
Abstract
The preservation of sexual potency after radical prostatectomy has always been the topic of much anxiety and debate. While cancer control and urinary continence are of supreme importance, the preservation of sexual function completes the trifecta that both patient and surgeon strive to achieve. The introduction of robotic assistance to modern laparoscopic surgery has provided many advantages, the two greatest being improved three-dimensional magnified vision and wristed instrumentation. These technical enhancements provide the surgeon with improved surgical tools that have the potential to facilitate a more precise surgical approach. One of the potential advantages during robot-assisted laparoscopic prostatectomy (RALP) is improving visualization, control, and dissection of the neurovascular bundle (NVB). With this article, we provide the description of our current technique of intrafascial, tension and energy-free dissection of the NVB during RALP, aiming to maximize the preservation of the periprostatic neuronal network and improve erectile function outcomes. A step-by-step description of the preservation of the pubovesical complex is also provided.
Introduction
Optimally, when a surgical approach is used to treat patients with PCa, the operation removes the cancer completely with negative surgical margins, avoids excessive blood loss or serious perioperative complications, and culminates in complete recovery of continence and potency. 2 To achieve this, the surgeon must treat sufficient periprostatic tissue to achieve cure while preserving the periprostatic neuronal network needed for erectile function (EF) and the neuromusculature needed for normal urinary and bowel function.
With the advent of robotics, there has been greater emphasis on full nerve sparing with progressive development of techniques achieving the intrafascial plane of dissection—considering that the recovery of EF is correlated with the amount of residual neurovascular bundle (NVB) resected with the prostate. 3
With this article, we provide the description of our current technique of intrafascial, tension and energy-free dissection of the NVB during robot-assisted laparoscopic prostatectomy (RALP), aiming to maximize the preservation of the periprostatic neuronal network and improve EF outcomes. A step-by-step description of the preservation of the pubovesical complex (PVC) is also provided.
Methods
Indications
Ideally, intrafascial nerve-sparing RALP should be attempted in preoperatively potent patients—and strongly motivated to maintain postoperative EF—with low risk for extracapsular disease (T1c, Gleason score <7, and prostate-specific antigen level <10 ng/mL) and with at least 10 years of life expectancy.
The intrafascial approach is not offered in cases of locally advanced disease or for patients with preoperative erectile deficit or not interested in maintaining potency.
Morbid obesity as well as previous abdominal surgery are not absolute contraindications to this approach; however, they may increase the length of the procedure. Prostate size does not seem to affect our outcomes.
Preoperative workup
We wait at least 2 months after prostate biopsy before the surgery to reduce the periprostatic inflammation caused by the biopsy. After transurethral resection of the prostate, we recommend waiting 3 to 4 months. Discontinuation of aspirin and antiplatelet agents is needed for at least 10 days before surgery.
All patients undergoing RALP have an endorectal MRI to obtain an accurate local staging of the disease, 4 including the challenging anterior part. 5 For PVC preservation, at least two biopsies per side of the anterior prostate were added to the standard scheme.
Preoperative workup includes complete blood cell counts, electrolyte and coagulation profiles. Chest radiography and electrocardiography are also obtained.
Preoperative preparation
The patient is admitted to the hospital 1 day before the surgery. A Fleet® enema is administered the evening before the surgery. Fasting starts at midnight before surgery. Thromboprophylaxis is implemented with good hydration and low-molecular-weight heparin—at least for high-risk patients. No additional bowel preparation is routinely performed.
Instrumentation
Robotic instruments
We use the da Vinci® Si robot system with four multijoint robotic arms, with one controlling a binocular endoscope and the other three arms controlling articulated instruments. A 0-degree lens is used. Endowrist bipolar and atraumatic graspers, Endowrist round tip scissors, and Endowrist needle driver are used. The distribution of these instruments from the left to the right side of the patient is bipolar grasper, atraumatic grasper, lens, and monopolar scissors. At the step of the vesicourethral anastomosis, scissors are exchanged with the needle-holder, while we change the position of the other two instruments (atraumatic and bipolar graspers).
