
Abstract
Background and Purpose:
Open radical inguinal lymphadenectomy is reported to have morbidity as high as 50%. We describe our endoscopic inguinal lymphadenectomy that aims at decreasing the morbidity of the procedure without compromising the oncologic outcomes.
Patients and Methods:
Eleven groin dissections were undertaken in seven male patients. The procedure was performed via three ports. The first one was a 10-mm incision 3 mm distal to the apex of the femoral triangle. Two additional trocars (10 mm and 5 mm) were positioned 6 cm medially and laterally to the apex of the triangle, respectively. Taking the great saphenous vein as a landmark, the superficial and deep components were dissected. The boundaries of dissection were the same as those of radical inguinal lymphadenectomy. The numbers of lymph nodes harvested were recorded. The morbidity was retrospectively analyzed.
Results:
The mean operative time was 126 minutes. The mean number of lymph nodes was 12.3. The averaged output of drainage per leg was 50.8 mL each day. There were only three minor complications: One patient had hypercarbia and pneumoderm, and another had 50 mL of seroma; the third had 180 mL of lymphocele. Follow-up ranged from 4 to 27 months (mean 16.3); there was no evidence of recurrence and other sequelae.
Conclusions:
Endoscopic inguinal lymphadenectomy is feasible for patients with penile cancer and genital malignancy. The technique reduces the risk of
Introduction
Despite the decline of the morbidity of modified inguinal lymphadenectomy for the past two decades, the postoperative complications remain high, ranging between 26.7% and 38.9%. 3 –5 In comparison with the radical lymph nodes dissection, the complication rate of the modified inguinal lymphadenectomy is lower, but the oncologic safety of this procedure has been questioned. 6 Some authors even suggested that the modified inguinal lymphadenectomy for penile carcinoma had no advantages. 7 To reduce morbidity of open radical lymphadenectomy without compromising the oncologic result, an endoscopic subcutaneous modified inguinal lymphadenectomy was first described by Bishoff and associates 8 in 2003 and successfully performed by Tobias-Machado and colleagues 9 in 2005.
We present our technique of endoscopic inguinal lymphadenectomy to assess its feasibility and efficacy and analyze the complications related to the procedure.
Patients and Methods
Between September 2009 and January 2012, we performed 11 inguinal lymphadenectomies for penile squamous carcinoma in four patients (bilateral) and for scrotal Paget disease in three patients (unilateral). The average age of the patients was 63.9 years, ranging 50 to 83 years. The body mass index (BMI) averaged 24.7. In four patients with penile carcinoma, one patient was classified as stage I of the disease according to Tumor-Node-Metastasis staging system (T1N0M0), and three were in stage II (T2N1M0). The patient in stage I refused to receive prophylactic groin node resection after partial penectomy. One year later, he was admitted to the hospital again for his left groin node enlargement. After positive node biopsy, he then had bilateral inguinal lymphadenectomy. The remaining three patients had therapeutic bilateral inguinal lymphadenectomy because of positive groin nodes. Three patients with scrotal Paget disease had prophylactic ipsilateral groin lymphadenectomy after local dissection. Prophylactic antibiotics were administered in all patients before surgery.
Surgical procedure
Because endoscopic inguinal lymphadenectomy is a novel alternative for groin node dissection, all risks and benefits of this new procedure were discussed in detail with the patients. This study was also approved by the ethics committee of the hospital. All patients signed a consent form to participate in the study.
Patients were positioned supine on a split-leg bed for bilateral dissection (Fig. 1) or were frog-leg position with the knee flexed for unilateral surgery. Then the femoral triangle was marked with colorant. A cross line with its middle point in the saphena hiatus was also drawn, and the triangle was divided into four quadrants—superomedial (SM), superolateral (SL), inferomedial (IM) and inferolateral (IL) zones (Fig. 2). The positions of the incisions and numbers of trocars were performed as described by previous reports in the literature (Fig. 2). 8,9

Patient positioned supine on a split-leg bed for bilateral dissection.

A cross line with its middle point in the saphena hiatus, four quadrants drawn. Positions of three trocars (left).
