rectal examination should be performed. An alternative strategy is to place a red rubber catheter per rectum, irrigate the pelvis with fluid through the suction irrigator, and inflate air through the red rubber catheter using a bulb syringe. If one sees bubbles in the irrigant, the rectal wall has been violated. If the patient has not been irradiated and there is no gross fecal spillage, the defect can be repaired primarily using robotic assistance. If there is gross fecal spillage or previous history of irradiation, strong consideration should be made for temporary fecal diversion.
Other visceral
Other visceral injuries such as injury to spleen or liver are extremely rare during ARRC. In patients with hepatosplenomegaly, however, care should be taken during initial access to avoid injury to these structures.
Management of postoperative complications
Immediate
Neuropraxia is possible after ARRC and is usually self-limited but may necessitate physical therapy. This complication is usually because of compression from patient positioning during surgery. 8 Similarly, compartment syndrome has been described after a lengthy ARRC in a patient with muscular lower extremities. 3 This complication is managed with fasciotomies and can be avoided by repositioning the patient's legs flat once the ARRC is complete, especially if an extracorporeal urinary diversion is being performed. These complications are entirely preventable with proper attention to patient positioning, padding, and avoidance of prolonged operative times.
Delayed
Ureteroenteric strictures can occur post-ARRC and can be managed either endoscopically or via surgical revision. Symptomatic pelvic organ prolapse has been noted in a few women in our initial experience, which led us to perform a two-layered vaginal closure with strengthening of the pelvic floor structures and suspension to the uterosacral ligaments.
Major Published Series
The ARRC literature includes multiple single-institution case series as well as multi-institutional collaborative data sets (Table 2). Intraoperative outcomes consistently reveal low blood loss for ARRC but lengthy operative times; however, operative times appear to be decreasing as experience increases. Postoperative variables among the ARRC series reveal short hospital stays and acceptable perioperative morbidity. Intermediate-term oncologic outcomes are also starting to trickle in and reveal acceptable 1, 2, and 3-year overall and disease-specific survival for ARRC. Long-term follow-up and results from ongoing randomized trials will illustrate further oncologic success of ARRC.
Total OR time inclusive of cystectomy, lymphadenectomy, and urinary diversion.
Includes OR time for RARC only.
260 for RARC+extracorporeal ileal conduit and 308 for RARC+extracorporeal orthotopic neobladder.
LN=lymph node; EBL=estimated blood loss; OR=operating room; IC=ileal conduit; NB=orthotopic neobladder; CC=continent cutaneous; DSS=disease-specific survival; IRCC=International Robotic Cystectomy Consortium; NR=not reported; RARC=robot-assisted radical cystectomy.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.