
Abstract
Background and Purpose:
Visual internal urethrotomy (VIU) is an option for the management of urethral stricture. However, little is known regarding sexual function after surgery.
Patients and Methods:
Seventy-six patients who underwent VIU were evaluated by using the Korean version of the Male Sexual Health Questionnaire. Three sexual functional domains of erection (EFD), satisfaction (SAD), and ejaculation (EjFD) were assessed at baseline, 3 months, 6 months, and 12 months after surgery. We assessed clinical factors (age, etiology, and maximum flow rate) and radiologic factors (stricture site, stricture length, frequency of recurrence, and duration until first recurrence). We compared with each sexual functional domain score by age group (range: 40–49, 50–59, 60–69, and 70–79 years).
Results:
A total of 76 men with mean age of 57.1±13.07 years completed this study. In univariate analysis, there were significant losses of EFD scores at postoperative 3 months for all age groups (P<0.05). And these scores were regained after postoperative 6 months. There was no statistically significant difference in SAD. Age, length of stricture, frequency of recurrence, and duration until first recurrence were significant differences in EjFD (P<0.001, P=0.006, P=0.005, and P=0.013, respectively). In 40 to 49 and 50 to 59 age groups, VIU improves EjFD (P<0.001, respectively). Multiple linear regression analysis revealed that age and stricture length were independent factors of VIU on EjFD (P<0.001 and P=0.013, respectively).
Conclusions:
VIU can improve ejaculatory function in younger age group (40–59 years). Age and stricture length are independent predictive factors of VIU on ejaculatory function.
Introduction
Visual internal urethrotomy (VIU) is an option for the management of urethral stricture. Because it is an easy and minimally invasive technique, it has been usually selected in case of relatively short urethral stricture. 2,3 The short-term success rate of VIU is from 39% to 73% for strictures shorter than 1.5 cm, whereas the long-term recurrence rate varies from 26.9% to 56%. 4 –6 Until now, most of outcomes have conventionally focused on urodynamic parameters, such as maximum flow rate (MFR). 6 But little is known regarding sexual functional outcomes after VIU.
Sexual functional outcomes can easily be investigated using a validated, self-administered questionnaire on erection, ejaculation, and sexual satisfaction, namely, the Male Sexual Health Questionnaire (MSHQ). 7 We evaluated the impact of VIU on sexual function using a validated questionnaire and focused on the correlations between sexual functional scores and various clinical factors of VIU.
Patients and Methods
Study population
A prospective evaluation of adult male patients was performed between January 2006 and April 2009 at a single institution. Seventy-six patients who had undergone VIU were enrolled in this study. Inclusion criteria were International Index of Erectile Function-5 score>17 8 and intravaginal ejaculatory latency time >2 min. 9 Patients were excluded if they had any one of the following: a malignant neoplasm of the genitourinary tract, a history of vascular surgery and coronary artery bypass grafting, or severe hepatic and renal dysfunction. Prior to undergoing VIU, we assessed clinical (history, age, etiology of stricture, and MFR) and radiologic factors (stricture site and stricture length) by the retrograde urethrography (Table 1). Before initiating this study, we had informed consent from all the patients and gained approval from our local institutional review board.
By paired samples t-test, comparison with before and 12 months after surgery.
P<0.001, comparison with the baseline values, but not significantly correlated with MSHQ domains.
MSHQ=Male Sexual Health Questionnaire.
Surgical techniques
VIU at the 12 o'clock position was performed under general anesthesia using a 21F Storz urethrotome with a straight cold knife. After urethrotomy, an 18F Foley catheter was inserted into the bladder through the urethra and removed at 2 weeks after surgery. All operations were performed by a single surgeon. Recurrence was defined if a patient required another operation or additional procedure, such as urethral dilatation. All patients were confirmed recurrences by retrograde urethrography. Frequency of recurrence and duration until first recurrence were assessed during follow-up periods when patients visit outpatient department (Table 1).
