
Abstract
Technique for apical dissection and control of the dorsal vein complex (DVC) during robot-assisted laparoscopic radical prostatectomy (RALP) affects blood loss, apical positive margins, and recovery of urinary control. Over the past 7 years, our technique for apical dissection has been spurred by the overarching goal of minimizing injury to the rhabdosphincter to improve urinary continence, evolving from stapling to suture ligation of the DVC before bladder neck dissection to an athermal DVC division followed by selective suture ligation (DVC-SSL) before RALP anastomosis. Assessment of patient-reported quality of life outcomes demonstrates earlier recovery of continence with DVC-SSL.
Methods
Indications/contraindications
Division and selective suture ligation (SSL) of the dorsal vein complex (DVC) may be used during robot-assisted laparoscopic radical prostatectomy (RALP) in healthy men with clinically significant prostate cancer.
Preoperative workup/preparation
Candidates for RALP should have a life expectancy of at least 10 years. Guidelines indicate metastatic workup should be pursued for those with a prostate-specific antigen (PSA) level greater than 20 ng/mL and T1 disease, PSA greater than 10 ng/mL and T2 disease, a Gleason score of 8 to 10, clinical stage T3 or T4, or clinical symptoms. 1
Instrumentation
• Prograsp robotic forceps (fourth arm–medial to left anterior superior iliac spine)
• Maryland robotic bipolar dissector (left arm)
• Curved robotic monopolar scissors (right arm)
• Two large robotic needle drivers
• Polyglactin 3-0 suture
• Laparoscopic suction/irrigator
Settings
Energy: 25 W for both monopolar and bipolar currents.
Insufflation pressure and flow: 15 mm Hg and 10 L/min
Surgical Steps
A completely antegrade approach with the following sequence: Bladder neck and seminal vesicle dissection, nerve-sparing, apical dissection, and DVC-SSL before anastomosis.
Athermal division of the DVC
After performing the nerve sparing at the base and midportion of the prostate, we use the Prograsp forceps in the fourth robotic arm to bunch the detrusor apron while creating slight cephalad tension. This also allows for visualization of the anterolateral prostatic contour. After pushing levator fibers away from the prostatic apex, vascular structures between the detrusor apron and the apical prostate are divided sharply. Encountered in this region are the DVC sinuses and arterioles that course anterior to the prostatic apex. Arteriole bleeding is controlled by precise bipolar cautery. Critical to adequate visualization is maintenance of pneumoperitoneum to minimize venous bleeding. This may be accomplished with the use of the AirSeal® (SurgiQuest, Milford, CT). 2 Alternatively, the bedside assistant is instructed to use the suction sparingly, primarily with the sucker tip submerged within a puddle of blood while suctioning to prevent lowering of the pneumoperitoneum.
An anatomic plane extends sagitally from the detrusor apron's attachment to the pubic bone to the prostate-urethral junction, lying anterior to the urethra and medial to the pillars of Walsh. Identification of this avascular plane is achieved with blunt dissection after the vascular structures have been sharply divided. Once this cleavage plane is established, the ischioprostatic ligaments (Walsh pillars) are divided using circumferential sharp and blunt dissection. The exposure for the division of the remaining posterior rhabdosphincter attachments is facilitated by grasping the prostatic base with the fourth-arm Prograsp forceps and gently rotating the prostate.
Now, the anterior urethra is sharply transected. The robotic Maryland and the curved scissors are removed and replaced with needle drivers. Selective suturing of the DVC venotomies is performed using 3-0 polyglactin cut to 23 cm on a CT-3 needle (Ethicon, Somerville, NJ). Identification of the venotomies is facilitated by lowering the pneumoperitoneum by assistant suctioning the pneumoperitoneum, or setting the insufflator to <5 mm Hg. The bleeding venotomies are repaired with a mattress suture, taking thin bites of the venotomies, avoiding wider needle trajectories that may ensnare the anterior rhabdosphincter (Fig. 1). Approximately two to three venotomies are typically encountered.
