
Abstract
Background and Purpose:
The treatment of symptomatic lower pole (LP) calculi poses a challenge because of lower clearance rates. We present our experience with microperc in the treatment of LP renal calculi.
Patients and Methods:
We retrospectively evaluated the symptomatic patients with LP renal calculi who underwent microperc between August 2011 and June 2012 from two referral hospitals. Patients were included only in cases of failure after shockwave lithotripsy (SWL) or retrograde intrarenal surgery (RIRS) and according to patient preference. The percutaneous renal access was performed using the 4.8F “all-seeing needle” with C-arm fluoroscopy or ultrasonographic guidance with the patient in the prone position. Stone disintegration was established using a 200 μm holmium:yttrium-aluminum-garnet laser fiber.
Results:
A total of 21 patients (mean age 37.3±20.1 years) with LP stone underwent microperc. The mean body mass index was 28.6±6.0 kg/m2, and the mean stone size was 17.8±5.9 (9–29) mm. The duration of surgery and fluoroscopic screening was 62.8±25.2 minutes and 150.5±92.8 seconds, respectively. The patients were discharged after a mean 37.5±14.4 hours of hospitalization time. The mean hemoglobin drop was 0.8±0.6 (0.1–2.3) g/dL. Conversion to miniperc was necessitated in one patient with loss of vision. Stone-free status was achieved in 18 (85.7%) patients. Clinically insignificant residual fragments were observed in only one (4.8%). The procedure failed in two (9.5%) patients. A total of two minor complications (renal colic necessitating stent insertion and urinary tract infection) were observed postoperatively, none severe.
Conclusion:
Microperc is a feasible and efficient treatment modality for symptomatic LP calculi. Our results provide that microperc might take a part in case of SWL and RIRS failures or as an alternative to percutaneous nephrolithotomy or RIRS in the management of symptomatic LP calculi.
Introduction
On the other hand, the location of the stone and pelvicaliceal system anatomy are the other factors affecting the selection of the appropriate treatment regimen. Hence, the management of symptomatic lower pole (LP) calculi poses a challenge because of lower clearance rate compared with the pelvis and other caliceal stones. 2,3 Although the noninvasive nature, minimal anesthesia requirement, and high acceptance rate by patients and physicians are main advantages of SWL, low stone-free and higher re-treatment rates are considered as drawbacks. 2 –6 RIRS has been popularized with the advances in endoscope and lithotripter technology. The collecting system anatomy, however, restricts its success rate especially for LP stones. 7,8 The studies comparing the outcomes of therapeutic methods have shown that PCNL is most invasive endourologic modality with the highest stone-free rate. 4,9
Microperc is a recently introduced and less invasive form of standard PCNL that provides safe and single step percutaneous renal access under direct vision, stone disintegration with a holmium:yttrium-aluminum-garnet (YAG) laser via a 4.8F access sheath, and clearance of stone debris with its own irrigation system. 10,11 We present our experience with microperc in the treatment of patients with LP renal calculi.
Patients and Methods
We retrospectively evaluated symptomatic patients with LP renal calculi who underwent microperc by experienced urologists (AT, AA, AAS) in PCNL between August 2011 and June 2012 from two referral hospitals in Turkey. All of the symptomatic patients with LP calculi <1 cm were primarily referred for SWL. With failure of SWL, microperc was used as an alternative treatment modality. For patients with an LP stone larger than 1 cm, microperc was primarily performed according to patient preference or in case of RIRS failure. Preoperative patient- and stone-related parameters and outcomes were prospectively recorded in the patient entry system. Before surgery, patients assigned informed consent.
All patients underwent routine biochemical and radiologic evaluation before surgery. The patients with positive urine culture results were treated with appropriate antibiotics preoperatively. The stone size and location were assessed by intravenous urography and/or CT.
Operative technique
Initially, a 6F open end ureteral catheter was inserted in all patients who were in the lithotomy position under general anesthesia. Then the patient was turned to the prone position, and all pressure points were padded. The percutaneous renal access to the posterior caliceal fornix was performed using the 4.8F “all-seeing needle” (PolyDiagnost, Pfaffenhofen, Germany) with C-arm fluoroscopy or ultrasonograpic guidance as described previously. 10,11 The all-seeing needle is composed mainly of 0.9 mm microoptic inner and outer puncture shafts (Fig. 1). After visualization of the collecting system and positioning the stone, the inner shaft was taken out. A three-way connector allowing the insertion of optic, laser fiber, and irrigation system was attached to the outer tip of the shaft (Fig. 2). The stone disintegration was established using a 200 μm holmium:YAG laser fiber with the settings of 0.8 J at 8 Hz (6.4 W) (Fig. 3). The irrigation pump system controlled by the surgeon with a foot pedal aids the maintenance of vision and removal of the stone debris during surgery. In addition, the pressurized irrigation system of microperc facilitates the flush out of the stone fragments by the inner or outside of the catheter through the ureter.