Description of validated questionnaire
The Korean version of the MSHQ is a validated, self-administered questionnaire that is used widely for the evaluation of male sexual function. We evaluated adult male sexual function using a three-item erectile functional domain (EFD; range: 0–15), a seven-item ejaculatory functional domain (EjFD; range: 6–30), and a six-item satisfaction domain (SAD; range: 1–35). 7
All patients completed a preoperative MSHQ to determine baseline sexual function and a repeat MSHQ was given on postoperative visits at 3, 6, and 12 months. Because we thought sexual functional scores may have correlation with age, respective MSHQ domain scores were stratified by age groups (range: 40–49, 50–59, 60–69, and 70–79 years). 10 But sample size was so small in 60 to 69 and 70 to 79 age groups (n=15 and n=13, respectively). To figure out comprehensive pattern, we divided the patients into two age groups (young group, 40–59 years; old group, 60–79 years) and analyzed the EjFD item scores in detail (Fig. 2).
Statistical analysis
We used the paired samples t-test and one-way analysis of variance to compare stratified by age groups before and after surgery. Univariate analysis was tested to identify clinical and radiologic factors associated with sexual functional outcomes. Thereafter, the significantly associated variables were used with multiple linear regression analysis to identify the independent predictors. Statistical analysis was performed by using SPSS version 18.0 (SPSS, Inc., Chicago, IL). Values of P<0.05 were considered statistically significant.
Results
A total of 76 patients were included in this study. The mean age was 57.1±13.07 years (range: 43–77 years) and the mean follow-up was 17.5±5.3 months (range: 12–38 months). The etiology of stricture was traumatic in 26, inflammatory in 16, idiopathic in 27, and iatrogenic in 7. The urethral stricture site was bulbous in 28, membranous in 40, and multiple in 8. The improvement of MFR was 3.76±2.33 m/s. The mean stricture length was 1.86±0.93 cm. The mean frequency of recurrence was 1.50±0.74 times. The mean duration until first recurrence was 10.50±6.76 months (Table 1).
In the univariate analysis of clinical factors, there were no significant differences in EFD and SAD scores before and after surgery. But age, stricture length, frequency of recurrence, and duration until first recurrence were significantly different in EjFD scores before and after surgery (P<0.001, P=0.006, P=0.005, and P=0.013, respectively).
We stratified respective MSHQ domain scores by age groups (Table 2). There were significant losses of EFD scores at postoperative 3 months in all age groups and these scores were regained at postoperative 6 months (Fig. 1). In comparison with baseline and postoperative 12 months, there were no significant differences in the mean scores for the EFD and SAD. In 40 to 49 age group, there was a significant increase in EjFD score from 31.1 to 34.4 (P<0.001) and similar pattern was seen in 50 to 59 age group, EjFD score from 29.7 to 32.6 (P<0.001).
