
Abstract
Objective:
The aim of this meta-analysis was to evaluate the efficacy and safety of total tubeless percutaneous nephrolithotomy (PCNL) versus standard PCNL.
Method:
MEDLINE, EMBASE, the Cochrane Central Register of Controlled Trials, and the Chinese Biomedical Literature Database were researched. Randomized controlled trials (RCTs) and clinically controlled trials (CCTs) comparing total tubeless PCNL (tubeless and stentless) versus standard PCNL were included in this review. The related studies that met the inclusion criteria were included in the meta-analysis. Two reviewers independently assessed the quality of each included studies and extracted data. RevMan 5.1. was used for meta-analysis.
Outcome:
Five RCTs and four CCTs were included, involving a total of 652 patients. All patients were divided into the total tubeless PCNL group and the standard PCNL group. The pooled results showed that the total tubeless PCNL group significantly reduced the hospital stay [weighted mean difference (WMD) −1.09 (95% confidence intervals, 95% CI −1.33, −0.85)] and analgesic requirement [standardized mean difference (SMD) −0.59 (95% CI −0.96, −0.23)]. There was no statistically significant difference in the operation time [WMD −4.14 (95% CI −8.27, −0.01)], mean hemoglobin decrease [−0.07 (95% CI −0.20, 0.06)], fever [relative risk (RR) 0.53 (95% CI 0.16, 1.69)], transfusion [RR 0.86 (95% CI 0.40, 1.85)], prolonged urinary drainage [RR 0.58 (95% CI 0.08, 4.09)], and ancillary procedure [extracorporeal shockwave lithotripsy, RR 0.84 (95% CI 0.29, 2.41), second-look PCNL RR 1.18 (95% CI 0.49, 2.89)]. According to the study design, the subgroup analyses were performed; most results were consistent with the overall findings, except the one that evaluated the analgesic requirement in the CCT subgroup.
Conclusion:
Total tubeless PCNL is a safe and effective procedure. It significantly reduced the hospital stay, analgesic requirement, and the time to return to normal activity without increasing complications. However, further randomized trials are needed to confirm these findings.
Introduction
Materials and Methods
Inclusion and exclusion criteria
The selected studies were included based on the following set of inclusion criteria: (1) the included studies were randomized controlled trials (RCTs). Because of the limited number of RCTs in circulation, the decision was taken to include nonrandomized comparative studies; (2) studies were concerned about the comparison of the total tubeless and standard PCNL; (3) adult patients in the included studies were considered suitable for PCNL, no more than two percutaneous tracts, minimal bleeding at completion, and intact pelvicaliceal system; (4) the nephrostomy tract was sutured or sealed by the hemostatic sealants; (5) the baseline characteristic of patients from two groups must be matched; (6) the procedure should be under general anesthesia, spinal anesthesia, or combined spinal–epidural anesthesia; (7) each includes a trial assessed at least one of the following outcomes: operation time, hospital stay, mean hemoglobin decrease, mean analgesic requirement, return to normal activity, and major complications.
Exclusion criteria are as follows: (1) noncomparative studies were excluded; (2) the nephrostomy tube, Double-J stent, or an external ureteral catheter was placed at the completion of the procedure in the experimental group; (3) patients who were children; (4) patients were excluded from the study, if they had undergone bilateral simultaneous PCNL, complete or partial staghorn calculi, more than two nephrostomy tracts, renal anomalies, and serious urinary infection.
Literature search
We conducted a comprehensive literature strategy search to identify studies that evaluated the total tubeless versus standard PCNL from 2000 to May 2012. We searched MEDLINE (1966–May 2012), EMBASE (1980–May 2012), the Cochrane Central Register of Controlled Trials (Issue 5 of 12, May 2012), and the Chinese Biomedical Literature Database without language restriction. We also searched the reference articles of the retrieved studies. A combination of the following MeSH and key words was used: Percutaneous nephrolithotomy or nephrostomy or Percutaneous nephrostomy or nephrolithiasis or PCNL or PCN or PNL, total tubeless or tubeless, or nephrostomy free.
