
Abstract
Introduction:
The application of robotic-assisted radical prostatectomy has increased considerably over the past decade, but there remains a paucity of standardized complications reporting associated with this procedure. The complications literature regarding robotic prostatectomy is wrought with limitations, variability, and bias making meaningful comparisons between surgical series difficult.
Materials and Methods:
From November 2006 to December 2010, a total of 575 patients were evaluated. Data were assimilated through an IRB-approved blinded prospective database by an independent third party committee. Patients were followed prospectively for 30 days postoperatively. The Modified Clavien system was utilized to grade complications. Grade I and II complications were classified as minor, while grade III, IV, and V were considered major complications. Multiple complications in individual patients were recorded as separate events. Our initial experience and that of our most recent were compared. Age, body mass index, American Society of Anesthesiologists score, Gleason grade, prostate specific antigen, prostate volume, and complications were evaluated.
Results:
Of the 575 patients, 482 (83.8%) had an ideal perioperative course. In the remaining 93 (16.2%) patients, there were 117 complications. Minor complications occurred in 84 (14.6%) and major complications arose in 15 (2.6%) patients. When the first 500 patients were divided into subsets of 100 patients, a linear regression analysis demonstrated no significant difference in overall complications among the five quintiles (p=0.17). The first quintile was found to have a significantly higher major complication rate compared with the second quintile (p=0.05). The subsequent quintiles exhibited no significant change in major complication rate.
Conclusions:
As a surgeon progresses through the learning curve, there is a stable overall complication rate with a drop in major complications after the first 100 cases.
Introduction
The durability of any surgical technique is largely attributed to its efficacy and safety. As the utilization of RARP has increased, numerous reports of complications have been published. Complication reporting is extremely important, but many series are wrought with bias and methodological flaws with significant variability in the definition and classification of a complication. 3 –11 Clavien et al recognized this disparity in the surgical literature and proposed a classification system for complications to standardize reporting. 12 This system was later modified and the reproducibility validated. 13 Critically evaluating the surgical morbidity literature, Martin et al established 10 criteria vital to strengthening the quality of publications. 14 Despite the attention to improving outcomes measurement, a review of the urologic oncology literature revealed that only 2% of the published series met 9 of the 10 criteria, 47% of the minimally invasive series met fewer than 5 of the 10 criteria, and only 19% utilized a numeric grading system of complications. 15
Previously, we reported an overall complication rate for RARP of 17.1% with a major complication rate of 5%. 16 As our case volume continues to grow, we sought to update our prospective analysis of a single-institution experience with the perioperative complications of RARP. Additionally, we sought to define a point at which a consistent drop in major complications was achieved.
Materials and Methods
From the beginning of our institution's robotic program, an institutional review board-approved blinded, prospective database was created and maintained by a third party committee independent of the operating surgeons and house staff. Between November 2006 and December 2010, all patients undergoing RARP were entered into the database.
The database comprised of 575 total patients undergoing RARP performed by one of the three surgeons (J.R., G.H., G.P.). Two of the three surgeons are fellowship-trained in Endourology/Minimally Invasive Surgery (G.H./G.P.), while the third surgeon is not fellowship-trained (J.R.). Further, one surgeon had limited experience with laparoscopic prostatectomy during fellowship and no robotic experience at the onset of the study (G.P.), while the other fellowship-trained urologist had significant exposure to RARP during training (G.H.). Finally, the third surgeon had no robotic experience at commencement of the study (J.R.).
RARP was performed by the individual surgeon according to their preferential technique. Two surgeons performed RARP as described previously in the Vattikuti Institute Prostatectomy (G.H./J.R.), and an initial posterior approach to RARP, more consistent with the Montsouris laparoscopic approach, was utilized by the third surgeon (G.P.). 17,18 Lymph node dissections were performed as deemed appropriate by preoperative risk stratification with a total of 177 patients undergoing node dissection. During this period at our institution, resident involvement was the standard and the extent of involvement gradually increased with resident experience.
Before the initiation of data accumulation, a five-member hospital-appointed panel defined the pertinent data points based on a MEDLINE review of the literature between 2002 and 2007 using the terms, complications and RARP.
We defined an ideal perioperative course as one in which the patient is discharged home from the hospital within 2 days of surgery, the patient's Jackson-Pratt drain is removed before discharge, and there are no unscheduled procedures, studies, hospital admissions, or emergency room visits. Any deviation from this ideal perioperative course was identified and classified as a complication in keeping with the Modified Clavien classification of surgical complications. 13 All patients were prospectively followed for 30 days postoperatively. The inpatient and emergency room electronic record in addition to outpatient records were monitored for identification of complications.