The 0.9-mm microfiber optic, 16 gauge needle, and 8F microsheath.

The small skin incison and the set of microperc is shown.

Stone disintegration with laser fiber.
The drainage of irrigation fluid from collecting system through the 6F open-end ureteral catheter was controlled during the surgery. In the presence of blockage of fluid passage from the catheter because of clogging by the stone debris or fragments, the clogging was dissolved by pressurized irrigation from the distal tip of the catheter. Stone clearance was evaluated with C-arm fluoroscopy and visual control with microoptic. In patients with LP calculi >2 cm, the stone disintegration was performed through the 8F microsheath that allows better manipulation, use of 360 μ laser fiber, and Double-J stent placement by the antegrade route.
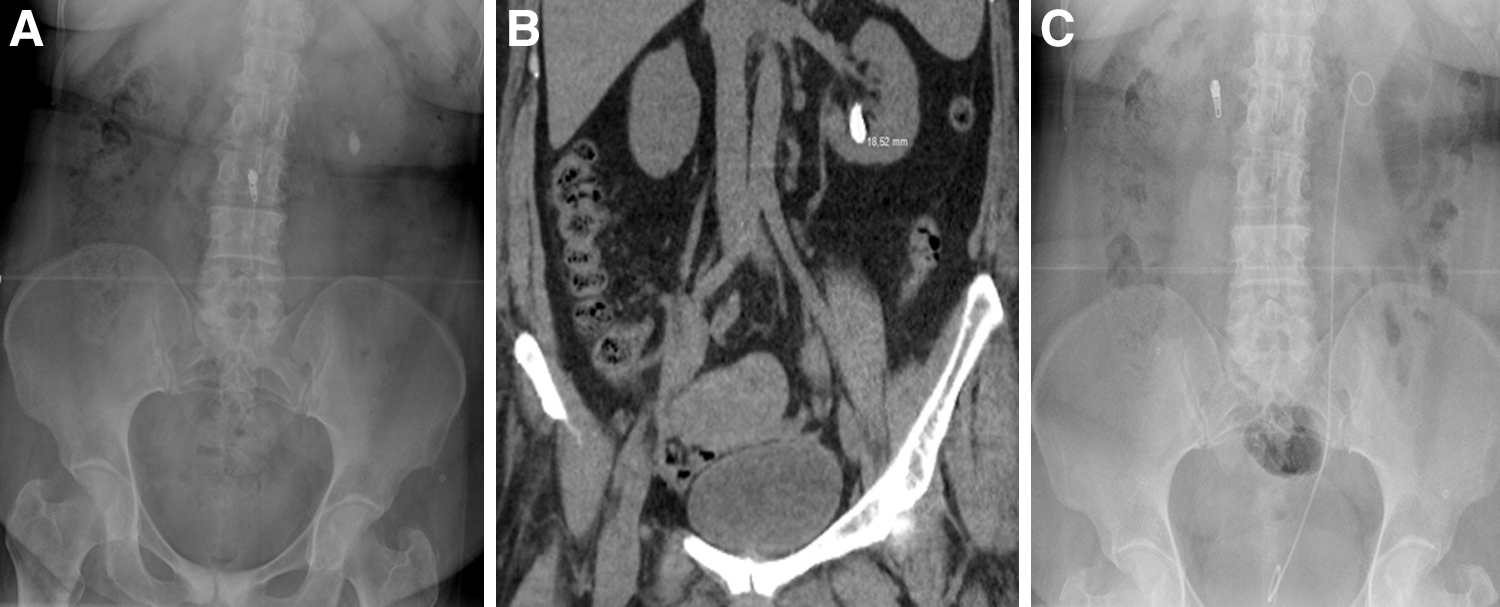
The patients were routinely discharged after removal of the urethral and ureteral catheter and radiologic assessment with views of the kidneys, ureters, and bladder on postoperative day 1 (Fig. 4). Success was defined as no residual fragment on CT at the first month of follow-up. Clinically insignificant residual fragments (CIRF) were defined as asymptomatic fragments ≤4 mm. 12 The postoperative complications were classified using the Clavien grading system. 13
Preoperative
Results
A total of 21 patients with LP stone underwent microperc. Pain was the predominant symptom of the patients. The mean age was 37.3±20.1 (7–69) years. Male/female distribution was 10/11. The mean body mass index was calculated as 28.6±6.0 (13.2–39.0) kg/m2. The mean stone size was measured as 17.8±5.9 (9–29) mm. The failure of SWL and RIRS was the indication for microperc in five and two patients, respectively. The demographic values are summarized in Table 1.