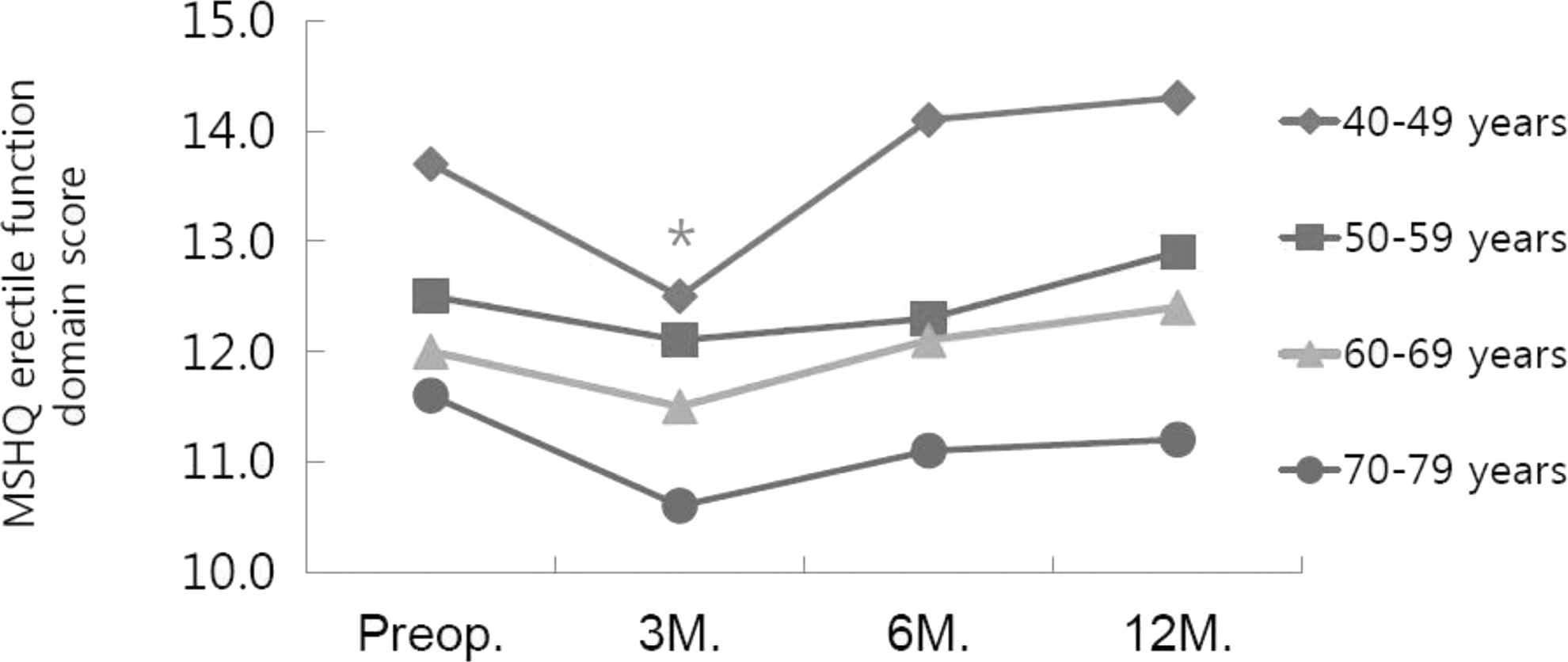
MSHQ erectile functional domain (EFD) scores between preoperative and postoperative 12 months. The symbol * represents significant losses of EFD scores at postoperative 3 months in all age groups (P<0.05), comparison with baseline values by paired samples t-test. MSHQ=Male Sexual Health questionnaire.
By paired samples t-test, comparison with before and 12 months after surgery.
P<0.05, comparison with the baseline values.
We divided the patients into two age groups (young group, 40–59 years; old group, 60–79 years) and analyzed the EjFD item scores in detail (Fig. 2). In old group, all EjFD item scores were not significantly different before and after surgery. But there was a significant difference for the pain item of EjFD in young group (P<0.005).

Score for MSHQ ejaculatory functional domain item between baseline and postoperative 12 months.
Multiple linear regression analysis revealed that frequency of recurrence and duration until first recurrence were not significantly different in EjFD scores (P=0.395 and P=0.834, respectively). But age (unstandardized coefficient beta [B]=−0.155; adjusted R 2 =0.874; P<0.001) and stricture length (B=−0.603; adjusted R 2 =0.826; P=0.013) were independent predictive factors of VIU influencing EjFD (Table 3).
SE=standard error; T=test statistic; CI=confidence interval.
Discussion
Since the introduction by Sachse in 1971 11 of the technique and instruments for direct vision internal urethrotomy, this method has gained a widespread treatment for the management of urethral strictures. The technique of VIU is simple, precise, and a low incidence of complications. 12,13 Many literatures reported the short- and long-term results of voiding symptoms after VIU. 4 –6 Although sexual function is a predictor of patient's satisfaction after surgery of urethral strictures, little has been reported regarding the impact of VIU on male sexual function.
More studies were discussed about male sexual function after urethral reconstructive surgery, such as open urethroplasty. One report suggested that the nervous input for EF lies generally outside the corpus spongiosum; no changes occur in EF. 14 Another study even reported an improvement in EF after urethroplasty. 10 The other study reported decline of EF after anterior urethral reconstructive surgery. 15 Because VIU is easy, precise, and minimally invasive technique than urethral reconstructive surgery, our study design was focused on the changes in male sexual function according to the resolution of urethral obstruction after minimally invasive surgery.