Data extraction and quality assessment
We screened the studies according to the inclusion and exclusion criteria. Two reviewers independently evaluated the risk of bias of the included trials with the Risk-of-bias table, which is recommended by the Cochrane handbook 5.1. It is a tool to assess the risk of bias of the included studies. It includes six domains: sequence generation, allocation concealment, blinding, incomplete outcome addressed, and other sources of bias. Each domain includes one entry in the Risk-of-bias table. Within each entry, we assigned a judgment about each methodological quality item for each included study.
The following items were extracted from each eligible study: characteristics, interventions, and outcome measures. To obtain any missing or unreported study data, we made further efforts to contact authors. Standard deviation would be calculated by review authors according to the directed algebraic relationship between p-value, standard error, and standard deviation when it is needed. In the event of duplicate publications, the studies were treated as a single source of data. Any disagreements were resolved by discussion.
Data analysis
Review Manager Software Version 5.1 was used for all analyses. For the binary data, relative risk (RR) was treated as the summary statistic; meanwhile, weighed mean difference (WMD) or standardized mean difference (SMD) was used for continuous outcomes, which accompanies with 95% confidence intervals (95% CI). The Z-test was used for overall effect of RR and WMD/SMD, and p<0.05 was considered to be statistically significant. Heterogeneity was calculated using Higgins χ 2 test and quantified by measuring I 2 . If an I 2 value is <50%, which may be considered to indicate nonsignificant heterogeneity between the randomized controlled studies, data were pooled by the fixed-effects model. The random-effects model was used in the condition that the heterogeneity was significantly presented (I 2 >50%), or the data for combining were extracted from non-RCTs. Subgroup analysis was performed according to the study design. The influence of the low-quality studies (including studies that the data calculated by reviewer) on the overall effect was detected by sensitivity analysis.