SD=standard deviation; BMI=body mass index; SWL=shockwave lithotripsy; RIRS=retrograde intrarenal surgery.
The duration of surgery and fluoroscopic screening was 62.8±25.2 (30–100) minutes and 150.5±92.8 (20–320) seconds, respectively. The patients were discharged after a mean 37.5±14.4 (14–76) hours of hospitalization time. The mean hemoglobin drop was 0.8±0.6 (0.1–2.3) g/dL. Conversion to mini-PCNL was necessitated in a patient with minimal bleeding causing loss of vision.
Stone-free status was achieved in 18 (85.7%) patients. CIRF was observed in only one (4.8%) patient with scoliosis and steep infundibulopelvic angle. The procedure failed in two (9.5%) patients. The failure of the procedure originated from the pushback of the fragment to the other calices that could not be reached by the rigid and fine microperc sheath.
A total of two complications were observed in the postoperative period. Ureteral stent insertion was necessitated in a patient with renal colic resistant to medical treatment (Clavien grade IIIb complication). 13 Urinary tract infection was controlled with antibiotics in the other patient (Clavien II complication). 13 No major complication was observed. The perioperative parameters are listed in Table 2.
Discussion
The management of symptomatic LP calculi is a problematic issue; mainly, all treatment modalities, such as SWL, RIRS, and PCNL ranging from noninvasive to invasive, can be used according to the stone size and anatomic factors. Many researchers have performed comparative studies to determine the appropriate treatment modality with the highest stone-free and less morbidity rates for LP calculi. 4,6,9 The recent technologic advances, especially in optical and lithotripter systems, have presented a promising future for dealing with this problem. In this study, we aimed to elucidate the role of microperc as a least invasive form of PCNL in the management of LP stones.
Because of its noninvasive nature, SWL has been accepted as a first-line treatment modality for patients with renal calculi up to 2 cm in diameter. Studies have shown, however, that success rates of SWL are influenced by patient- and stone-related factors including stone size, location, and composition, pelvicaliceal system anatomy, and skin-to-stone distance (SSD). 2 –6,14 –16 The studies clearly demonstrated that stone-free rates are inversely correlated with stone size. 17 In particular, calcium oxalate monohydrate, brushite, and cysteine stones are more resistant to SWL than others. 18,19 The superiorities of microperc to SWL are that stone disintegration is performed using the laser under direct vision independent of stone composition and density and SSD. 11 Although the lack of information on stone density and composition and SSD are considered as limitation factors in the present study, we did not encounter any problem related to these factors during microperc.
The success of the treatment modality is related to clearance of the stone fragments as well as stone disintegration. Although the adequate fragmentation of the stone is achieved in most of the patients by SWL, the clearance of the stone fragments is limited because of the anatomic factors of the lower calix listed as: Steep infundibulopelvic angle, length of LP infundibulum (>10 mm), and infundibular width (<5 mm). 1,20 –22 Thus, the recent EAU guidelines recommend the use of SWL for 1 to 2 cm LP calculi in the presence of these unfavorable factors. To improve the clearance rate, different treatment strategies such as mechanical percussion, patient inversion, urinary diuresis, and antegrade or retrograde irrigation methods are described in the literature. 23 –25
In the present study, five patients had a history of SWL failure. In two of these patients, stone fragmentation was accomplished, but clearance did not occur in a 3-month follow-up period. Although there is no capability of stone fragment retrieval via the 4.8F sheath during microperc, the clearance of stone debris or particles formed by laser fragmentation is obtained by a pressurized irrigation system. In the present study, stone-free status was achieved in 18 (85.7%) patients. CIRF was observed in one (4.8%) patient with scoliosis and asteep infundibulopelvic angle.
