
Abstract
Distal ureter bladder cuff (DUBC) excision is an essential part of radical nephroureterectomy (RNU), but the technique to accomplish it remains controversial. We describe a novel technique of transurethral distal ureter balloon occlusion before detachment (TUDUBOD) whereby the affected ureter is occluded with a 5F Fogarty balloon catheter and circumferentially incised until the perivesical fat to detach it from the bladder. In the 13 patients who were treated between May 2005 and May 2010, mean surgical time for TUDUBOD was 21.3 minutes. Results for surgical margins were always negative; at mean follow-up of 39.8 months (range 16–74 mos), 4 (30.1%) patients had bladder recurrences but none occurred at the DUBC excision site or perivesical space. TUDUBOD seems to be a simple, cheap, and effective mean of managing the distal ureter during RNU that keeps with the oncologic principle of preventing tumor cell spillage outside the bladder.
Introduction
We describe a simple, minimally invasive, and cost-effective method of transurethral distal ureter occlusion and detachment that upholds the oncologic principle of preventing spillage of tumor cells outside the bladder.
Technique
Patient preparation
Following administration of general anesthesia, the patient is placed in the dorsal lithotomy position.
Ureteral occlusion
Using a cystoscope, a 5F Fogarty occlusion catheter is introduced into the affected ureter. The distal end of the Fogarty catheter is cut to remove it from the cystoscope, and a connector is used to inflate the balloon with 1 mL saline. Complete ureteral occlusion was tested in the first five cases by injecting 5 mL indigo carmine intravenously and observing efflux of blue dye from the contralateral orifice but not from the occluded one.
DUBC excision