Laparoscopic instruments
A standard laparoscopic kit including reusable instruments is used by the assistant (Johann fenestrated atraumatic grasper (Microfrance), suction irrigator with long suction cannula, T-Challenger clip applier (B-Braun), fine-dissection grasper (Microfrance). Both robotic and laparoscopic trocars are reusable except from the first one, for the robotic lens, that is disposable. The specimen retrieval bag is also disposable.
Sutures
A 30-cm V-lock stitch 3-0, 17 mm, ½ c is used to perform the urethrovesical anastomosis. Alternatively, Monocryl (poliglecaprone 25) 3-0, 22 mm ½ c may be used. When a ligation of the dorsal vascular complex (DVC) is needed, then a Vicryl 0 (polyglactin 910) needle 26 mm ½ c is used.
Surgical Technique
The patient is prepared and draped in the supine position with the legs abducted. A nasogastric tube and a bladder catheter are placed.
Trocar placement
The first port to be placed is the 12-mm trocar for the camera, which is positioned at the supraumbilical crease in the midline. The first robotic operative port for the scissors is placed close to the lateral border of the right rectus muscle midway between the umbilicus and the pubic symphysis. The second robotic port, for the bipolar forceps, is placed as lateral as possible and about 3 fingerbreadths from the left anterior-superior iliac spine. The third port, for the robotic grasp, is placed slightly medially to the left border of the rectus muscle at the same height as the camera. Two more 5-mm ports for suction, clip device, and assistance with atraumatic laparoscopic grasp are placed between the camera port and the right robotic port as far as possible to avoid conflicts.
First steps of surgery