Results
Study description
A total of 829 studies were identified initially. Two reviewers (Qiang Zhong and Changjian Zheng) screened the studies according to the inclusion and exclusion criteria. After an initial screening of titles and abstracts, reviews, letters, editorials, comments, case reports, or irrelevant clinical comparative studies were excluded. Seventeen studies were thought to meet the inclusion criteria. After further reading the full text, two studies 8,9 were excluded because the ureteral catheter was removed on the postoperative day 1 or 2 for the total tubeless group; staghorn stone and renal anomalies were included in two studies 10,11 ; three studies 12 –14 were excluded because of the lack of the detailed result data or the inconsistent of the baseline. Finally, nine studies 4,15 –22 were included in this meta-analysis, including five RCTs 4,15 –18 and four case-controlled trials. 19 –22 Figure 1 shows the process of literature identification and selection flow diagram.
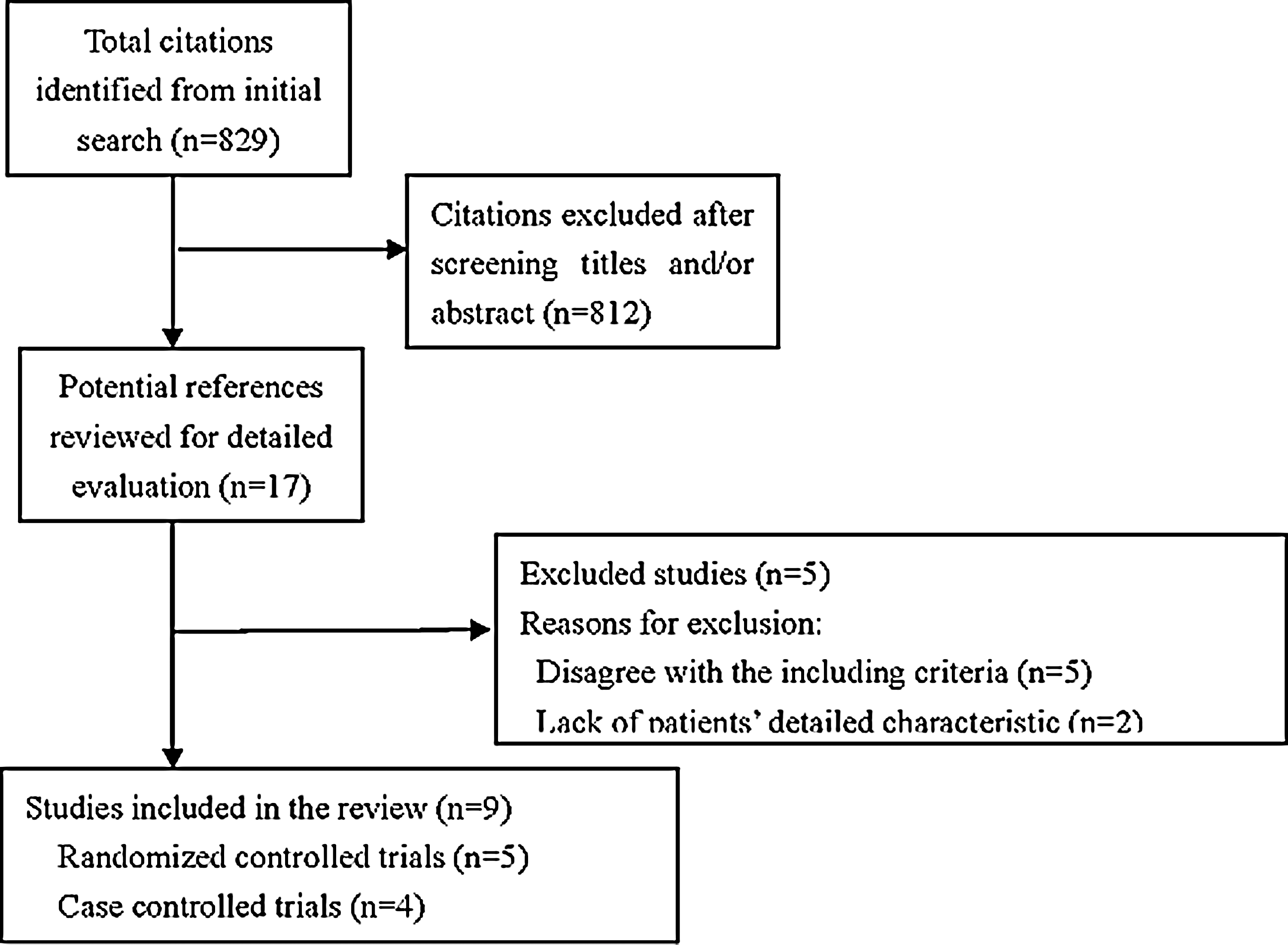
Study flow chart.
The studies' basic characteristics and outcome measures are shown in Table 1. There were 652 patients, of which 304 underwent total tubeless PCNL, and 348 underwent standard PCNL. Numbers in the respective study ranged from 20 to 135. All of the included trials were under general anesthesia. Three studies 17 –19 placed Double-J stent for the standard PCNL group besides nephrostomy tube. One study 19 did not mention the stone burden. Four studies 16,19,20,22 did not mention the stone-free rate, and two studies 17,19 did not describe the size of the nephrostomy tube. The judgments about the risk of bias for each included study are given in Figure 2.