According to the modified Clavien classification, grade I complications encompass any deviation from an ideal perioperative course not necessitating pharmacologic intervention; grade II complications require pharmacologic intervention; grade III complications necessitate surgical, endoscopic, or radiographic intervention; grade IV complications are those that are life-threatening; and grade V complications represent a patient death. In this study, grade I and II complications were classified as minor, while grade III, IV, and V were considered major complications. Multiple complications in individual patients were recorded as separate events.
All data were accrued and analyzed utilizing Microsoft Excel (Microsoft Corporation, Redmond, WA).
Results
From November 2006 through December 2010, 575 patients with a mean age of 60.1 years (range 43–77) underwent a RARP at our institution. Table 1 lists preoperative, intraoperative, and postoperative patient characteristics.
PSA, prostate specific antigen; ASA, American Society of Anesthesiologists.
Our mean patient body mass index (BMI) was 28.1 kg/m2 (range 19–45). The mean preoperative prostate specific antigen (PSA) and prostate volume were 5.94 cc (range 0.1–53) and 42.9 mL (range 14–175), respectively. Operative time, defined as skin incision to skin closure, was 217.2 minutes (range 109–537) and robotic console time was 173.5 minutes (range 48–480). The average length of stay was 2.12 days (range 1–23).
Of the 575 patients, 482 (83.8%) had an ideal perioperative course as previously defined. In the remaining 93 (16.2%) patients, there were 117 complications (Table 2). Upon further review 61 (52.1%) were grade I, 37 (31.6%) grade II, 7 (6.0%) grade IIIa, 8 (6.8%) grade IIIb, 2 (1.7%) grade IVa, and 2 (1.7%) grade V complications. Minor complications occurred in 84 (14.6%) patients and encompassed 83.8% of those seen in our patients. Major complications arose in 15 (2.6%) patients and accounted for 16.2% of the complications.
PE, pulmonary embolus; TIA, transient ischemic attack; ER, emergency room; UTI, urinary track infection; GI, gastrointestinal; DVT, deep vein thrombosis; PCN, percutaneous nephrostomy; SB, small bowel; SBO, small bowel obstruction; ESRD, end stage renal disease.
When the first 500 patients were divided into subsets of 100 patients, an analysis of variance demonstrated that each of the 100 patient quintiles had a similar age (p=0.52). When comparing the first four quintiles, we found that they had a similar preoperative biopsy Gleason score and PSA (p>0.05). When the last quintile was assessed, however, the preoperative biopsy Gleason score and PSA were significantly higher (Table 3).
The overall and major complication rates for the five quintiles of 100 patients are denoted in Figure 1. A linear regression analysis demonstrated no significant difference among the five quintiles (p=0.17) for overall complications. With regard to major complications, the first quintile was found to have a significantly higher major complication rate compared with the second quintile (p=0.05). The subsequent quintiles exhibited no significant change in the major complication rate. Given there were multiple surgeons who performed RARP in the study, we compared the complication rates among the three different surgeons. We found no significant difference in overall, major, or minor complications between the surgeons (data not shown).
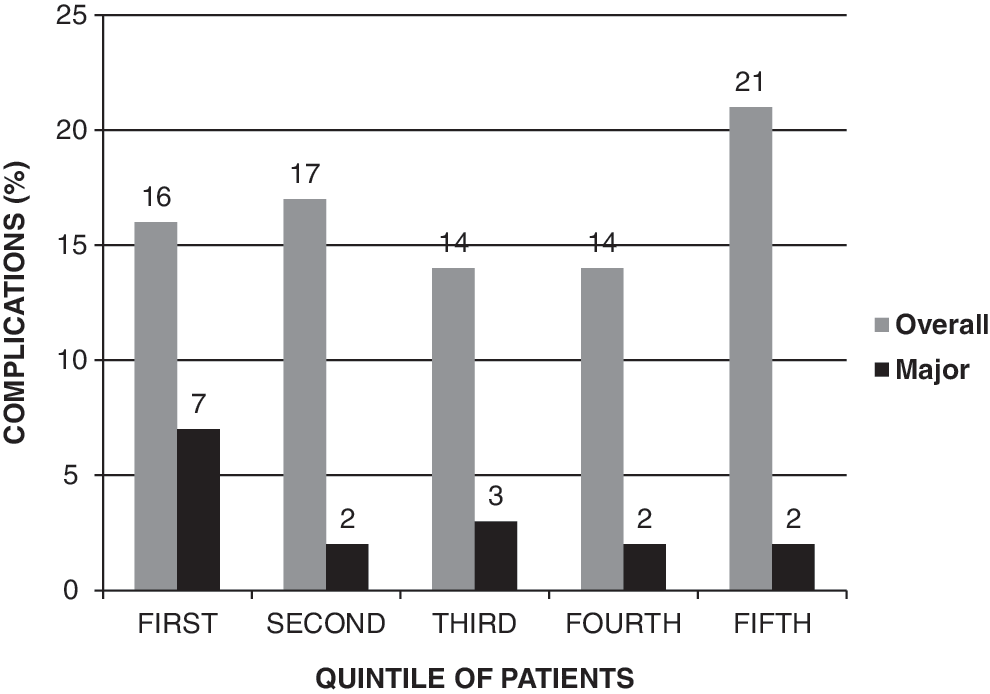
Total and major complications stratified by quintiles of patients.