With the patient in a steep Trendelenburg position, the peritoneal cavity is inspected. The sigmoid colon is freed from its adherences to the lateral abdominal wall and together with small bowel loops, it is moved cranially to free the Douglas space. A peritoneal incision is then performed extending from the left to the right medial umbilical ligament in to detach the bladder from the anterior abdominal wall. This incision is extended in an inverted U to the level of the vasa on either side and the space of Retzius is entered. A complete lateral dissection of the bladder should be achieved to avoid tension when performing the urethrovesical anastomosis. The ventral prostatic surface is cleaned by the adipose tissue to put in evidence the pubovesical ligaments and the reflection of the endopelvic fascia.
Nerve-sparing technique: The lateral dissection
We start our dissection on the right side. The fat tissue between the base of the prostate and the bladder laterally to the pubovesical ligaments marks the starting point of our “hole-shaped” dissection. Usually an anastomotic vein connecting the DVC to the right NVB lies here (Fig. 1). At this point, the dissection is carried out in depth; the assistant aids in the development of this avascular plane by inserting and carefully opening an atraumatic grasper (Fig. 2). Some arteries from the NVB to the base of the prostate are encountered; they are carefully dissected, clipped, and divided. The NVB is freed from the base of the prostate (Fig. 3).
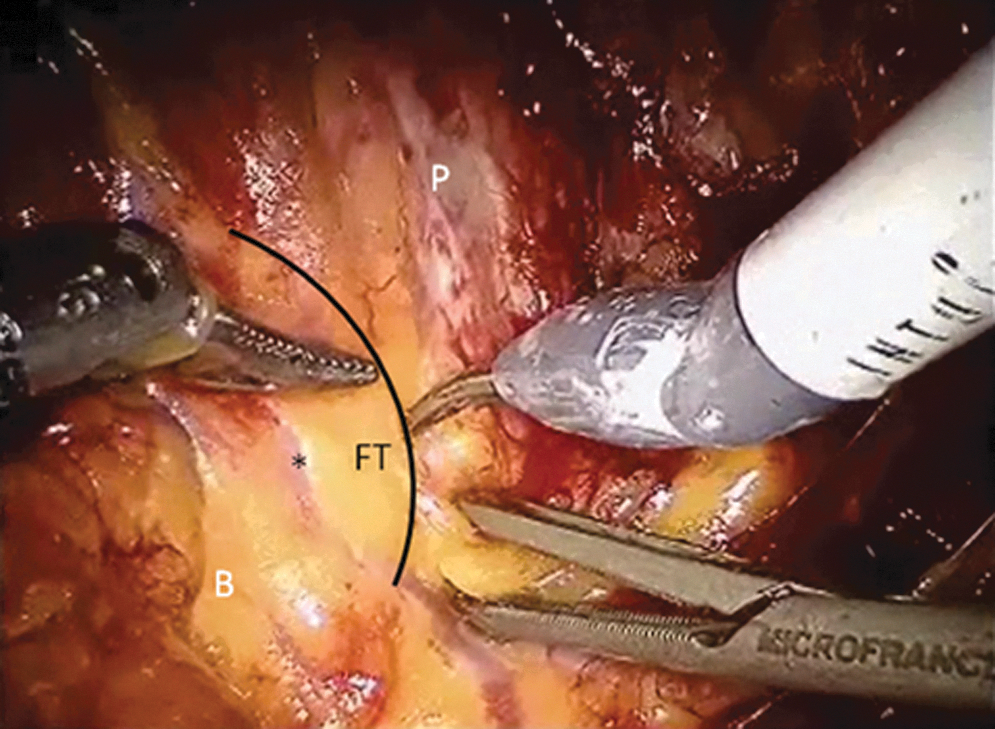
The black line marks the limit between base of the prostate (P) and bladder (B). FT=fat tissue, *=anastomotic vein.
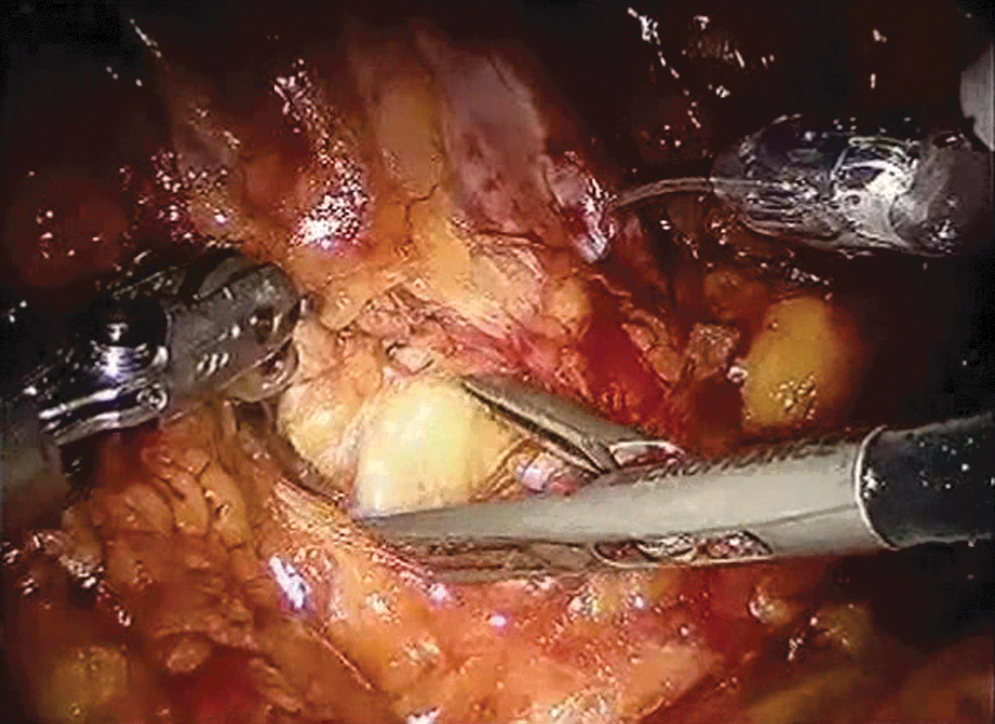
Hole-shaped dissection between base of the prostate and bladder. The assistant helps in the development of this avascular space with a grasper.