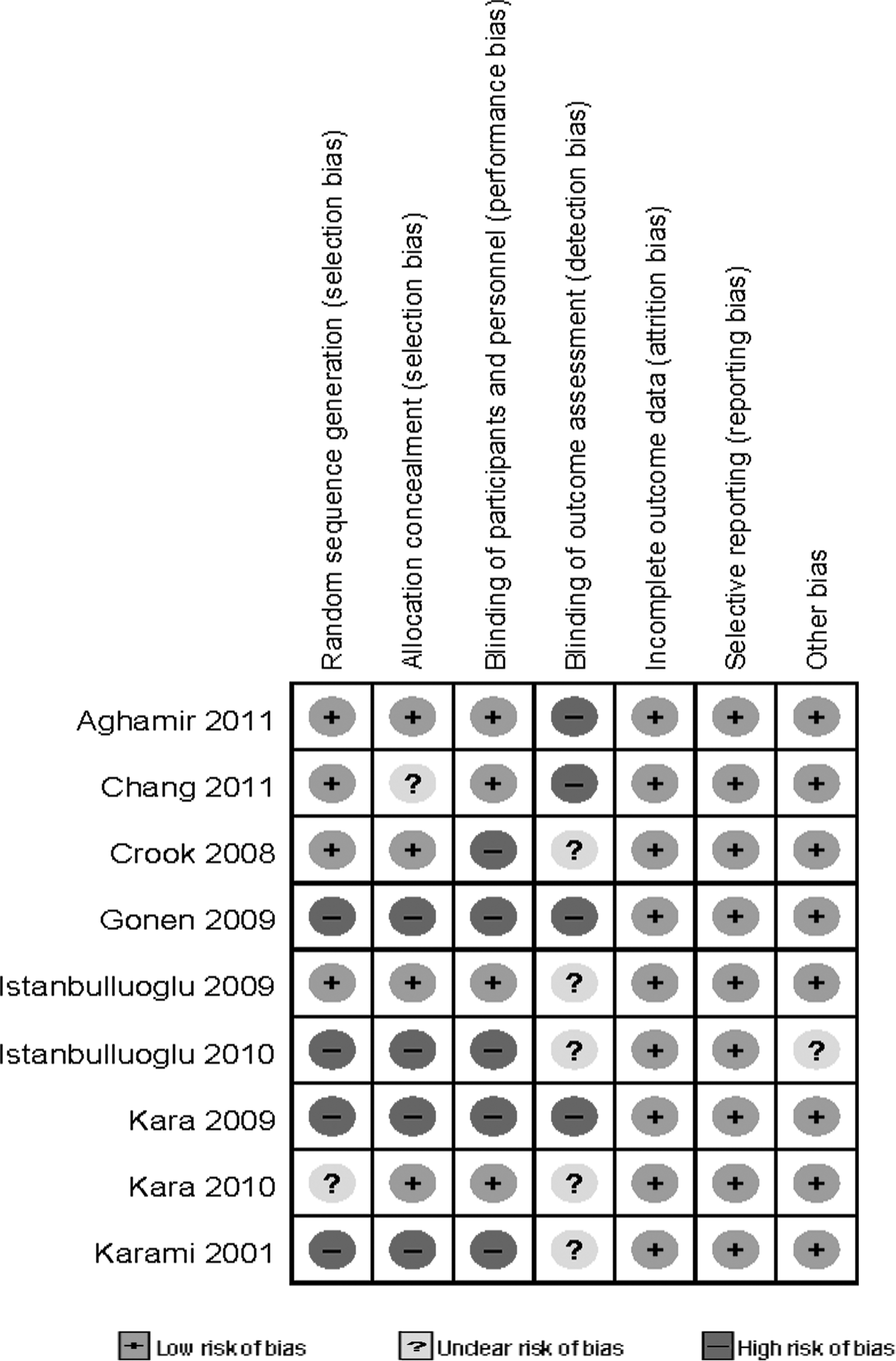
The judgments about each methodological quality for each included study.
RCT=randomized controlled trial; CCT=case controlled trial; PCNL=percutaneous nephrolithotomy; 1=operation time; 2=hospital stay; 3=mean hemoglobin decrease; 4=mean analgesic requirement; 5=return to normal activity; 6=fever; 7=transfusion; 8=pleural effusion; 9=perinephric collection; 10=prolonged urinary drainage.
Meta-analysis
Operation time
There were eight studies 15 –22 that reported the operation time, including four RCTs and four clinically controlled trails (CCTs). Because of lack of the standard deviation and the p-value, two trials 15,19 (one RCT and one CCT) were excluded from the combination of data. The pooled results indicated that the difference between two groups was insignificant, with the pooled WMD values of −4.14 (95% CI −8.27, −0.01; p=0.05) (Table 2). In a subgroup analysis, the results of the subgroup of RCTs and CCTs were consistent with the overall results, with the pooled WMD values of −6.01 (95% CI −12.91, 0.89; p=0.09) and −4.02 (95% CI −12.77, 4.73; p=0.37), respectively (Table 3).