In an attempt to assess male sexual function, we evaluated patients using the MSHQ—a standardized, validated questionnaire intended to monitor EFD, SAD, and EjFD before and after surgery. In our series, preoperative EFD, SAD, and EjFD scores were 12.7, 25.8, and 30.3, respectively. Because there were no available normative MSHQ scores in our country, we compared our data with other studies using the MSHQ in our country. Song et al reported effect of tamsulosin on ejaculatory function. 16 Baseline MSHQ scores of EFD, SAD, and EjFD were 9.74, 19.49, and 25.06, respectively. Lee et al reported effects of components of metabolic syndrome on sexual function in Koreans. 17 A total of 602 men were included; EFD, SAD, and EjFD scores were 8.25, 19.13, and 23.12 by moderate lower urinary tract symptoms.
In our series, there were no significant changes between the EFD scores and the various clinical factors in the univariate analysis (Table 1). In comparison with baseline and postoperative 12 months, there were increases in EFD scores for 40 to 49, 50 to 59, and 60 to 69 age groups. But there were no statistically significant increases (Table 2). Interestingly, all age groups lose EFD scores significantly at postoperative 3 months and regained them after postoperative 6 months (Fig. 1). It appears that postoperative EF heals with time. Dogra et al 18 analyzed that recovery of EF occurs in more than 96% of cases within 6 months after urethroplasty and argued that physical (decrease in tissue swelling) and psychosomatic recovery occurring during this period may relate to healing of EF and penile sensitivity. Erickson et al 10 also suggested that substantial psychological and physical recovery occurs during this healing period. But the clinical relevance of this healing period is unclear. We can only speculate that healings in EF happen in this period. In our series, EFD score for 70 to 79 age group has a slight decrease (Table 2). Although this was not statistically significant, this finding probably reflects that age relates to the recovery of EF. In older age, a longer healing period may be needed. A large-scale, prospective trial will further elucidate the impacts of VIU on EF.
In our series, there were no significant differences between the SAD scores and various clinical factors in the univariate analysis (Table 1). When we stratified SAD by age group, 40 to 49 and 50 to 59 age groups scored quite higher SAD scores after surgery, respectively, and 60 to 69 and 70 to 79 age groups appeared to have lower SAD scores after surgery, respectively. But there were no differences between the SAD scores before and after surgery (Table 2). The clinical significance of this is unknown.
During ejaculation in young men, the muscles in the epididymis, seminal vesicles, vas deferens, and prostate contract automatically. This mechanism propels semen forward. At the same moment, nerve impulses tighten muscles in the bladder neck so that semen is forced out through the urethra instead of back flowing into the bladder. The enjoyable sensation of orgasm usually happens with ejaculation. The resolution of urethral obstruction by VIU can attribute improvement of ejaculatory function. But in older men, the increased rate of ejaculatory dysfunctions was observed. 19 During ejaculation in older men, the muscular contractions of orgasm are less extreme, semen volume declines, and ejaculation is prolonged and less urgent. In this situation, we believe that the resolution of urethral obstruction by VIU cannot improve male ejaculatory function.
In our series, age was an independent predictive factor on ejaculatory function after VIU (B=−0.155; adjusted R 2 =0.874; P<0.001). When we stratified EjFD scores by age group, there were significant increases in 40 to 49 and 50 to 59 age groups after surgery (P<0.001 and P<0.001, respectively). But there were slight decreases in 60 to 69 and 70 to 79 age groups (P=0.071 and P=0.064, respectively). Erickson et al 10 reported improvement on ejaculatory function after urethroplasty in younger age group (≤49 years). They asserted that resection of the scarred and a contractile part of urethra/spongiosum improves the rhythmic ejaculatory mechanism by restoring the continuity of the musculature.
