
Abstract
Purpose:
To compare color Doppler twinkling artifact and B-mode ultrasonography in detecting kidney stones.
Patients and Methods:
Nine patients with recent CT scans prospectively underwent B-mode and twinkling artifact color Doppler ultrasonography on a commercial ultrasound machine. Video segments of the upper pole, interpolar area, and lower pole were created, randomized, and independently reviewed by three radiologists. Receiver operator characteristics were determined.
Results:
There were 32 stones in 18 kidneys with a mean stone size of 8.9±7.5 mm. B-mode ultrasonography had 71% sensitivity, 48% specificity, 52% positive predictive value, and 68% negative predictive value, while twinkling artifact Doppler ultrasonography had 56% sensitivity, 74% specificity, 62% positive predictive value, and 68% negative predictive value.
Conclusions:
When used alone, B-mode is more sensitive, but twinkling artifact is more specific in detecting kidney stones. This information may help users employ twinkling and B-mode to identify stones and developers to improve signal processing to harness the fundamental acoustic differences to ultimately improve stone detection.
Introduction
B-mode diagnostic ultrasonography is an alternative to CT without ionizing radiation; however, its adoption has been hindered by lower sensitivity (19%–93%) and specificity (84%–100%) for the detection of urinary calculi. 4 –17 Ultrasonography is also critically dependent on the sonographer. 18 Improvements in ultrasound hardware and signal processing might lead to better stone detection and increased use of this modality.
A twinkling artifact associated with color Doppler ultrasonography of urinary calculi has been described as a rapidly changing mixture of red and blue seen on or behind the stone where the shadowing would be expected on B-mode imaging. 19 The etiology of the artifact is not completely understood, but it has been hypothesized to be from phase or clock jitter, and stone surface roughness. 19,20 More recent data suggest that twinkling may arise from tiny gas pockets on the stone surface. 21 Several studies have demonstrated the dependence of the twinkling artifact on ultrasound machine settings and stone composition. 20,22 –26 The twinkling artifact has been observed in 83% to 96% of stones seen on B-mode ultrasonography. 22 –24,26 –29
All previous studies comparing CT scan, twinkling artifact, and B-mode ultrasonography have performed the twinkling evaluation after a complete B-mode ultrasonography. To our knowledge, there have been no studies separating the B-mode portion of the examination to test the independent performance of the twinkling artifact alone in the evaluation of urinary tract calculi. The purpose of this study was to compare the independent characteristics of twinkling artifact and B-mode ultrasonography in the detection of renal stones. The ultimate goal is development of a new ultrasound mode to make detection of stones easier and more accurate.
Patients and Methods
Nine subjects with varying degrees of kidney stone burden detected by recent CT scan volunteered to participate in our study over a 6-month period. Subjects prospectively underwent bilateral renal ultrasonography by a single ultrasonographer blinded to the CT scan results, using a commercial ultrasound machine (Philips/ATL HDI 5000 with a P4-2 ultrasound transducer). The entire ultrasound session was recorded using traditional B-mode ultrasound and with color Doppler ultrasound to evaluate for twinkling. For both ultrasound methods, the machine settings were not restricted or fixed, and the sonographer was allowed to optimize the commercial ultrasound system settings in an attempt to improve resolution.
The entire video session was edited into short separate segments demonstrating twinkling and B-mode ultrasonography of the upper pole, interpolar area, and lower pole of each kidney, thus creating 12 short video segments for each subject. The 108 video segments were randomized using a random number generator and then independently reviewed by three experienced radiologists. After viewing a short training video that defined the scoring procedure, each radiologist independently reviewed the randomized video segments and scored whether they believed a stone was or was not present. Their responses were compared with the subject's recent CT scan. The average time between the CT scan and the ultrasound examinations was 41 days (range 0–99 days). In all cases, there were no interval stone events, episodes of symptomatic acute renal colic, or witnessed passage of stones or stone fragments. In cases with more than 30 days between the CT scan and ultrasound examination (n=4), a separate interval imaging study (plain film radiography of the kidneys, ureters, and bladder or renal ultrasonography) confirmed no change in stone burden or stone location.
The primary outcomes of interest were the receiver operator characteristics (ROC) for both twinkling artifact and B-mode ultrasonograpphy including sensitivity, specificity, positive and negative predictive value, percent correctly classified, and the area under the ROC curve. Results were stratified by stone size (<5 mm, 5–10 mm, >10 mm) and by radiologist. In cases where multiple stones were located within the same area of the kidney, the stone was stratified by the largest stone. Subgroup analyses were performed of patients with multiple stones in the same area of the kidney. All t tests were two tailed with statistical significance set at P<0.05.
This study received approval (#35261) from the University of Washington Institutional Review Board, and informed consent was obtained from all subjects.