Using a resectoscope, a full-thickness circumferential incision is performed until the perivesical fat to detach the DUBC from the bladder (Fig. 1). Care is taken not to compromise the ureteral wall, to minimize irrigation in the last phase of the procedure to avoid extravasation of the irrigant fluid, and to coagulate the bladder edges circumferentially. Finally, a 22F Foley urethral catheter is inserted.
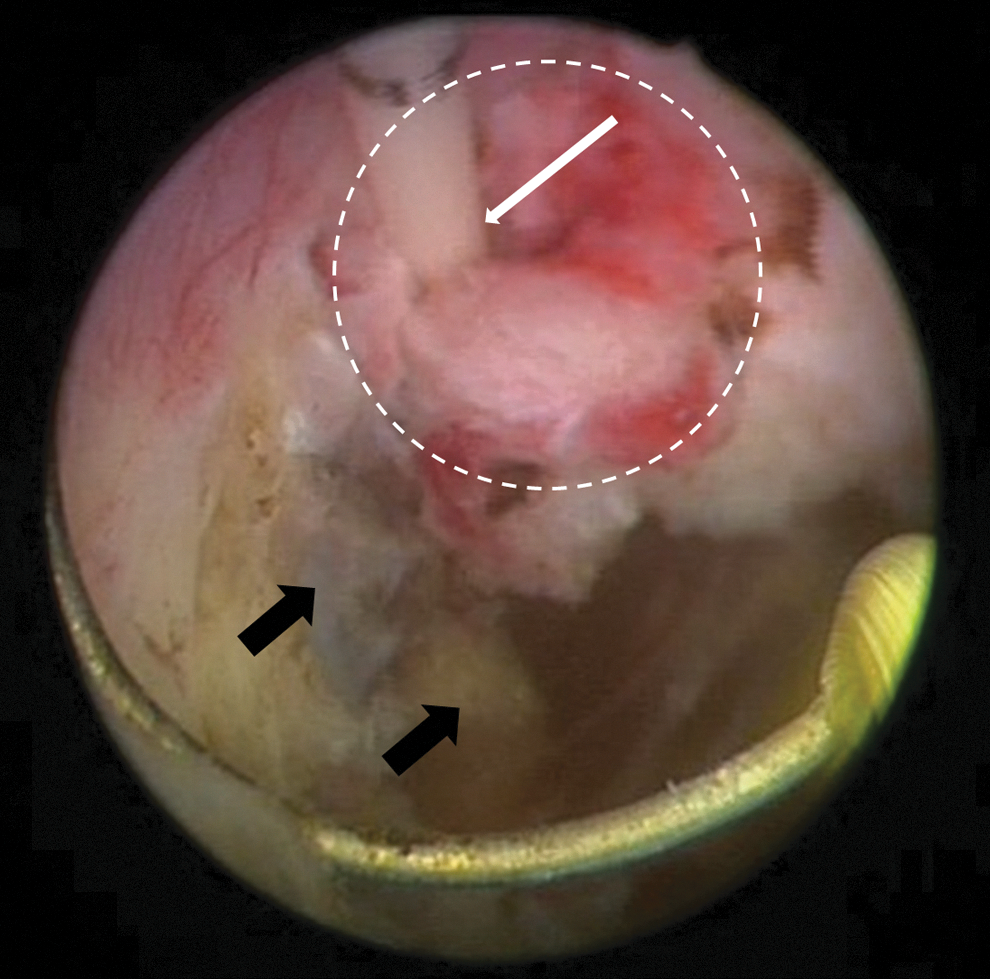
Endoscopic view of transurethral distal ureter balloon occlusion and detachment. The ureteral orifice occluded by the Fogarty catheter (white arrow) has been circumferentially incised (white circle) until the perivesical fat (double black arrow) to be pushed outside the bladder wall.
RNU
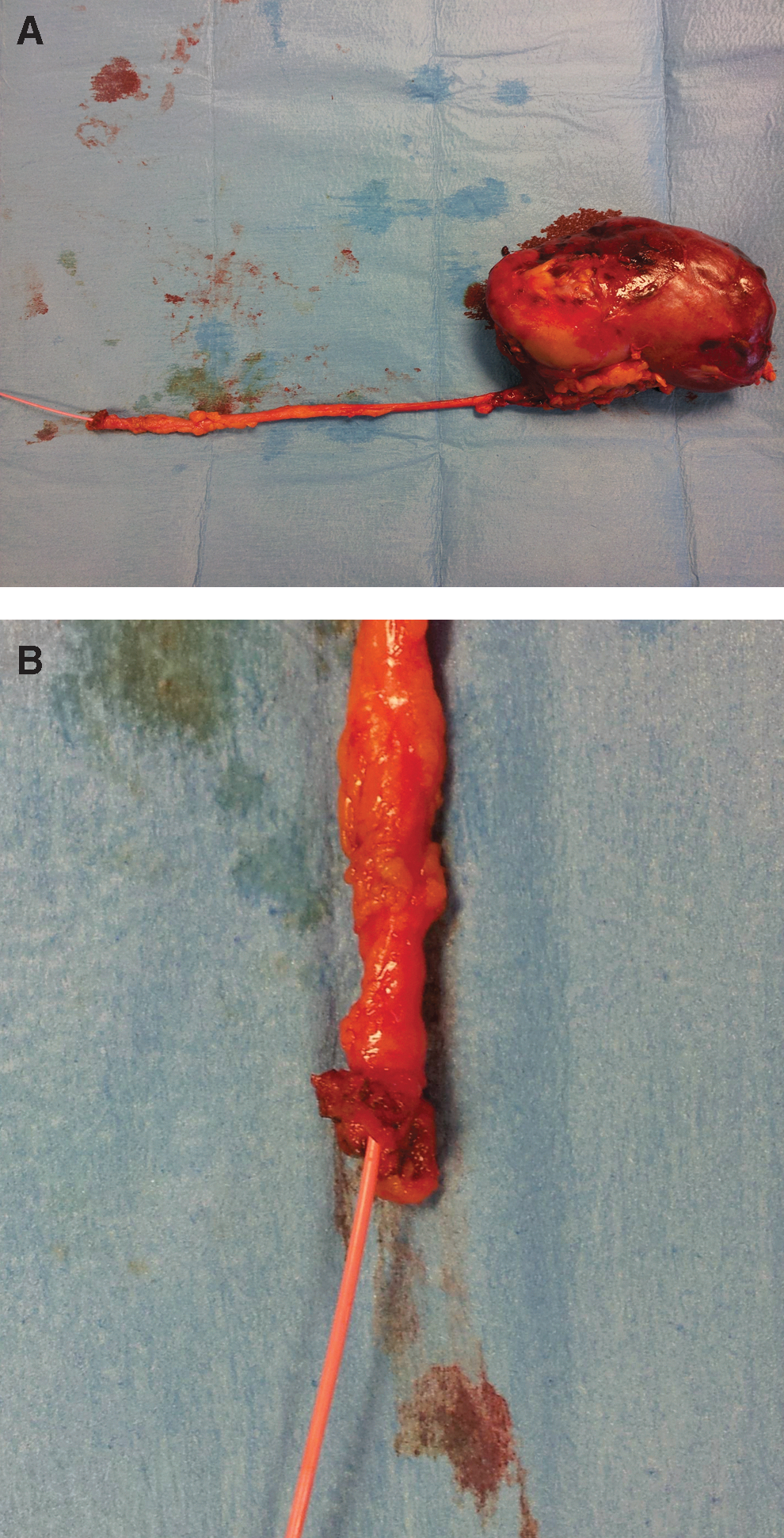
The patient is turned to the flank position. After lumbotomy between the 11th and 12th ribs, the renal artery is ligated and the kidney mobilized superiorly and anteriorly to ligate the renal vein. This allows keeping all of the kidney in one hand while proceeding with progressive ureteral mobilization toward the bladder. Care is taken to clip the proximal ureter before mobilizing the kidney to further prevent tumor cell spillage. Blind manual dissection of the distal ureter is performed until there is feeling of the portion of the Fogarty catheter coming out from the ureteral orifice, which is then clamped to prevent balloon deflation and cut (Fig. 2). A drain running from the perivesical area to the renal hilum is left in place. The Foley catheter is removed on postoperative day 7 after a normal findings on cystography.
Equipment
• Cystoscope
• 5F Fogarty catheter and ureteral catheter connector
• Resectoscope
Patients
