
Abstract
Background and Purpose:
Several disposable platforms have been introduced for laparoendoscopic single-site (LESS) surgery. Besides technical issues, cost is one of the main limiting factors for their widespread use. We present our experience with LESS surgery for kidney pathologies using the first completely reusable LESS platform.
Patients and Methods:
We performed LESS kidney procedures in 29 patients including nephrectomy (18), partial nephrectomy (3), pyeloplasty (4), and renal cyst ablation (4). All procedures were performed using a completely reusable single-port device (X-Cone) with a simplified combination of standard and prebent instruments. We obtained perioperative and demographic data including a visual analog pain scale (VAS); complications were recorded using Clavien grading.
Results:
Mean patient age was 49.31 years. Conversion to standard laparoscopy was necessary in one and addition of a needlescopic instrument in four cases. No open conversion was necessary. Intra- and postoperative complications occurred in two (Clavien II) cases. Mean operative time was 110, 90, and 89 minutes, and hospital stay was 4.9, 3.1, and 3.6 days for nephrectomy, partial nephrectomy, and pyeloplasty, respectively. Mean VAS was 2.13, 1.67, and 1.5 while blood loss was 81.3 mL, 140 mL, and 17.5 mL, respectively. There were no positive resection margins.
Conclusions:
LESS with a completely reusable platform is feasible for different upper urinary tract procedures yielding favorable functional and cosmetic results. A simplified combination of standard straight instruments and a single prebent grasper facilitates handling and shortens the learning curve. Reusable materials significantly reduce cost and may help to further adopt LESS surgery in surgical practice.
Introduction
One of the limiting factors inherent to LESS is the technical difficulty and a lack of reproducibility. 9 New angulated instruments have to be incorporated to provide sufficient retraction and triangulation for dissection. 10 Consequently, LESS procedures remain limited to more experienced surgeons and the learning curve is considerable. 11 Novice LESS users are frequently forced to add at least one additional trocar to complete the case successfully and safely. Most of them use needlescopic instruments, attributing to a favorable cosmetic result. 12
Most ports currently available are disposable platforms that are very cost intensive. 13 Furthermore, modified scopes and a set of specialized instruments are needed to start LESS surgery. Because the evidence for LESS surgery is quite limited and investment costs are considerable, many urologists are reluctant to set up a LESS program. 14
Reusable laparoscopic instruments have been shown to reduce per case cost dramatically. 15 The X-Cone® (Karl-Storz, Germany) is the first reusable LESS platform that allows for a simplified LESS concept based on preexisting conventional instruments and few additional tools. 16 Limited flexibility has been one of the major concerns for the use of such metal-based reusable ports. 8,16 We aimed to assess the applicability of such a platform for upper urinary tract procedures as well as complications using Clavien grading and pain scale measurements.
Patients and Methods
To date, we have performed LESS procedures for kidney pathologies in 29 patients. Institutional Review Board approval was obtained (350/2011A), and data were prospectively collected. Nephrectomy (simple and radical), partial nephrectomy, pyeloplasty, and renal cyst ablation were considered indications for a LESS approach. Exclusion criteria were body mass index (BMI) >30 and previous extensive intra-abdominal surgery as well as routine contraindications for laparoscopy (eg, pulmonary insufficiency). Demographic information, BMI, previous abdominal surgical history, surgical indication, operative time, estimated blood loss (EBL), hospital length of stay (LOS), complications, and final pathologic results were analyzed. Data were available for all variables.
Complications were classified according to the Clavien grading system 17 with Clavien grade I/II complications necessitating nonsurgical interventions deviating from typical postoperative standards, including blood transfusions. Clavien grade III complications need surgical intervention with sedation (IIIa) or general anesthesia (IIIb). Grade IV complications are life-threatening, necessitating inensive care unit management, while grade V is equivalent to patient death.
Pain assessment was conducted using an objective visual analog pain scale (VAS) ranging from 0 (no pain) to 10 (maximum pain).