It is very important to create a working space for inguinal lymph node dissection via laparoscopy. After the skin flap was separated in this plane, the anterior working space resembled a “camping tent.” The ceiling of the tent was formed by the skin and the subcutaneous tissue, which preserved the continuity of the lymphatic and vascular supply to the overlying skin. The floor consisted of a deep layer of tissues, including the superficial inguinal lymphatic tissues, the great saphenous vein, the fascia lata, and muscles of the thigh (Fig. 3a). The boundaries of dissection were the apex of the femoral triangle inferiorly, the sartorius muscle laterally, the adductor longus muscle medially and 10 mm superiorly to the inguinal ligament.
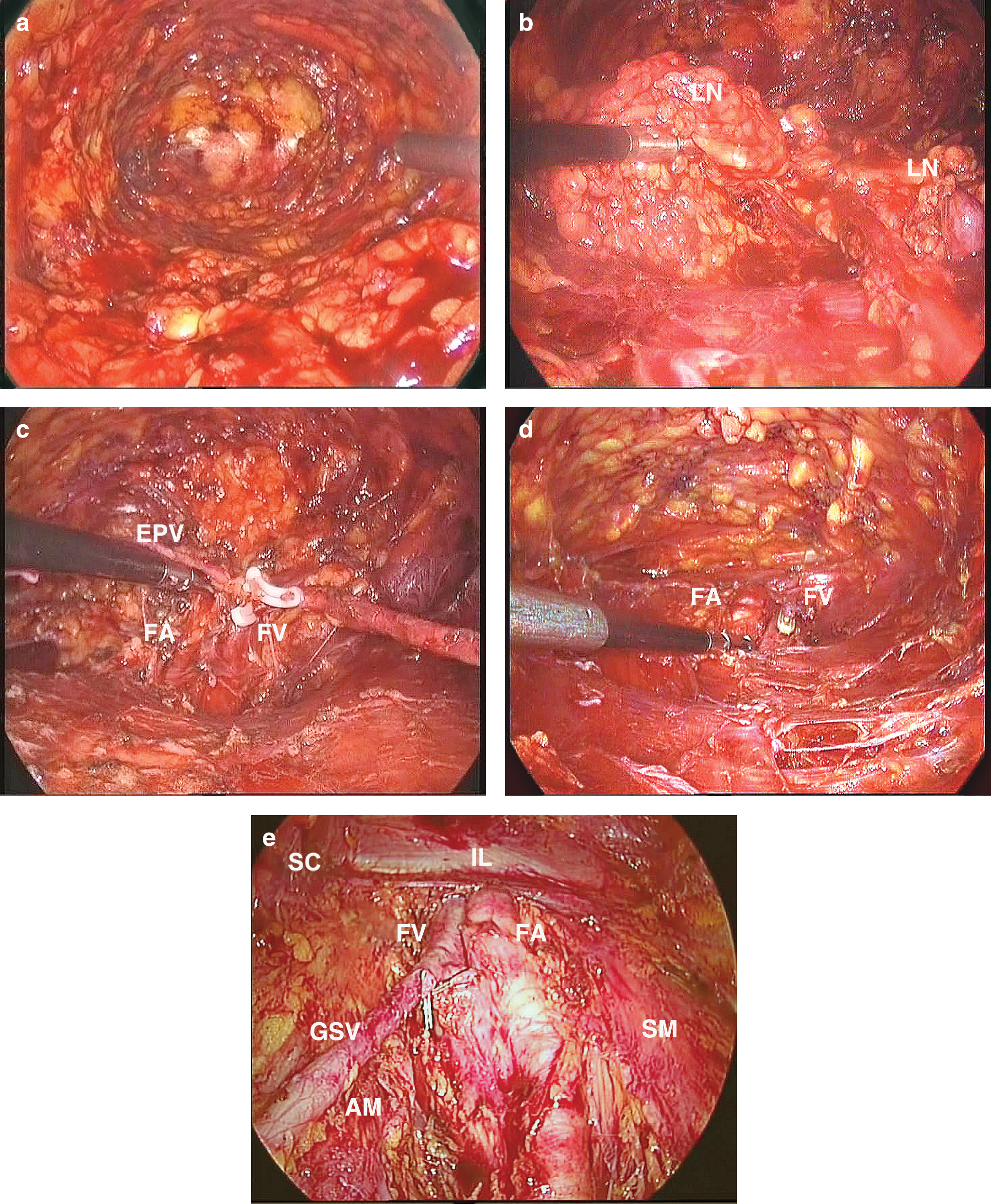
The great saphnous vein was considered as an anatomic landmark, and the IM, IL, SM, and SL nodes along the vein (zone IM, IL, SM, and SL) were stripped step by step (Fig. 3b, 3c). After the saphenofemoral junction was exposed, the entrance of the long saphenous vein was well dissected and controlled with polymer clips (Fig. 3d). If possible, without compromising the dissection, the saphenous vein itself and its branches should be preserved as far as possible (four cases preserved).
