
Abstract

The National Institutes of Health urology and radiology teams have developed and implemented a similar approach over the past decade using electromagnetic tracking to register the preprocedural MRI to the real-time ultrasonography in an outpatient office-based setting to track the location of more than 11,000 biopsies in more than 600 patients, with an initial significant improvement in cancer detection rates in specific populations. 1 –3
There are several different methods for MRI + ultrasound fusion-guided prostate biopsies, including electromagnetic tracking, optical tracking, stereotactic mechanical arms, and retrospective image based registration. The emergence of multiple fusion technologies that can be deployed in an office setting could augment the “blind” or “random” transrectal ultrasonography guided prostate biopsy for patients with anterior lesions, central zone lesions (Fig. 1), previously negative biopsy in the face of a rising prostate-specific antigen level, or patients undergoing active surveillance for low Gleason score prostate cancers. 1
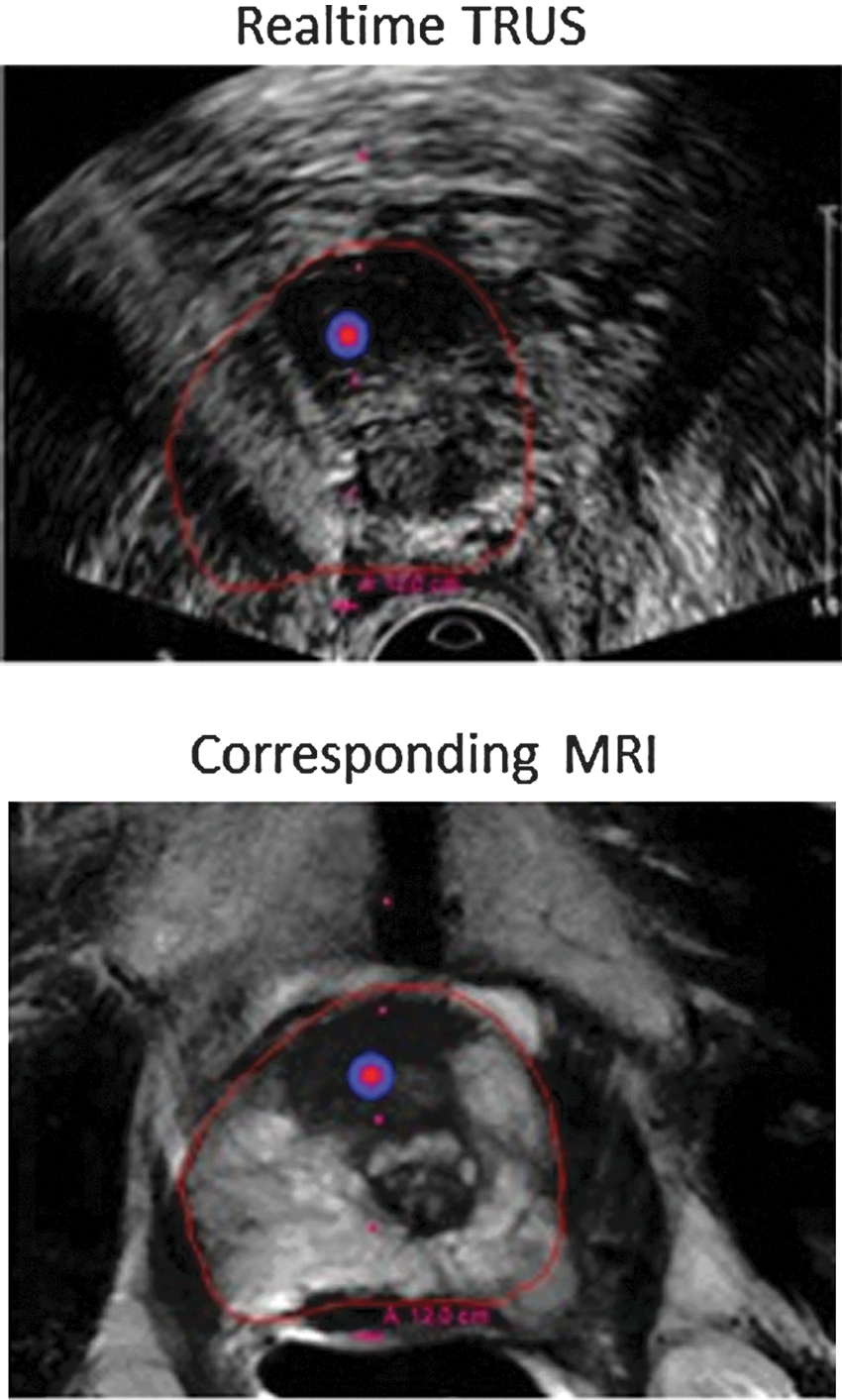
Transrectal ultrasound and corresponding preprocedural magnetic resonance imaging with anterior gland prostate cancer target (red-blue dot) in area not normally sampled by standard blind (random or sextant) biopsy.
The team from Heidelberg has shown tremendous accuracy with their system, which should translate into fertile ground for clinical impact as the MRI “ManoGram” matures and evolves for use in specific settings.
Footnotes
Acknowledgements
This work was supported in part by the Center for Interventional Oncology & the Intramural Research Program of the National Institutes of Health (NIH). NIH and Philips Healthcare have a Cooperative Research and Development Agreement. Peter Pinto, M.D., Peter Choyke, M.D., Baris Turkbey, M.D., and Sheng Xu, Ph.D., are contributing members of our prostate fusion biopsy team.
Disclosure Statement
BJW and NIH have intellectual property in the field.