Reusable platform
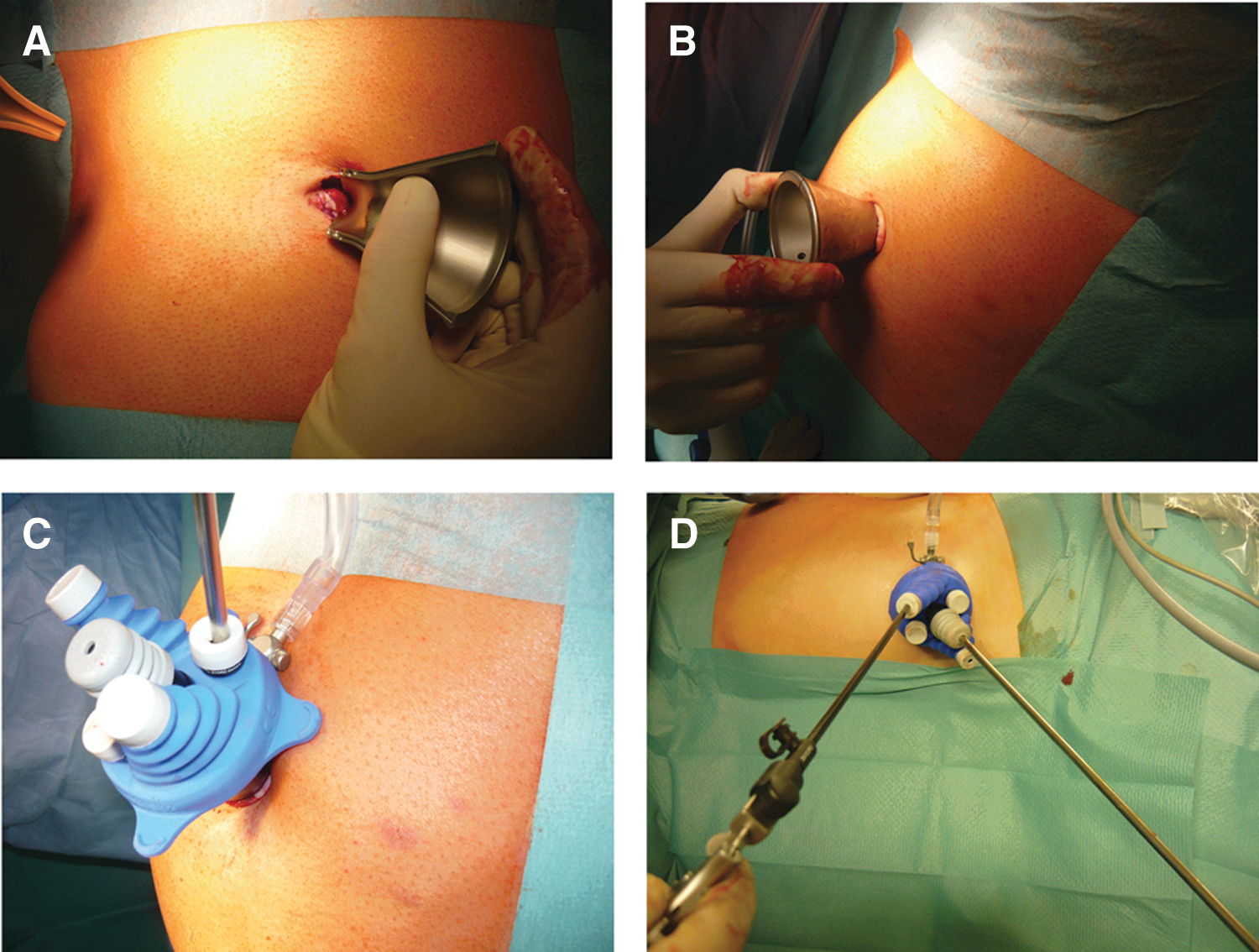
The X-Cone is a reusable access device for single-port surgery basically consisting of two self-retaining steel shells creating a funnel sealed by a silicone rubber cap (Fig. 1). The fascial opening needed to insert the port is 2.5 cm. During insertion, two-mirror L-shaped half shells are connected to each other creating an asymmetric X-shaped funnel, the larger opening extracorporeally directing to the operator side and the smaller opening lying intra-abdominally (Figs. 2 A–C). The waist of the X-Cone is placed at the abdominal wall level fixing the system. For sealing against gas loss, the top side of the funnel is covered with a silicone cap with four holes—one for gas desufflation by a curved cannula and three self-sealing openings for the telescope and operating instruments (Fig. 2 D). It is important not to use bigger incisions to avoid leakage.

Median transumbilical open access.