Using WMD as the summary statistic.
Using SMD as the summary statistic.
Fixed-effects model.
CI=confidence interval; ESWL=extracorporeal shockwave lithotripsy; RR=relative risk; SMD=standardized mean difference; WMD=weighed mean difference.
Using WMD as the summary statistic.
Using SMD as the summary statistic.
Hospital stay
Eight studies, 4,15 –18,20 –22 including five RCTs 4,15 –18 and three CCTs, 20 –22 with data available for combination had reported hospital stay. The pooled result showed that the hospital stay in the total tubeless PCNL group was significantly decreased, with the pooled WMD values of −1.09 (95% CI −1.33, −0.85; p<0.00001) (Table 2). In a subgroup analysis, each subgroup results were consistent with the overall results, with the pooled WMD values of −1.17 (95% CI −1.61, −0.73; p<0.00001) and −1.04 (95% CI −1.29, −0.79; p<0.00001), respectively (Table 3).
Mean hemoglobin decrease
Three RCTs 16 –18 and two CCTs 20,22 provided available data on the assessment of the mean hemoglobin decrease for the combination. The pooled results showed that there was no significant difference between the total tubeless PCNL and standard PCNL, with the pooled WMD values of with the pooled WMD values of −0.07 (95% CI −0.20, 0.06; p=0.27) (Table 2). In a subgroup analysis, the results showed that the subgroup of RCTs and CCTs was consistent with the overall results, with the pooled WMD values of −0.07 (95% CI −0.22, 0.08; p=0.35) and −0.09 (95% CI −0.39, 0.22; p=0.58), respectively (Table 3).
Analgesic requirement
Nine studies 4,15 –22 all reported the analgesic requirement. Seven 15,16,18 –22 trials showed that the difference between the two groups was statistically significant, but the rest of two trials 4,17 showed that the difference was insignificant. Because of the different type of the anesthetic used, SMD was used for the data pooling. The overall pooled result indicated that the total tubeless PCNL group was associated with less analgesic requirement, with the pooled SMD values of −0.59 (95% CI −0.96, −0.23; P=0.001<0.05) (Table 2). Sensitivity analysis was performed by excluding one study 4 that provided the mean difference only, and the standard deviation was imputed from the p-value, and the result was still stable. Subgroup analysis was also performed, and the pooled result of the RCTs supported the overall result, with the pooled SMD values of −0.54 (95% CI −0.95, −0.13; p=0.009), but the result of the CCTs was contrary to the overall result: SMD values of −0.99 (95% CI −2.55, 0.56; p=0.21) (Table 3).
Fever
Two RCTs 15,16 and two CCTs 20,21 provided available data on the assessment of the fever rate after operation (>38°C) for the combination. The pooled result showed that the fever rate in the total tubeless and standard PCNL groups was 2.3% and 4.3%, respectively. There was no significant difference between the total tubeless PCNL and standard PCNL, with the RR values of 0.53 (95% CI 0.16, 1.69; p=0.28) (Table 2). In a subgroup analysis, the results showed that the subgroup of RCTs and CCTs was consistent with the overall results, with the pooled WMD values of 0.56 (95% CI 0.12, 2.48; p=0.44) and 0.47 (95% CI 0.08, 2.94; p=0.42), respectively (Table 3).
Transfusion
Eight studies 4,15 –21 reported the postoperative transfusion rate, including five RCTs 4,15 –18 and three CCTs. 19 –21 The pooled result showed that the transfusion rate in the total tubeless and standard PCNL group was 3.4% and 4.7%, respectively, and two groups had the similar risk for transfusion, without any significantly statistical difference, with the RR values of 0.84 (95% CI 0.37, 1.91; p=0.68) (Table 2), which showed no significant difference between the total tubeless group and the standard PCNL group. In subgroup analysis, the results were consistent with the overall results, with the pooled WMD values of 0.60 (95% CI 0.19, 1.88; p=0.38) and 1.20 (95% CI 0.37, 3.87; p=0.76), respectively (Table 3).