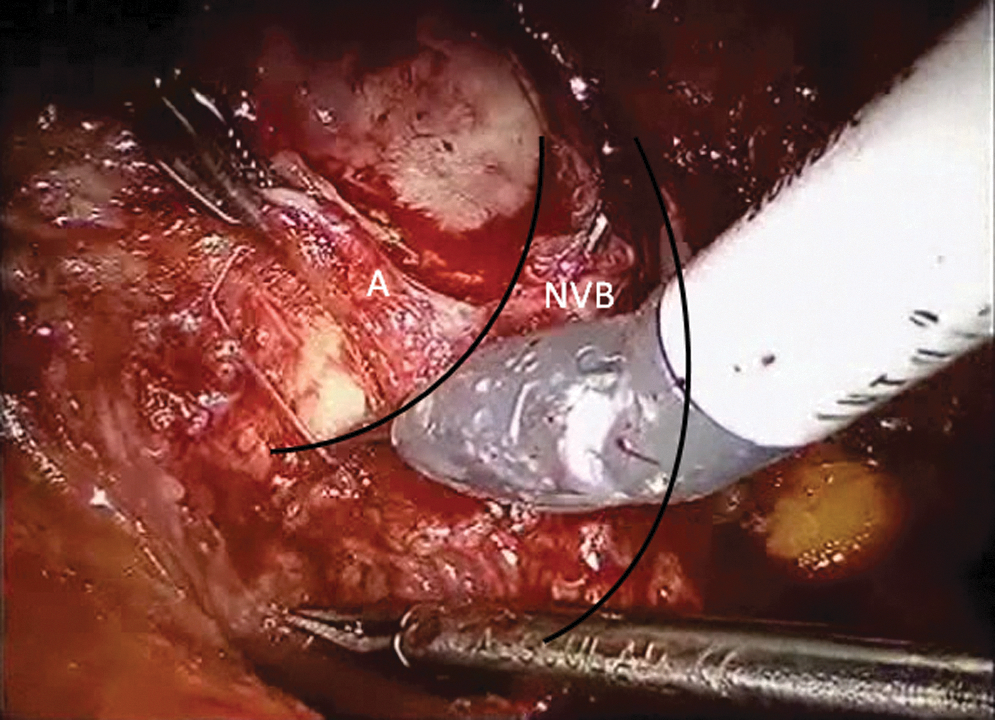
The neurovascular bundle (NVB, between the two black lines) is being released by the prostatic base. Small arteries (A) for the base of the prostate are carefully dissected, clipped and divided.
The posterior prostatic fascia is reached in depth, and it represents the posterior limit of our intrafascial dissection (Fig. 4). At this point, the lateral and posterior surfaces of the prostate have been delimited.
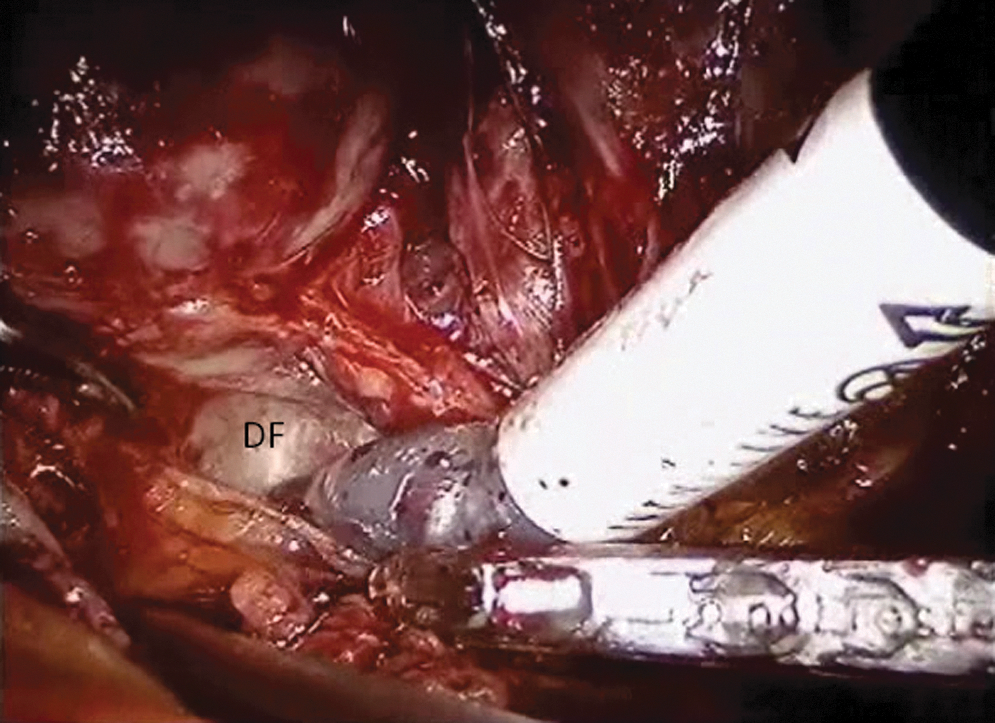
The hole-shaped dissection at the level of the prostatic base proceeds in depth until the Denonvillier fascia (DF). At this step, both the lateral and posterior surface of the prostatic capsule have been delimited.