Assembly and use of the X-Cone:
A newly developed angulated roticulating forceps was used beside a rigid extra-long 30-degree 5-mm laparoscope (Karl Storz, Tuttlingen, Germany), a 5-mm grasper, 5-mm scissors, and a roticulating 10-mm clip-applicator (Weck Hem-o-lok®), all of which are regularly used instruments in laparoscopic surgery. The set was complemented by a 3-mm bipolar forceps, a 3-mm atraumatic grasper, and 3-mm scissors (all straight and reusable). Hemostasis and dissection was conducted using a combination instrument (Ultracison Harmonic® scalpel—Ethicon, Johnson and Johnson, or BiCision®—ERBE, Germany). All upper tract procedures were performed with the patient in a lateral decubitus position using a transumbilical access. Nephrectomy, partial nephrectomy, and dismembered pyeloplasty were performed according to the principles of standard laparoscopy. Specimens were retrieved through the umbilicus using Endo Catch™ bags. The umbilical access was closed in layers using interrupted absorbable sutures while umbilical reconstruction was achieved by subcuticular stitches (Fig. 3).

Final view after umbilical reconstruction.
Principle of dissection
In all cases, a simplified combination of one prebent grasper and one straight instrument was used. The telescope was introduced through the most dependent opening of the trocar, while 10- and 12 -mm instruments were passed through the central access. All other instruments were applied through the four openings accordingly allowing for counterintuitive movements and retraction. Importantly, dissection was always performed by the surgeon's dominant hand using the straight instrument, significantly shortening the learning curve. The extra-long roticulating curved instrument was only applied for retraction and held by the camera assistant. Because of this technical modification, there was less instrument crowding and more freedom for the operating surgeon during dissection. Additional needlescopic instruments were only inserted percutaneously when technical difficulties occurred. Any use of additional percutaneous instruments was reported separately. Data are expressed as mean±standard deviation or standard error of the mean.
Results
We performed urologic LESS procedures in 29 patients including nephrectomy (n=18), partial nephrectomy (n=3), pyeloplasty (n=4), and renal cyst ablation (n=4). Mean age was 49.31 years (9 men and 20 women), and mean BMI was 21.4 (18.1-26.2). All procedures were performed through a transumbilical access without any conversion to open surgery. Conversion to standard multiport laparoscopy was necessary in one, and addition of a single 3-mm instrument occurred in four cases. Intra- and postoperative complications occurred in two (Clavien II) and 0 cases, respectively (Table 1). Mean follow-up is 18.89 months (5–31 mos).
BMI=body mass index; VAS=visual analog scale; OR=operative; RCC=renal-cell carcinoma.
3-mm (needlescopic assistance).
Nephrectomy was performed right-sided in 7 and left-sided in 11 cases. Mean age was 49.33 years (20–83 years) and mean operative time was 110.47 minutes (60–151 min). Radical nephrectomy was performed in five cases, and negative surgical margins were achieved in all cases. EBL was 81.33 mL (20–300 ml), mean postoperative VAS score was 2.13 (1–5), and average LOS was 4.87 days (3–11 days). Postoperative prolonged ileus was noted in one patient (Clavien grade II). Conversion to multiport was necessary in one, while single-needlescopic assistance was used in two patients. In this patient, we converted to standard laparoscopy because of bleeding from the vena cava (second case of the series). Laparoscopic suturing was performed to salvage the case.
Partial nephrectomy without warm ischemia was performed in three patients (two men, 1 woman, mean age 59.67 years (46–75 years) with a mean operative time of 90 minutes (53–111), an EBL of 140 mL (20–250 mL), and VAS of 1.67 (1–3). Mean LOS was 5 days (3–7 days). All patients had negative surgical margins (pT1a, R0, renal-cell carcinoma). Prolonged ileus was observed in one patient (Clavien grade II).
Dismembered pyeloplasty was performed in four patients (two men, two women) with a mean age of 42.5 years (20–69 years). Mean Ooperative time was 89.75 minutes (66–111 min). VAS was 1.5 (1–2), and average LOS was 3.5 days (3–4 days). An additional needlescopic instrument was needed in two patients for suturing.
Renal cyst unroofing was completed in four patients (three men, one woman) with a benign history in all cases. Mean age was 48.25 years and operative time averaged 72.25 minutes (62–91 min). Mean LOS was 3.75 days (2–6 days), and VAS was 1.25 (1–2).
All patients subjectively reported a satisfactory cosmetic result of the transumbilical access.