Results
Mean subject age was 47±15 years, 44% were women, and mean body mass index was 26±6 kg/m2. There were 32 stones in the 18 kidneys with a mean stone size of 8.9±7.5 mm (Table 1). The area under the ROC curve for B-mode ultrasonography was 0.594 and for twinkling artifact ultrasound was 0.647 with no difference between methods (P=0.33) (Fig. 1). B-mode ultrasound had a sensitivity of 71%, specificity of 48%, positive predictive value of 52%, negative predictive value of 68%, and 58% of the video segments were correctly classified as either having or not having a stone as determined by the CT scan (Table 2). Twinkling artifact ultrasound had a sensitivity of 56%, specificity of 74%, positive predictive value of 62%, negative predictive value of 68%, and 66% of the video segments were correctly classified.
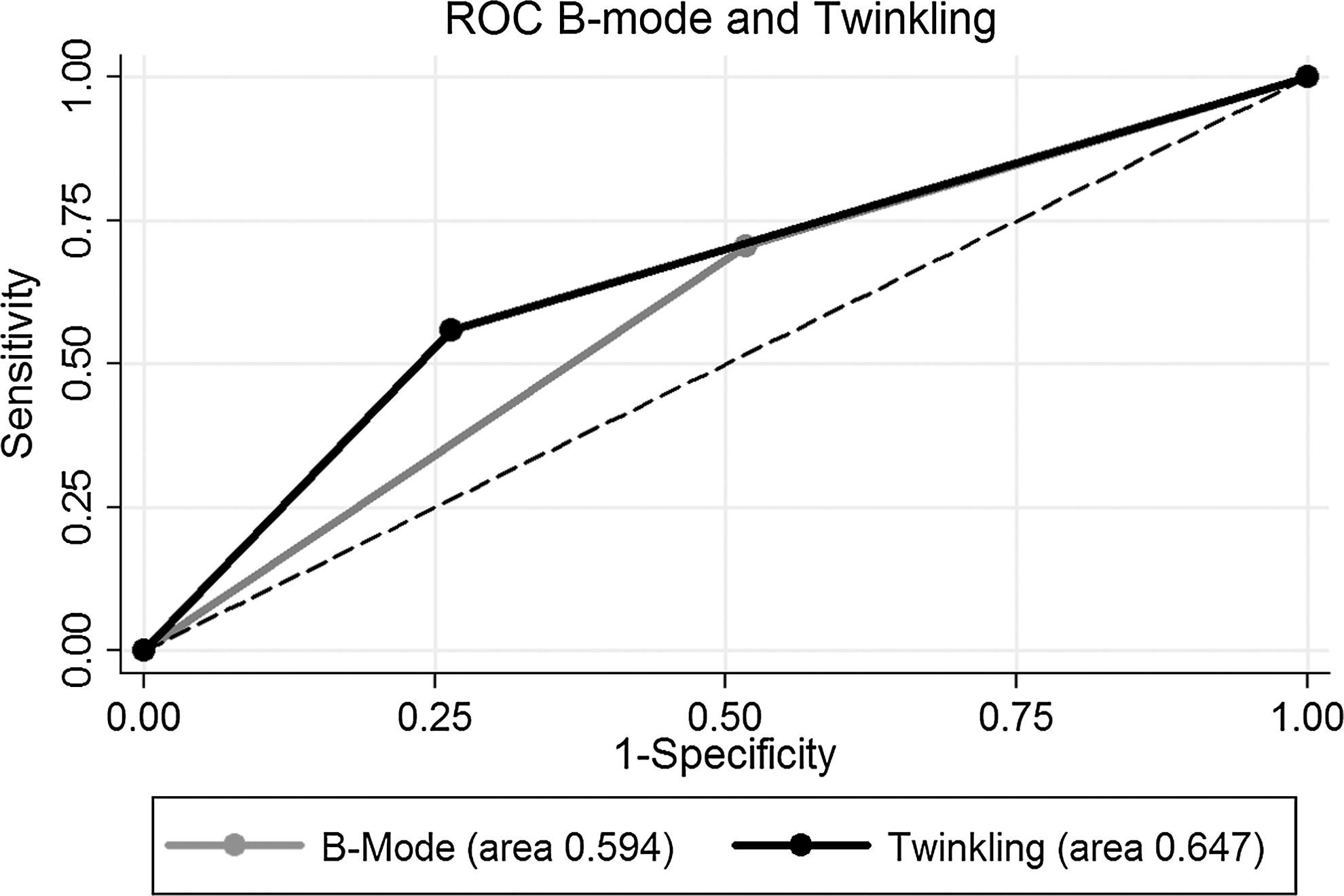
Receiver operator characteristic (ROC) curves for twinkling artifact and B-mode ultrasonography in the detection of kidney stones. Although the areas under the ROC curves are similar for both ultrasound methods, the independent performance characteristics differ with greater sensitivity of B-mode ultrasonography, but greater specificity of twinkling artifact ultrasonography.