We subsequently perform a high anterior, intrafascial release of the NVB (by opening both the endopelvic and the prostatic fascia at the 2 o'clock position) following the principles of tension- and energy-free dissection (Fig. 5). The curve that the NVB describes on the lateral surface of the midprostate as well as variations in the course of the bundle from modifications of the prostate volume are respected. A lateral displacement that peels away the NVB from the prostate is avoided to minimize stretch neuropathy and neurapraxia that adversely affect recovery of sexual function. The robotic scissors are rather spread longitudinally along the prostatic capsule and medially to the NVB followed by sharp dissection. In this way, the NVB is freed without tension. Major attention should be given in the dissection of the NVB toward the apex, because one or two small arteries leave the bundle to enter the prostate, and traction on them could cause tear of the capsule. These small arteries should be identified, clipped, and divided.
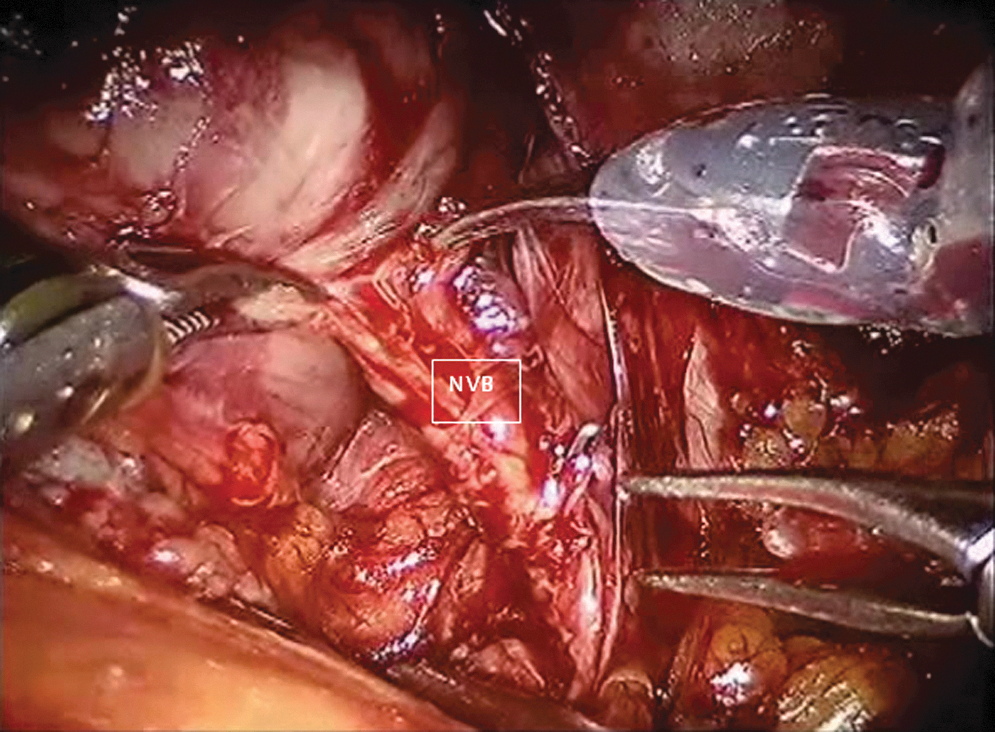
Dissection of the neurovascular bundle (NVB) from the lateral prostatic surface, right side. Small arteries penetrating the prostate are managed carefully with clips; peeling movements on the NVB are avoided to reduce neuroapraxia and the risk of tears of the prostatic capsule.