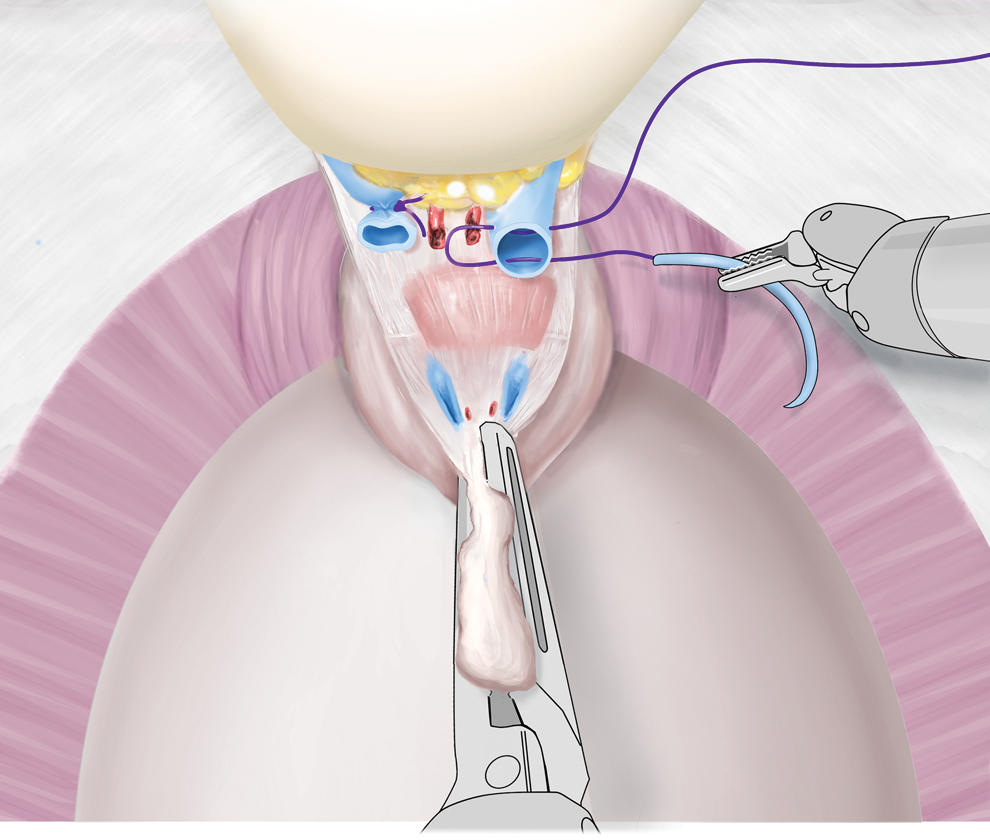
Selective suture ligation of DVC venotomies.
For efficiency, the remaining suture after SSL of the DVC is used for 50% of the urethral anastomosis. The first stitch is preplaced as a posterior anastomotic suture before division of the posterior urethra. Then, the assistant divides the posterior urethra using laparoscopic scissors. This sequence prevents retraction of the urethral stump. The prostate is then placed in the laparoscopic bag, and the anastomosis is performed.
Management of intraoperative complications
Occasionally, visualization is compromised during DVC-SSL because of pooling of venous coagulum from the cut vascular structures. Use of a powerful suction apparatus (Neptune,® Stryker, Kalamazoo, MI) that generates up to −500 mm Hg (as opposed to a traditional −80 mm Hg of wall suction) helps to maintain adequate pneumoperitoneum during sharp dissection of the DVC. This prevents clotting of the suction tip, hand piece, and/or tubing. A second suction/irrigator and tubing, however, should be readily available in the same room.
Results
In published results, men undergoing DVC-SSL experienced shorter operative times (P<0.001) than men undergoing suture ligation (SL)-DVC. While men undergoing DVC-SSL experienced greater estimated blood loss (P=0.033), there was no difference in preoperative to postoperative hematocrit change on postoperative day 1. There was no variation in apical margin positivity or overall surgical margin positivity between the two groups.
Postoperative urinary control was measured by Expanded Prostate Cancer Index Composite urinary function scores and by pad use. Urinary function and continence were better at 5 months with DVC-SSL vs SL-DVC; however, they were similar 1 year postoperatively. 2
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.