The major superiority of SWL to microperc is the feasibility with sedoanalgesia. SWL, however, is generally performed with the patient under general anesthesia in younger children, similar to microperc. The requirement of general anesthesia, however, can be accepted as an important limitation, if we consider the higher additional treatment rate of SWL compared with PCNL. 4,6,26 In the present study, six symptomatic pediatric patients with LP stone aged ≤16 years were treated with a single session microperc. No additional treatment was needed for these patients.
In recent years with the introduction of new generation flexible ureteroscopes with higher deflexion capabilities and small size and the advances in laser lithotripsy technology, the indications for ureteroscopy (URS) have been expanded, and URS has been accepted as an alternative treatment modality with lower morbidity than PCNL and higher stone-free rate than SWL. The studies analyzing URS for LP stones reported success rates of2 60% to 89%. 2,8,9,27,28 Although 7% of the LP stones were found to be inaccessible among 1000 cases of a URS series, Resorlu and associates 7 found that the stone length and infundibulo-pelvic angle affects the stone free rate after URS. 8 PCNL is an alternative modality for inaccessible calices with URS. Microperc provides safe access and stone fragmentation under direct vision. In the present study, microperc was successfully performed in two patients in whom RIRS failed because of a steep infundibulopelvic angle.
The retrieval devices allow the repositioning of the stone to a more accessible calix and contribute to the success rate of URS. 27 Thus, the cost of the procedure increases because of the usage of the baskets, retrieval devices, and access sheaths. Microperc seems to be more cost-effective because of its noninstrument dependent application. There is no study, however, that compares the cost-effectiveness of microperc and flexible URS.
The Lower Pole Study Group prospectively compared the outcomes of URS and SWL in patients with stones ≤1 cm, and PCNL and URS in patients with stones between 1 and 2.5 cm. 6,29 No statistical difference was detected between URS and SWL in terms of stone-free, complication, and additional treatment rates, and duration of hospitalization for LP stones ≤1 cm. In another study, 28 URS was found to be associated with higher stone-free and lower re-treatment rates compared with SWL for LP stones of 10 to 20 mm. The studies that compared PCNL and URS clearly revealed higher stone-free rates for PCNL. 9,29
The main difference between URS and PNL is the access route. URS is an endoluminal procedure performed through the natural orifices. PCNL is an invasive procedure that is performed through a gate (access) from the skin to the renal collecting system. The URS procedure is associated with fewer complication rates compared with PCNL. Flexible URS is regarded as a safe treatment modality because of its endoluminal nature for patients receivinging anticoagulant agents in whom PCNL is contraindicated. 30 On the other hand, while the risk of ureteral injury has been minimized with the decrease in instrument size, PCNL or microperc does not carry such a risk.
The studies mentioned above have clearly demonstrated that PCNL is associated with higher success and complication rates and morbidity than SWL and URS. 4 –6 The complications often occur during access creation, dilation, or stone fragmentation phases of the procedure with a wide range between 29% and 83%. 31 –33 To decrease the morbidity and complication rate of PCNL, smaller size nephroscopes have been used by investigators. 34 –38 Microperc provides the smallest single step renal tract that allows confirmation of a safety access by the all-seeing needle and stone disintegration. 10,11 The technique was initially performed by Desai and colleagues 11 in 10 patients with renal calculi with a mean size of 14.3±6.3 mm. Among them, the stone was located in the lower pole in four patients. The mean hemoglobin drop was reported as 1.4±1.0 g/dL. Although this was the first study that reported the applicability and results of microperc, our study is the first study focusing on the role of microperc in the management of LP renal calculi that is accepted as a controversy. In the present study, the mean hemoglobin drop was found to be 0.8±0.6 g/dL. No major complication was observed.
Concerning the limitations, the retrospective nature and small number of the cases presented in the study constitute the main concerns. We believe that despite the limitations, the present study will contribute to the literature. Prospective randomized comparative studies, however, are needed before making a consensus about which treatment modality is more effective and less invasive.
Conclusion
Our results show that microperc might take a part in case of SWL and RIRS failures or as an alternative to PCNL or RIRS in the management of symptomatic LP calculi. Microperc is a feasible and efficient treatment modality for symptomatic LP calculi. This is the first study of microperc that focuses on the role of managing LP calculi, which is a challenging location.
Footnotes
Disclosure Statement
No competing financial interests exist.