Using the same lateral approach, the right prostatic apex is prepared. With the right lateral surface of the prostatic capsule and the prostate apex totally dissected, we return to the prostate-vesicular angle. The omolateral vas deferens is cut while the tip of the seminal vesicle is left in place: Considering its close relationship to the NVB, this maneuver enhances the possibilities of nerve preservation. Small metallic clips are used to control the deferential and vesicular arteries.
The right side of the bladder neck (BN) is then carefully prepared.
We repeat the same type of BN dissection, NVB preservation, and seminal vesicle/vas deferens transection on the left side of the prostate.
With the NVBs totally released, the posterior plane is developed by a lateral approach anterior to the posterior prostatic fascia, which remains in place, covering the perirectal fat. This hypovascular plane can be created easily using blunt dissection. The BN is left intact and preserved: We transect it only at the end of the prostatectomy.
The detrusor apron (DA), part of PVC, is then grasped and pulled on the left by the robotic atraumatic grasper (Fig. 6). With minimal use of cautery, the DA is then dissected by the ventral surface of the prostate.
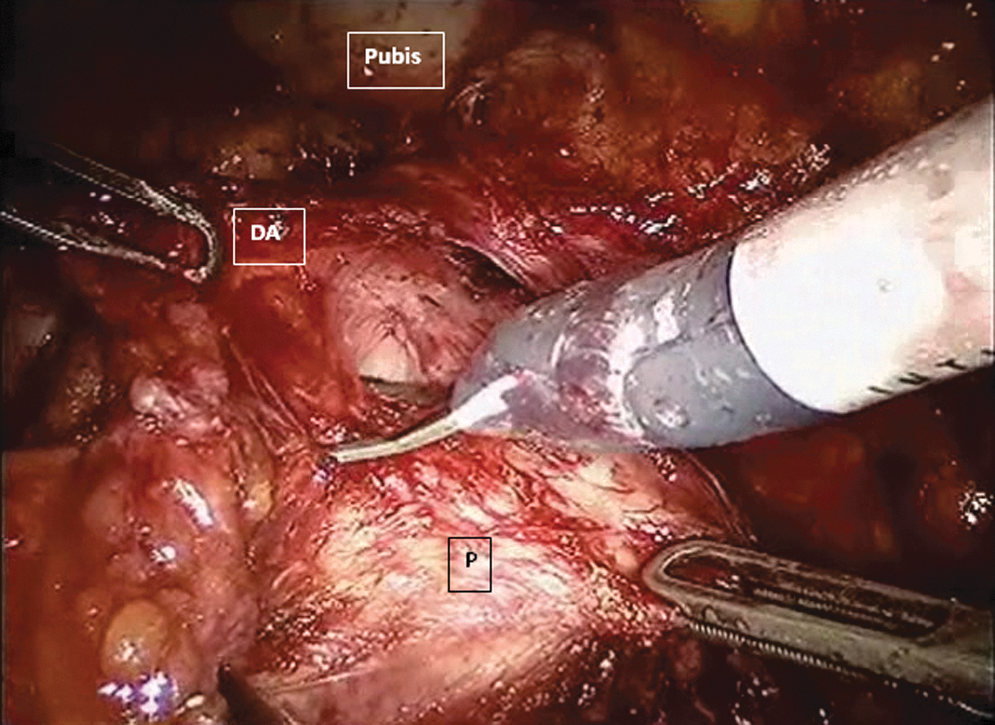
Dissection of the detrusor apron (DA) by the ventral prostatic surface. Minimized cauterization followed by sharp dissection maintains clear the native anatomy. The robotic grasper pulls the DA on the left while the assistant pulls the prostate (P) on the right. Observe the insertion of the DA at the pubis (pubovesical ligaments).