After the anterior surface of the femoral vein was cleaned off, the inguinal ligament was identified by the silver-white transverse fibers. The femoral sheath was opened with an ultrasonic scalpel, and the femoral artery was dissected bluntly with the suction rod; subsequently, the femoral vein medial to it was also cleared. Both vessels were clearly skeletonized. The deep inguinal lymph nodes (Cloquet node) were dissected from the inguinal ligament to the fossa ovalis and then marked with clips for pathologic analysis. Dissection was caudally continued following the femoral and the saphenous tract. All the superficial and deep lymphatic tissue and nodes in the region were completely resected en bloc.
After the inguinal region dissection, the saphenous vein, femoral vein and artery, and pectineus, adductor longus, and sartorius muscles were identified clearly (Fig. 3e). Suction drainage was placed through the 5-mm incision and maintained until drainage was less than 15 mL daily for 2 consecutive days. The thigh perimeter was measured to assess the lower extremity edema. A light pressure dressing was used over the groin region until hospital discharge.
Results
Eleven inguinal lymphadenectomies in seven patients were performed. Patients' demographics and clinicopathologic data are summarized in Table 1. The mean operative time per leg was 126 (range 90–180) minutes. The total number of lymph nodes removed was 135, with an average of 12.3 (range 7–15) nodes per leg, among which mean deep nodes of 1.1 (range 0–3) were included. The mean output of drainage per leg was 50.8 (range 5–130) mL each day. The mean postoperative hospital stay was 10.8 (range 7–15) days. One patient had hypercarbia and pneumoderm during the operation; it was successfully managed by hyperventilation and adequate liquid transfusion. There were two cases of minor complications; one patient had 50 mL of seroma in the left leg. After several needle aspirations and application of a compression bandage, the problem was resolved successfully. Another patient, who had the saphenous vein excision, had 180 mL of lymphocele in his left thigh. Continued drainage was administered for 12 days. All the patients had no lower extremity edema after surgery (44.61±2.25 vs 44.86±2.26, P=0.054) and returned to normal activity within 15 days.
BMI = body mass index.
The follow-up interviews were obtained in person. The mean period of follow-up was 16.3 (range 4–27) months. There was no evidence of recurrence of tumor and postoperative sequelae, such as incisional pain and numbness, or lymphedema in the low extremity.
Discussion
Radical inguinal lymphadenectomy remains the gold standard for the treatment of patients with metastatic penile carcinoma, as well as with various genital malignancies. It is not without complications, however, and some of them are fraught with considerable morbidity, such as incisional infection, necrosis, dehiscence, and lymphorrhage, etc. This really inspired the strategies for diminishing the morbidity of inguinal lymphadenectomy. In 2003, Bishoff and coworkers 8 first described the use of minimally invasive laparoscopic techniques in two human cadavers and one patient with penile carcinoma in stage T3N1M0. It was not, however, completed in the patient, because of a large, adherent node to the femoral vessels and an open conversion was necessary. It was Tobias-Machado and colleagues 9 in 2005 who performed it successfully in a comparative study between video endoscopic inguinal lymphadenectomy and standard open procedure for penile cancer; the authors referred to the endoscopic technique as VEIL.