After Institutional Review Board approval, from May 2005 to May 2010, a total of 13 patients underwent transurethral distal ureter balloon occlusion and detachment (TUDUBOD) before RNU. Patient data are summarized in Table 1. Two patients had a history of bladder cancer, and the diagnosis of UT-TCC was made by routine upper tract imaging; the remaining 11 patients presented with hematuria, and the diagnosis of UT-TCC was based on CT scanning. Whenever in doubt about radiologic findings (two cases), diagnostic ureteroscopy was performed before DUBC excision to confirm the diagnosis.
DUBC=distal ureter bladder cuff; RNU=radical nephroureterectomy.
The mean time for DUBC excision was 21.3 minutes (range 15–30 min); mean time for changing the patient's position was 19.8 minutes (range 15–25 min); mean time for open RNU was 108 minutes (range 75–140 min), with a mean of 95.7 minutes (range 75–105 min) for those not receiving and 124.1 minutes (range 90–140 min) for those receiving regional lymphadenectomy. Mean overall procedural time was 154.2 minutes (range 110–195 min), and mean postoperative hospital stay was 8.1 days (range 5–10 days). One patient had fever in the postoperative period necessitating antibiotic treatment (Clavien grade II). Final pathologic tumor staging and grading is reported in Table 1.
The surgical margin results were always negative at both kidney specimens and DUBCs. Six of the seven patients with pT3–4 disease received adjuvant chemotherapy. At mean follow-up of 39.8 months (range 16–74 mos), four (30.1%) patients
Role in Urologic Practice
DUBC excision should be performed under direct vision, because a “blind” extravesical approach may result in incomplete excision, when too close to the orifice, or damage to the contralateral ureter, when too extended. The open transvesical approach guarantees precise DUBC excision after preventive ureteral occlusion but violates bladder integrity in both cystotomy and DUBC excision site in a patient with a UT-TCC. Transurethral DUBC excision represents an attractive means of avoiding such a problem.