Return to normal activity
There were two RCTs 17,18 that reported the return to normal activity between the total tubeless and standard PCNL. Because of the significant heterogeneity (I 2 =97%), we did not pool the data. However, the time for return to normal activity in the total tubeless group was significantly lower than the standard group in both the trials.
Ancillary procedure
There were four studies 15,17 –19 that reported the requirement for ancillary procedures between the total tubeless and standard PCNL, and three RCTs 15,17,18 provided available data for pooling. As shown in Table 2, the pooled result showed that the extracorporeal shockwave lithotripsy (ESWL) rate in the total tubeless and standard PCNL group was 3.7% and 4.4%, respectively, and this difference was indistinctive ([RR 0.84, 95% CI 0.29, 2.41; p=0.74). The result also indicated that the incidence of second-look PCNL in the total tubeless and standard PCNL group was 6.1% and 5.1%, respectively, without any significant statistical difference (RR 1.18, 95% CI 0.49, 2.89; p=0.71).
Prolonged drainage and perinephric collection
There were two RCTs 15,16 and one CCT 20 that reported the prolonged urinary drainage between the total tubeless and standard PCNL. The reason for it was the analgesic-resistant pain or renal colic. The pooled result indicated that the incidence of prolonged urinary drainage in the total tubeless and standard PCNL group was 2.5% and 4.8%, respectively, without any significant statistical difference (RR 0.58, 95% CI 0.08, 4.09; p=0.59). Two studies 15,19 reported two patients who suffered the perinephric collection. One patient was in the total tubeless group, 15 and the other one was in the standard group. 19
Discussion
The placement of a nephrostomy tube is considered to be a safety option at the completion of PCNL. It has some advantages, including draining the kidney, avoiding urine extravasation, plugging the access, and facilitating a secondary nephrostomy procedure required. However, the prolonged hospital stay and significant postoperative pain derived the urologist to improve this procedure. Bellman et al 1 in 1997 first reported the tubeless PCNL. Because of the success in reducing the hospital stay, analgesic requirement, and the cost, this new technique gained popularity. However, the tubeless with a urethral stent was associated with the stent-related discomforts and the need to remove the Double-J stent through postoperative cystoscopy. In recent years, many investigators reported that the tubeless and stentless PCNL in selected patients was safety, which can reduce the hospital stay and analgesic requirement. In our review, the meta-analysis got the similar conclusion. The hospital stay, analgesic requirement, and the time to return to normal activity in the tubeless and stentless group were decreased significantly, without increasing the complications.
Analgesic requirement is an important indicator to evaluate the postoperative pain. In our review, the pooled results show that the analgesic requirement was decreased significantly in the totally tubeless group. Some studies 8,23 noted that the placement of the nephrostomy tube was an important source of the postoperative pain, and this may explain the reason for diminished analgesic requirement in the experimental group. The analgesic requirement was associated with the tube size closely. 23 According to the previously published series, the tubeless PCNL was associated with less analgesic requirement compared to standard or large-bore PCNL. Likewise, the small-bore PCNL can also decrease the analgesic requirement versus standard or large-bore PCNL, which was confirmed by two prospective randomized studies. 24,25 However, whether the tubeless PCNL was associated with less analgesic requirement compared to small-bore PCNL is still controversial. Some investigators 24,26 reported that there was no significant difference between the tubeless and small-bore PCNL. On the contrary, Shah and his coworkers 27 reported that tubeless PCNL decreased the analgesic requirement, and this difference was statistically significant.