Afterward, more and more reports of endoscopic inguinal lymphadenectomy were published by Sotelo and coworkers, 10,11 Tobias-Machado and associates, 12 Master and colleagues, 13 and Correa and Tobias-Machado. 14 Although fewer than 200 cases of endoscopic inguinal lymphadenectomy for penile cancer have been reported in the literature in the last decade, the endoscopic approach is regarded to be a safe and feasible technique that appears to reduce the complications associated with the standard open approach, and the early oncologic results are encouraging.
We performed the procedure based on the pioneers of Tobias-Machado and coworkers 9 and Sotelo and colleagues. 10,11 In our experience, however, we believe that separating the skin flaps in the femoral area plays a crucial role in creating working space. Instead of scissors or harmonic scalpel, cautery was used to separate the fibrofatty tissue between the subcutaneous fat and deep layer of fascia along the Scarpa fascia. This was equivalent to raising flaps during an open procedure. Electrocoagulation could decrease the bleeding and make the separation faster. In this way, we succeeded in creating a working space, which was large enough to attain excellent dissection.
After the skin flap raising by insufflation, the great saphenous vein was taken as an anatomic landmark, the four quadrants of the superficial node were stripped step-by-step up to the saphenous arch at its junction with the superficial femoral vein, and the deep nodes were then also removed. The boundaries of dissection included the following anatomic landmarks: Inguinal ligament, adductor muscle, sartorius muscle with the femoral vein and artery as the floor of dissection, as shown in Figure 3e.
The node count is still believed to be an important surrogate marker for the quality of lymph node dissection. The average number of lymph nodes in our series was 12.3 per leg with 1.1 deep lymph node, which was comparable to the number reported in previous reports in the literature. 4,13 Consequently, we believed that our endoscopic procedure would meet the principles of the conventional technique, which is a radical resection of inguinal lymph nodes. There was no recurrence in our series after 16.3 months of follow-up. The early oncologic outcomes are encouraging. We believed this satisfactory outcome was attributed to the radical boundary of dissection and adequate lymph nodes of harvest.
Another benchmark of this new technique is associated with the complication. In our series, 3 of 11 legs in seven patients had complications, of which the morbidity rate was 42.9% (3/7). Although the rate of morbidity in our series was higher indeed, nevertheless, there were no severe complications such as skin necrosis, incision infection, dehiscence, vessels damage, or lymphorrhagia. On the other hand, it may be related to the small number of patients in the study. One patient, at age 83 years, had hypercarbia and pneumoderm during the operation; this was probably attributed to his elderly age. Another one had seroma in the left leg. The reason was that the compress bandage was not tight enough to cover. A third patient had thigh lymphocele because of inadequate drainage. Although these complications were not quite difficult to treat, we should still be alert every moment to prevent the occurrence, especially in elderly patients.
We considered that the lower severe morbidity rate in our study was related to the following factors: First, the large incision was replaced by three small incisions that minimize the skin and subcutaneous tissue injury and decrease the damage by mechanical retraction. Second, the skin flap was raised by the dissection in definite anatomic planes, which ensured the lymphatic and blood supply to the skin flap. Last, adequate ligature of major lymph vessel by harmonic scalpel or clips was essential for decreasing the morbidity associated with the lymphatic system.
There have been few reports about the BMI of patients undergoing endoscopic inguinal lymphadenectomy. Master and associates 13 noted that there was no increased incidence of complications restricted to obese patients, who were regarded as a challenge in open surgery. In comparison with Western patients, our patients who were normal weight (mean BMI=24.7) were much thinner than those reported in the literature. 11 We also noted that there was a correlation between the BMI and operative time. The thinner the patient, the shorter the operative time.
Because ambulatory surgery is not in current practice because of the social insurance system in our country, a hospital stay between 7 and 10 days is usual for these patients. So the hospital stay (average 10.8 days, 7–14 days) was much longer than that in published reports in the literature. 9,11,13
Conclusions
This new technique not only reduces the risk of postoperative complications because of the smaller cutaneous incisions, but also achieves the identical results of quality of lymph node dissection compared with open surgery. The oncologic results are encouraging. On the other hand, the disadvantages are the requirement of a surgical team trained in endoscopic techniques and specific surgical instruments. Moreover, long-term oncologic control has to be proven through a prospective, randomized, comparative study.
Footnotes
Disclosure Statement
No competing financial interests exist