The “pluck” technique has been suggested to be simple and oncologically safe, 3,6 but it lacks ureteral occlusion, thus potentially exposing to tumor cell spillage outside the bladder. As a matter of fact, there are at least six well-documented cases in the literature of extravesical tumor recurrence in patients having undergone such a procedure, 8 –13 therefore recommending ureteral blockage before DUBC excision.
Gill and associates 14 suggested transurethral partial circumferential incision of the intramural ureter, ligation of the orifice with an endoloop through two needlescopic 2-mm ports placed transvesically, and transurethral completion of DUBC detachment. The same group subsequently confirmed this method to be oncologically safer than transurethral DUBC detachment or laparoscopic extravesical stapling. 15 Cheng and colleagues 16 used cystoscopy to rule out concurrent bladder cancer and establish a pneumovesicum, and three transvesical ports to ligate the ureteral orifice and excise the DUBC with diathermy scissors. A one-port pneumovesicum method has recently been described to excise the DUBC and occlude it with a Hem-o-lok clip before pushing it outside the bladder. 17
Although reported to provide midterm oncologic results comparable to those of the other techniques of DUBC excision, 18 these endoscopic transvesical procedures are technically difficult and violate bladder integrity. Therefore, totally transurethral ureteral occlusion and DUBC detachment remain more oncologically sound and easy to perform also for urologists who are not skilled in laparoscopy.
Agarwal and coworkers 7 described transurethral partial circumferential incision of the intramural ureter, ligation of the mushroom-shaped ureteral stump with a PDS endloop, and subsequent completion of DUBC excision until the perivesical fat. In the 13 treated patients, mean surgical time was 28 minutes, and there were no positive surgical margins. At a mean follow-up of 15 months, bladder recurrences were seen in 5 (45%) of the 11 patients who had the undergone surveillance cystoscopy; two recurrences occurred close to the excised ureteral orifice but none at the ureteral scar or in the perivesical space. Pathak and colleagues 19 described transurethral partial circumferential incision of the intramural ureter and placement of a Hem-o-lok clip at the ureteral orifice through the straight working channel of a rigid nephroscope before completing DUBC excision. Both techniques are relatively fast and easy to perform, but care must be taken not to incise the bladder wall to the perivesical fat before the ureteral orifice is occluded.
To avoid such problem, Mueller and associates 20 suggested cystoscopic injection of fibrin sealant (Tisseel®) through a ureteral catheter to occlude the distal ureter before DUBC excision. In the eight treated patients, there was no positive surgical margin and no intra- or extravesical tumor recurrence at a mean follow-up of 11 months. Our technique is equally easy to perform, but the Fogarty catheter is cheaper than Tisseel. Most important, our technique proved to fulfill well the oncologic principle of completely occluding the distal ureter before incising the bladder wall, because we saw no tumor recurrence at the DUDC excision site or at the perivesical space at a much longer mean follow-up of nearly 40 months. Such a finding is made even more relevant by the fact that almost 70% of our patients had a high-grade disease.
If the strength of our technique is being simple, fast, cheap and, above all, holding the basic oncologic principle of preventing tumor cell spillage, some technical details could potentially be further refined. First, care must be taken to avoid excessive irrigation, because this could lead to postoperative hyponatremia. 21 Although we had no such problem, we are currently exploring the possibility of using devices working in saline, such as bipolar resectoscopes or the holmium laser. Second, the patient needs repositioning, leading to prolonged operative time. Again, we are exploring the possibility of performing the DUBC excision with a flexible cystoscope with the patient in the flank position, 22 thus eliminating the need for repositioning. Potential limitations include the technique not being suitable for tumors located close to the ureteral orifice, the relatively small number of cases, and the absence of a control group receiving the “pluck” technique.
Conclusion
TUDUBOD seems to be a simple and effective mean of managing the distal ureter during RNU with favorable midterm oncologic results. It is applicable to both open and laparoscopic RNU and, above all, keeps with the oncologic principle of preventing tumor cell spillage outside the bladder.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.