Given the short follow-up period of our study, the commonly used surrogate marker for cancer control of biochemical recurrence was not available to report. Substituting for biochemical recurrence, we experienced a positive surgical margin in 114 patients (19.8%). Stratified by a pathologic grade, 55%, 31.6%, 7.9%, and 0.9% had pathologic stages T2c, T3a, T3b, and T4, respectively.
In our series, there was a single conversion to open (0.2%) that occurred early in our experience due to dense adherence of the prostate to the rectum. After conversion to an open procedure, the prostate was removed without complication.
There were two deaths (0.3%) in our series. The first was a patient that was readmitted to the hospital on POD 17 with a pulmonary embolus. Despite the initiation of appropriate and timely therapy, the patient expired. The second mortality was in a patient who was readmitted to the hospital on POD 3 with abdominal distension and pain secondary to an incarcerated ventral hernia and small bowel obstruction. The patient was brought to the operating room where the hernia was reduced and repaired without a need for bowel resection. Postoperatively, the patient was brought to the ICU, but he became hypotensive several hours after surgery and was unable to be resuscitated.
Discussion
Improving the quality of health care is an essential goal in the United States. Complete disclosure of complications is a crucial element to achieve this goal such that transparent and accurate complication reporting facilitates the physician's ability to assess his/her outcomes respective to his/her peers. 19 According to the Hawthorne effect, a critical evaluation of complications can not only promote awareness among surgeons, but also improve the surgeon's performance. 20 The importance and benefits of standardized reporting of complications thus, cannot be overstated.
Although the literature on RARP has increased considerably in recent years, series reporting complication rates are relatively limited when considering the frequency with which the procedure is performed. There remains an ill-defined and highly variable complication rate for RARP. 8 In this article, we aim to address the paucity of data reporting complications of RARP. We defined an ideal perioperative course as any patient that was discharged within 48 hours of RARP without a drain who did not have any unscheduled visits or procedures and reported any deviation from this as a complication. These complications were then stratified based on the modified Clavien classification. The implementation of a third party independent of the surgeons or house staff further assisted to remove selection bias from identification and reporting of our complications.
The overall complication rate in our series was 16.2% with a minor and major complication rate of 14.6% and 2.6%, respectively. Although difficult to compare to other series due to the variability in methodologies, these results are in line with the published literature. 3 –11 We initiated the collection of data at the beginning of our experience and, thus, we endorse these results as a true account of the perioperative complications of the procedure rather than a documentation of periods of operator excellence after the learning curve. This contrasts the reporting of Fischer et al who may have understated their complication rate of 26% because the first 240 patients undergoing RARP were not included. 3 The published literature regarding the initial series of a new surgical procedure should be interpreted with caution as many centers exclude their initial experience during the learning curve. This highlights the need for a standardization of complication reporting.
Our mean operative time was 217.2 minutes (range 109–537), which is decreased from our previous report of 231 minutes (range 125–537) 16 and reflects the evolution of operative time through the initial learning curve. A total of 16 blood transfusions were administered—2 intraoperatively (0.3%) and 14 postoperatively (2.4%). There were no specific criteria for initiating transfusions, and the majority of these transfusions occurred in the first 100 patients.
One RARP was converted to open retropubic prostatectomy (11th patient) due to dense adherence of the prostate to the rectum. Later in our series, this scenario was encountered and managed robotically on several occasions as experience was gained by the surgeon. As with any other surgical procedure, confidence in the face of difficult operative characteristics is gained progressively with increased experience.
In one patient, a small bowel injury occurred and was thought to be related to a robotic malfunction during which trocars remained in situ without pneumoperitoneum, while the robot was interrogated. This represented our only robotic malfunction during 575 RARPs, which is consistent with the reportedly low rate of robotic failures or errors. 21 Bowel injuries have previously been reported to occur during trocar insertion. Our method of gaining access involves the use of a Veress needle to establish pneumoperitoneum with subsequent placement of the 12-mm supraumbilical camera port. The remaining trocars are placed under direct vision. In patients with prior umbilical surgery, the open Hassan technique is recommended. In our experience, there have been no other trocar-related complications.