SD=standard deviation.
PPV=positive predictive value; NPV=negative predictive value.
When stratified by stone size, there was no difference in the area under the ROC curve between twinkling artifact and B-mode ultrasonography for any of the three stone size categories (P=0.54 for stones <5 mm, P=0.61 for stones 5–10 mm, P=0.11 for stones >10 mm). As stone size increased, the sensitivity, negative predictive value, and percent correctly classified increased for both B-mode and twinkling artifact ultrasonography. For all categories of stone sizes, B-mode was more sensitive, but twinkling artifact was more specific. For each method, the detection of stones was not significantly different between radiologists (P=0.41 for B-mode, P=0.73 for twinkling artifact) or if there were multiple stones in the same area of the kidney (P=0.96).
Role in Endourology
This study evaluated the independent performance characteristics of twinkling artifact seen on color Doppler ultrasonography and B-mode ultrasonography in the detection of kidney stones. Previous studies have concurrently evaluated twinkling artifact with a complete B-mode ultrasonographic evaluation. 27 –29 We determined that on its own, B-mode is inherently more sensitive, while twinkling artifact is more specific for stone detection.
For patients with urinary stone disease, the cumulative radiation exposure of repeated CT scans is of particular concern given the relatively young age of many patients, the increase in prevalence of kidney stones, and the tendency of nephrolithiasis to be recurrent. Many practitioners repeat imaging after lithotripsy, between stone events, and for surveillance of small stones. 30 Despite improvements in the imaging quality with low-dose CT scans, an alternative to CT that does not involve ionizing radiation could have a tremendous impact on the care of patients with recurrent kidney stones.
Acoustically, kidney stones of any composition are intrinsically very different from the surrounding tissue. The speed of sound in tissue is around 1540 m/s, while it is almost threefold higher in stones (range 3500–4600 m/s). 31 –33 Stones have twice the density of water; thus, the characteristic acoustic impedance of a stone is roughly sixfold higher than tissue. Despite these dramatic differences and in part because of signal compression, commercial ultrasound machines currently detect and display an echogenic focus of the proximal reflection of the stone that is often not dramatically different in intensity compared with the surrounding tissue and renal sinus. Also, the characteristic posterior acoustic shadow is created by greater absorption and reflection of the sound wave by the stone. Spatial compounding, however, creates shadows at different angles that are averaged, decreasing the visibility of the posterior acoustic shadow. This may lead to small but clinically significant stones being missed by ultrasonography. 12 When stones are detected, 60% to 79% of the time there may be size discordance, with ultrasonography tending to overestimate stone size. 6,10
After the twinkling artifact was first discovered using color Doppler ultrasound on various parenchymal calcifications, 19 there was hope that the twinkling artifact would improve the detection of stones using ultrasound. In previous meta-analyses, B-mode ultrasonography had a pooled sensitivity of 45% and specificity of 88% for renal stones. 10 In other studies, the addition of color Doppler scanning with the twinkling artifact to a standard B-mode ultrasound session improved sensitivity from 48% to 66% to 55% to 99%. 28,29 It is unclear why twinkling is absent in some stones and present in some kidneys without kidney stones. The cause of these false positives 26 and especially false negatives are not currently understood but may be related to the chemical composition of the stone, 34,35 presence of “microlithiasis,” 26 ultrasound machine settings, or perhaps the age/generation of the ultrasound machine. 22
Ultrasonography with the twinkling artifact for enhanced stone detection has tremendous clinical potential, especially if it can be improved. Ultrasound is safe even for pregnant women and children, involves no ionizing radiation, and is less expensive than CT scans. Improvements in the accuracy and precision of ultrasonography in detecting and sizing of stones might lead to increased utilization of this modality. Existing ultrasound systems, however, are general purpose instruments optimized for characterizing soft tissue inhomogeneities and blood flow, not hard structures such as stones. One of the goals of our research group is to harness these dramatic differences between tissue and stone and create a new commercial ultrasound mode dedicated to kidney stone detection and more accurate sizing. We have been working to develop stone-specific detection algorithms to enhance the display of the twinkling artifact and improve the accuracy of stone sizing. Using our software-based research ultrasound engine, we have tested these signal processing algorithms in phantoms and are now testing these algorithms in humans with kidney stones. These efforts may allow us to generate a new commercial ultrasound mode dedicated to stone detection that is more accurate and precise with less dependence on the skill of the sonographer.
Footnotes
Acknowledgments
The authors would like to thank Dr. Oleg Sapozhnikov for initiating and guiding this research. This work was supported by grants NIH DK48331, NIH DK92197, NSBRI through NASA NCC 9-58, and the UW Commercialization Gap Fund.
Disclosure Statement
No competing financial interests exist.