In our review, we found that the difference between the experimental and control group on the stone-free rate was not so much dramatic in the respective included trial; furthermore, only one trial 21 reported that the stone-free rate was 100%. Although the implement of the tubeless and stentless PCNL was confined in the smaller stone burden and uncomplicated procedure, we sometimes may not make certain that there was no residual stone existed at the end of the procedure. When a secondary procedure for removal of residual stones is planned, the pre-existing tract may not provide good access to reach the stone. In most cases, generating a new access tract may be inevitable. 15 Although only 10 of 163 patients performed the second-look PCNL in the total tubeless group, the second procedure inevitably increased patient morbidity. Hence, the rigorous examination during the procedure was necessary. Portis et al 28 reported that the high-magnification rotational fluoroscopy can make the accuracy of intraoperative detection of residual fragments reach 76%, 76%, and 96% at the 0-, 2-, and 4-mm success thresholds, respectively. Meanwhile, the flexible nephroscope was a good auxiliary for the rigid instruments to exam each calyx and remove the residual fragments with a basket or grasping forceps or manipulate into the renal pelvis with irrigation or a guidewire. 29 In addition, with the advent of new-generation flexible ureteroscopes with greater deflection and control, there has been an increase in endoscopic ureteroscopy and laser lithotripsy for renal calculi. 30 Flexible ureteroscopes seemed as the alternative therapy for medium-size renal stone with acceptable efficacy and low morbidity. 31 Breda et al 32 reported that the stone-free rate was 100% for the stone burden <20 mm. These suggested that the flexible ureteroscope maybe a better option to be used as remedial treatment for the residual stone after the tubeless and stentless procedure compared with the second PCNL.
The main reason for endourologists to continue to favor nephrostomy tube placement is probably the fear of bleeding or urinary leakage from a tract left open. 1 However, for patients who had been selected for tubeless and stentless procedure, minimal bleeding was one of the primary premise conditions. To ensure no visible bleeding, the surgeon has better to wait for 5 minutes after the termination of the procedure and observe for any gross tract hemorrhage. 33 For the urinary leakage speaking, no included trial reported the occurrence of the urinary leakage. In our review, the trials underwent uncomplicated procedure, which was considered to be enough for the ureter to provide adequate drainage without stenting for the selected patients. 22 In recent years, the hemostatic agents, mainly including gelatin matrix hemostatic sealant, fibrin glue, and oxidized cellulose, were used to seal the nephrostomy tract to reduce the complication of bleeding and urinary leakage. As Bellman said, 7 the hemostatic agents were more likely used in those patients who had persistent bleeding even after pressure was applied to the flank. Therefore, as for the tubeless and stentless procedure, the hemostatic agents may be avoided, at least not a routine manner. 33 Our meta-analysis showed that the hospital stay and the time for return to the normal activity were decreased significantly in the experimental group. These may be contributed to not only the less pain and the tubeless procedure, but also the absence of the stent, which was associated with the stent-related complications and the pain caused by postoperative cystoscopy.
As Srinivasan et al 34 said, the most important factors to govern the technique for drainage were the operative course, procedural complexity, stone burden, and the clinical status of the patient. The patients for the tubeless and stentless procedure should be selected rigorously, even stricter than tubeless PCNL with stent. Our selection criterion is minimal bleeding, no residual stone, intact pelvicaliceal system, less than two percutaneous tracts, no large stone burden. If the patients meet these conditions at the end of the procedure, neither a nephrostomy tube nor a stent will be left in the patient. However, although the improvement of the lithotripsy and the endoscopic technique made it possible to develop the tubeless procedure for selected patients, it is not enough to make the tubeless PCNL to become the universal current standard of care. In the case of the doubtful stone clearance or bleeding, it is safer to leave a tube or stent.
This study has some limitations. First, the included trials were all small sample size; secondly, because of the enrolling of the non-RCTs and the limitations in the design and implementation of the RCTs, it is likely to result in a biased assessment; third, the heterogeneity was significantly presented when pooling the data of the operation time and analgesic requirement, and it cannot readily be interpreted; the pooled results' value may be limited. Large RCTs with a rigorous methodology are recommended.
Conclusion
Total tubeless PCNL is a safe and effective procedure for selected patients. It significantly reduced the hospital stay, analgesic requirement, and the time for return to normal activity without increasing complications. However, further randomized trials are needed to confirm these findings.
Footnotes
Disclosure Statement
No competing financial interests exist.