As our case volume grew, we chose to assess the trend in complication rates. To accomplish this goal, we divided the initial 500 patients into quintiles of 100 patients and assessed their overall and major complication rates. We found that over the five groups there was no significant difference in the incidence of minor complications (Fig. 1). There was a nonsignificant increase in complications in the most recent group (5th Quintile), a finding we attribute to the application of RARP to an increasingly complex patient population having higher biopsy Gleason grade and PSA values. This data are illustrated in Table 3.
When the major complications were further examined, however, we encountered a significant decrease in major complications (Fig. 1). We conclude that with strict definitions of complications and unbiased complication reporting, a robotic naïve surgeon may expect a stable minor complication rate as well as a significant drop in major complications as they progress through the learning curve.
Although the overall complication rate in our series is higher than several previous reports, the majority of our complications were considered minor, defined as a grade I or II in the modified Clavien classification (Table 2). A possible explanation of this finding is that many series are representative of high-volume centers at which surgeons are vastly experienced in robotic surgery. However, given our findings of a consistent overall complication rate, the discrepancy in complication rates may be, in part, due to a more rigorous definition and reporting of complications. For instance, a report from the Vattikuti Urology Institute referenced patients experiencing unscheduled postoperative visits that were considered nonideal postoperative courses and not complications. 9 In the present series, any aberration from the ideal postoperative course was by definition considered a complication regardless of the clinical implications.
Imperative in the report of complications is a clear definition of what constitutes an adverse outcome, yet in possibly the largest series of RARP complications, Menon et al failed to provide such a definition. 10 Of equal importance is the use of a reproducible grading system with regard to the severity of complications. Patel et al in another large RARP series did not utilize a standardized reporting system in their 1500 patients. 11 The underutilization of a uniform and standardized reporting system prohibits meaningful comparisons of surgical series.
Borrowing from the radical cystectomy literature, it has been shown that studies following the Martin criteria for complication reporting revealed a significantly higher complication rate than those that did not. 22,23 We postulate that although major complication rates may decrease with increased experience, there is a positive correlation between the quality of reporting and the overall complication rate.
Our study is limited by the short follow-up of 30 days postoperatively, the performance of RARP by three different surgeons, and the relatively small patient population. This study was not designed to assess the long-term complications of RARP, and therefore functional outcomes, including continence and potency are not reported. We felt that continence rates within 30 days of RARP were clinically insignificant, especially given the growing body of literature supporting a gradual improvement over time after surgery and catheter removal. 24 Our short follow-up is purposeful as we chose to only assess the perioperative outcomes of the procedure. Finally, the small patient population illustrates that this report represents our complete experience with robotic-assisted laparoscopic radical prostatectomy and includes our initial patient population. The inclusion of this data further assists us to accurately assess the true complication rate of RARP.
As with any other tertiary hospital, invariably some of the patients who underwent RARP at our institution were referred from out of network. However, all patients were followed postoperatively at our institution initially. We did not have research personnel contact patients to inquire about potential complications that were managed outside of our institution. Therefore, it is possible that our complication rate is a slight underestimation of the true number. This is difficult to control for and is inherent to any study of patients undergoing surgery at a large referral center.
Although difficult to stratify a cohort of patients in a multisurgeon study by quintiles, the first 100 were performed by two robotic-naïve surgeons (G.P./J.R.) and represent a true learning curve. Patients of a third surgeon were added to the study starting after 128 RARPs were performed at our institution. However, we believe this surgeon (G.H.) to have been beyond the learning curve at this point given his extensive experience with robotic surgery during fellowship training. Therefore, we feel that the quintiles are representative of a learning curve and beyond in our series of patients undergoing RARP.
Some of the strengths of our study are the elimination of possible self-underreporting and selection bias by relinquishing data acquisition to an independent blinded third party. Additionally, the strict definition of a complication adds to the validity of our results. We believe that the inclusion of all patients undergoing RARP by robotic-naïve surgeons represents a realistic and widely applicable account of RARP complications for the community urologist.
In this report, we have demonstrated that throughout the initial experience with RARP, the procedure maintains a safe overall complication rate of 16.2% and a minor complication rate of 14.6%. Additionally, as experience is gained with RARP, a surgeon can expect a drop in their major complication rate.
Conclusions
Improving the quality of health care delivery is paramount to patients and physicians in our current medical environment. At our institution, RARP is associated with an overall complication rate of 16.2%, and while minor complications may remain relatively constant, major complications decrease with increased surgical experience. Our prospective data provide one of the most comprehensive, objective, unbiased reviews of postoperative complications to date and is an important tool to set realistic expectations and accurately counsel patients.
Footnotes
Disclosure Statement
The authors have nothing to declare.