Discussion
Since initial reports of LESS nephrectomy by Raman and coworkers 2 and Rane and Rao, 1 several investigators have demonstrated the technical feasibility of a variety of surgical procedures. These include advanced reconstructive procedures such as pyeloplasty and ileal interposition and technically challenging procedures such as radical prostatectomy, partial nephrectomy, and donor nephrectomy. 4 Consequently, multiple single-use multichannel ports and homemade devices have been developed. 18 Others advocate a single-incision multiple port access using either conventional or curved instruments in conjunction with flexible trocars. 19 Robot assistance has been introduced to further enhance surgical complexity. 20,21
The advantages of LESS are mainly related to improved cosmesis and possibly postoperative pain as well as faster convalescence. 22 Raman and associates 23 were the first to report a case-control study comparing LESS with conventional laparoscopy. They compared LESS with laparoscopic nephrectomy outcomes with the superiority of LESS over standard laparoscopy being limited to a subjective cosmetic advantage that was not specifically measured or quantified. Autorino and colleagues 24 reported that outcomes after LESS in non–high-risk patients were comparable to those of conventional laparoscopy. Tugcu and coworkers 22 compared LESS simple nephrectomy and triangular laparoscopic nephrectomy. Time to return to normal activities was reduced in the LESS group, and all the patients were pleased with their cosmetic outcome. Although some aspects have already been proven, large-scale randomized trials are still missing to ultimately determine efficacy. 24
LESS has not yet replaced standard laparoscopy, even at high-volume institutions performing the technique. 25,26 In fact, this can be considered as a consequence of a variety of limitations inherent to LESS: Technical problems because of instrument crowding and in-line vision, limited teaching facilities, and ultimately cost. 27 The latter is a particular problem whenever robot assistance is incorporated. 20 Even in the case of conventional LESS, however, cost is a major issue given that the majority of multichannel devices are intended for single use. Furthermore, most roticulating instruments are not reusable either. 28 The fact that most platforms are disposable is particularly important throughout the learning curve. In the era of cost-conscious medicine, reusable ports and instruments may help to overcome this limitation. 15
This is the first study on LESS exclusively using reusable instruments for upper urinary tract surgery. We used a completely reusable LESS-platform (X-Cone) consisting of two metal shells and a reusable silicone cap. 16 Our report details the initial series of LESS urologic procedures for upper tract procedures. Although the flexibility of the port may be inherently limited, most kidney procedures are technically feasible. Because all cases were approached through a transumbilical access, patient selection was limited to nonobese subjects. Additional needlescopic instruments were only necessary in 13.8% of the cases and conversion to triangular laparoscopy only in 3.4% while no open conversion was needed.
Complications occurred in two patients (Clavien grade II, prolonged ileus). The absence of transfusions or other perioperative complications further underlines the safety of the approach. Also, postoperative visual analog pain scale scores were low and comparable to those of other reports. 8 In all oncologic cases, negative surgical margins could be achieved. Finally, subjective cosmetic results and umbilical appearance were satisfactory in all patients.
Intraoperative ergonomy also represents a significant issue. We used a combination of one straight and one curved instrument in all cases. Importantly, only the standard instrument was used for dissection and preparation whereas the prebent grasper served only for retraction. Hence, we set up a simple set of instruments requiring only the reusable multichannel port, one curved grasper, and an extra-long telescope. All additional instruments derived from a standard laparoscopy set. With regard to cost-effectiveness, the reusable platform offers a clear advantage over a disposable port system. A financial break-even after initial purchase of the X-Cone can be achieved after fewer than four cases with the most popular LESS multichannel port systems (1130€ X-Cone vs 350€ disposable platform per use). The relatively low cost will likely reduce the threshold to using a LESS-approach because a conversion to standard laparoscopy or minilaparoscopy does not involve any additional cost.
We generally recommend, however, the liberal use of additional needlescopic instruments as necessary, especially in the case of right-sided nephrectomies. The disposition of additional instruments in complicated cases is sometimes imperative for the safe and successful completion of LESS procedures, especially in case of hemorrhage from major vessels. In particular, right-sided nephrectomies necessitate a 3-mm instrument for liver retraction. The use of additional instruments has also been proposed in the literature by other investigators, 4,7,29 whereby a meticulous selection of cases appropriate for a LESS approach is likely to reduce additional instrument use.
Conclusion
Upper urinary tract LESS procedures are feasible using a cost-effective reusable platform. With proper patient selection, complication and conversion rates are low. Subjective cosmetic outcomes are excellent; morbidity is low and at least comparable to that of standard laparoscopy. Because LESS remains technically challenging, the threshold for downgrading to minilaparoscopy should be low to guarantee patient safety. Well-designed prospective trials are still needed to ultimately assess the short-term advantages (cosmesis) and long-term oncologic outcomes of the LESS approach.
Footnotes
Disclosure Statement
No competing financial interests exist.