Some patients have ejaculatory pain or discomfort during ejaculation. We think that these symptoms are caused by obstruction on the pathway of ejaculation after urethral stricture. In our study, EjFD scores about pain during ejaculation were improved in young age group than that in old age group after VIU (Fig. 2). So, VIU can be not only the resolution of the lower urinary tract but also the secure of the pathway of ejaculation.
We analyzed the correlation between EjF and MFR in this study. After postoperative one year, MFR was significantly improved (P<0.001), but the correlation between EjF and MFR was not significantly matched (Table 1). We think the reason is as follows. At first, the severity of the obstruction can impair EjF, but MFR cannot always reflect the severity of the urethral obstruction. Voiding has different mechanism from ejaculation. Voiding should consider interaction of detrusor function, sphincteric movement, prostate volume, and so on. With this background, the patient who has improved EjF by VIU may not improve MFR due to the other urologic problems. The resolution of urethral obstruction absolutely contributes to improvement in ejaculatory function. But the limitation is difficult to measure the severity of the obstruction. The accurate measurement of maximum ejaculatory flow rate is practically impossible. Intraoperative urethroscopic findings also can be important, but the problem exists that it is subjective. At second, we evaluated EjF using the MSHQ. In this study, the improvement of EjF means to gain more EjFD item scores. EjFD scores about pain during ejaculation were more gained in young age group, significantly (Fig. 2). So, we think that this point probably reflects the improvement of EjF.
Stricture length often correlates to the severity of fibrosis within the urethra and surrounding tissues. Long strictures are often associated with inflammatory disease, repeated urethral dilations, and traumatic urethral distraction. 20 In our series, stricture length was an independent predictive factor for impact on ejaculatory function after VIU (B=−0.603; adjusted R 2 =0.826; P=0.013). There were no evidence about the correlation between stricture length and ejaculatory function. However, Byun and Song reported that 41% of all patients with a stricture length of 0.5 to 1.5 who underwent a second VIU, and that 71% of all patients with a stricture length of 1.5 to 2.5 cm who underwent a second VIU. 21 Huh et al reported that the success rate of the first VIU was 81.8% for stricture lengths of 0.5 to 1.0 cm and 33.3% for stricture lengths of 1.6 to 2.0 cm. 22 These reports suggest that stricture length related with success rate and recurrence rate of VIU. We speculate that the lower outcomes of voiding function after VIU may reflect the lower outcomes of ejaculatory function.
In the univariate analysis, frequency of recurrence and duration until first recurrence were significantly different in the EjFD scores (Table 1). But there were no significant differences in the multiple linear regression analysis. We think that 12-month follow-up period was not enough to determine whether frequency of recurrence and duration until first recurrence were significant or not. We cannot but count patients with no recurrence (n=22) as a missing value in statistical analysis about recurrence. We think that the small sample size prevented accurate statistical comparison of the clinical factors about recurrence.
Our limitation of the present study concerns the use of self-administered questionnaire for assessing sexual dysfunction. This may cause respondents for response bias, as they overestimate or incorrectly report their sexual dysfunction symptoms. We did not measure objective data, such as ejaculate volumes, but depended on patients' self-assessments in the MSHQ. Measuring ejaculate volumes may be a better way to further evaluation. Follow-up period was not enough to understand variable clinical manifestations after surgery.
Despite these weaknesses, our data suggest that the younger men can expect improved ejaculatory function after VIU and stricture length was a predictor to improve ejaculatory function after VIU for urethral stricture. Large-scale, prospective, longer term follow-up trials will further elucidate the impacts of VIU on sexual function. We are conducting a prospective study that accesses the correlation between sexual function and voiding function, such as International Prostate Symptom Score and uroflowmetry. A physician should keep in mind that, in urethral diseases, urosexual functional problems coexist after single surgery.
Conclusions
The MSHQ is a simple and useful tool to measure male sexual function after VIU. Using the validated questionnaire, we showed that VIU can improve ejaculatory function in younger age group (40–59 years), and age and stricture length are independent predictive factors of VIU on ejaculatory function.
Footnotes
Disclosure Statement
No competing financial interests exist.