At the level of the apex, we identify the avascular plane between DVC and urethra, under the DVC. 6 The urethra is then dissected into the prostatic notch and transected sharply 5 mm distal to the notch. It is important to ensure that there is no apical tissue behind the urethra to avoid cutting into the posterior aspect of the apex and create a positive surgical margin. The cavernosal nerves are close to the urethra and are vulnerable to thermal or traction injury at this step of dissection. Specific attention is also needed in case of the presence of an accessory pudendal artery, which absolutely must be preserved. Finally, care should be taken to avoid inadvertent rectal injuries.
At this moment, the prostate is still attached cranially at the BN (Fig. 7). The gland is pulled by the assistant on the right side while the robotic grasper pulls the DA on the left. The last ventral attachments are freed.
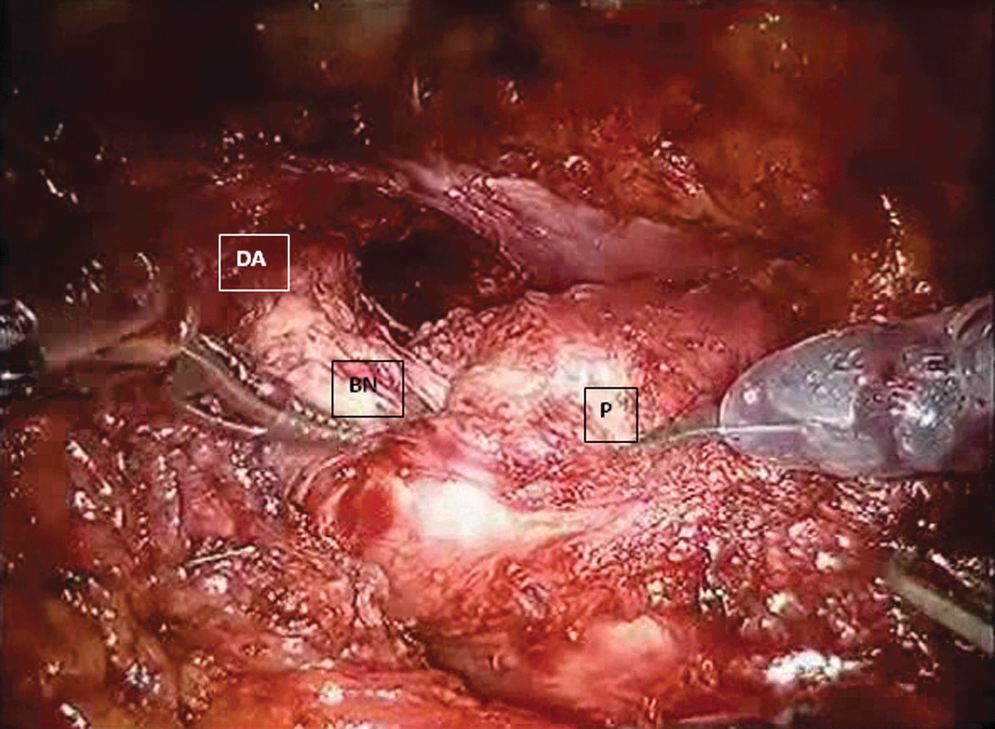
Detrusor apron (DA) completely dissected by the ventral prostatic surface. Lateral view of the spared bladder neck (BN) entering in the prostate (P) completely pulled on the right.
At the end, the BN is dissected and divided by a BN-sparing technique.
Hemostasis is controlled before proceeding to the anastomosis.
Finally, a running urethrovesical anastomosis is performed with a 30 cm V-Lock 17-mm ½ c stitch by starting and finishing at the 5 o'clock position. The anastomosis can be performed entirely at the right side of the preserved PVC or in two halves, on the right and left side of the PVC, passing the needle under this complex as necessary. An 18F Foley silicon catheter is placed with 10 mL of saline in the balloon. The final aspect of the surgical field is shown in Figure 8.

Final aspect. The totally preserved pubovesical complex (PVC) in place. All the surgical steps have been performed under and laterally to this complex. The naturally present pubic attachments of the bladder are preserved.
It is important to underline that the DVC has been totally spared, and consequently no ligation is needed.
The anastomosis (as well as any inadvertent vesical injury) is tested for any leaks with 200 mL of saline.
No drain is usually used in our clinical practice. When necessary, a Jackson-Pratt drain is placed through the left 5-mm port. The specimen is removed in a retrieval bag after enlarging the umbilical port incision as needed.
Postoperative care
If placed, the drain is removed when the volume is <100 mL/d or in the absence of any suspicious sign of urinary fistula. Patients are regularly discharged on postoperative day (POD) 5 with the Foley catheter still in place; the catheter is then electively removed on POD 9 on an outpatient basis without previous cystography.
Management of complications
A recent meta-analysis 7 comparing the radical prostatectomy (RP) approaches with regard to complication rates demonstrated that total intraoperative complication rates and mortality rates were low for all surgical modalities (retropubic-RRP, laparoscopic-LRP, and RALP), suggesting that RP is a safe procedure. Total intraoperative complication rates were significantly higher for RRP (1.5%) vs RALP (0.4%) (P<0.0001) and for LRP (1.6%) vs RALP (0.4%) (P<0.0001). For total perioperative complication rates (17.9% RRP, 11.1% LRP, and 7.8% RALP), RALP vs RRP (P<0.0001) and vs LRP (P=0.002) were significant. According to these outcomes, RALP shows the lowest morbidity among the surgical approaches of RP.
The treatment of the most common intraoperative and perioperative complications that may be encountered during RALP is summarized in the Tables 1 –3. Tips for preventing complications are also provided according to the published literature. 8 –10
RP=radical prostatectomy; DVT=deep vein thrombosis; CT=computed tomography.
CT=computed tomography; RP=radical prostatectomy; TURP=transurethral resection of the prostate; BN=bladder neck.
NVB=neurovascular bundle.
Summary of the Major Published Series of RALP on Overall Potency Results
Accordingly to a recent meta-analysis, 11 nerve-sparing RALP was associated with an incidence of 12- and 24-month erectile dysfunction ranging from 10% to 46% and from 6% to 37%, respectively. The mean values of the 3-, 6-, 12-, and 24-month potency recovery rates were 50% (32–68%), 65% (50–86%), 70% (54–90%), and 79% (63–94%), respectively. 11 Differences in the definitions and measures of erectile dysfunction, in the characteristics of the surgery (surgical technique, use of energy, experience of the surgeon, plane of fascial dissection) and patient selection as well as in the postsurgical rehabilitation may explain these widely different rates of erectile dysfunction.
The mainstay to EF recovery is maximizing the preservation of the periprostatic neuronal network (ideally achieved through an intrafascial dissection of the NVB) followed by avoidance of traumatic or thermal injury. Theoretically, the tridimensional magnification, scaling of movements, and seven degrees of freedom associated with the robotic technology could significantly simplify and improve the results of nerve-sparing procedures. Actually, a recent meta-analysis shows for the first time a significant advantage in favor of RALP in comparison with RRP in terms of 12-month potency rates combined to a nonstatistically significant trend in favor of RALP after comparison with LRP. 11 Tewari and associates 12 also showed a significantly shorter time to reach erections in patients who underwent RARP compared with those receiving RRP, while Asimakopoulos and colleagues 13 confirmed this outcome in a prospective randomized trial comparing RALP with LRP.
Conclusions
The better vision offered by the robotic platform combined with the ability to perform millimetric dissection of the NVBs allows the surgeon to follow anatomic planes that are very hard to develop through classic retropubic or laparoscopic surgery and consequently to maximize the preservation of the periprostatic neuronal network minimizing stretch neuropathy phenomena. In the hands of an experienced surgeon, the robotic platform enhances the possibilities of a total respect of the periprostatic anatomy, leading, according to the most recent literature, to less complications and better functional outcomes. It seems that the era of a new gold-standard surgical treatment in the field of RP has arisen.
Footnotes
Acknowledgments
The first author is a scholar of Alexander S. Onassis Public Benefit Foundation.
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.