
Abstract
Introduction:
Malignant ureteral obstruction (MUO) has traditionally been a difficult problem to manage. Indwelling ureteral stents have a failure rate up to 50%, necessitating the placement of percutaneous nephrostomy (PCN) drainage, which has associated complications and impacts on quality of life. Recently, metallic ureteral stents have emerged as a treatment for extrinsic ureteral obstruction. We present our initial experience using Resonance (Cook Urologic, Spencer, IN) full-length metallic stents for MUO.
Materials and Methods:
20 patients (27 renal units) with advanced cancers and MUO were treated with metallic stents. Patients were followed prospectively to evaluate for recurrent obstruction. Perioperative morbidity and overall mortality were recorded.
Results:
The mean patient age was 49.9 years (SD 18.9). The primary malignancies causing MUO were gastrointestinal (8), gynecologic (6), genitourinary (2), or other (4). All but two renal units had been previously treated with traditional stents. Eight out of 20 (40%) patients required further intervention for their MUO. Mean time to failure for the metallic stents was 7.4 months (222 days). Two patients required conversion to percutaneous drainage. Five patients required change to traditional stents (3) or removal of metallic stents. At the last follow-up, sixteen patients had died. Fourteen of the sixteen patients died with functioning metallic stents in place, although one patient who initially had bilateral metallic stent placements had a left stent removed due to migration. Of the remaining four living patients, two have functioning metallic stents at a mean follow-up of 42 months.
Discussion:
MUO remains a difficult clinical problem in a group of patients with a high mortality. While metallic stents ultimately have a failure rate similar to that of traditional stents, the mean time to failure is longer. Therefore, metallic stents may benefit patients with MUO, because the longer dwell time may eliminate the need for more frequent stent changes or further interventions.
Introduction
Traditional management options involving ureteral stents or percutaneous nephrostomy (PCN) tubes have disadvantages. Conventional polyurethane ureteral stents are associated with high failure rates and significant complications. 6 –8 PCN is associated with a high complication rate, and patients reported a poor quality of life. 9,10 Recently, full-length metallic stents (Cook Urologic, Spencer, IN) have been introduced in the United States as an alternative for MUO management. Secondary to their metal composition, these stents have been shown in vitro to be more resistant to extrinsic compression than their plastic counterparts. 11 Limited series in Europe have shown short-term efficacy of these stents for MUO. 12 We herein describe our initial experience with Resonance (RES) in a cohort of patients with MUO.
Materials and Methods
Between July 2007 and June 2008, we placed metallic stents (RES; Cook Urologic) in 20 patients with MUO. In 7 patients, stents were inserted bilaterally, for a total of 27 stented ureters.
Patients were either newly diagnosed (2) with MUO or had a prior diagnosis (13) and had previously been diverted with traditional polyurethane ureteral stents. Obstruction was diagnosed by clinical signs, increasing azotemia, or incidentally through routine cancer surveillance imaging. Diagnosis was confirmed with ultrasonography, computed tomography, magnetic resonance imaging (MRI), and diuretic renal scintigraphy. The decision to place metallic stents was based on patient comorbidities, cancer prognosis, and need for additional chemotherapy.
Stent placement
After an initial cystoscopic examination of the bladder, retrograde pyelography was performed in all patients to define the obstructed ureteral segment. If a traditional stent had been previously placed, then a guide wire was placed either through the stent lumen or adjacent to the stent before stent removal and a subsequent retrograde pyelogram. A hydrophilic glide wire was then negotiated past the point of obstruction and advanced into the kidney under fluoroscopic visualization. A 5F torque catheter (Boston Scientific, Natick, MA) may be necessary to bypass tightly stenotic segments. Once the wire was in place, a calibrated 5F ureteral catheter was passed over the wire until the tip reached the ureteropelvic junction (UPJ). Ureteral length was determined endoscopically by visualizing markers on the ureteral catheter at the ureterovesical junction. The glide wire was then replaced with an Amplatz super stiff wire (Boston Scientific), and the ureteral catheter was removed. A second safety wire was placed using a 8–10F coaxial dilating system.
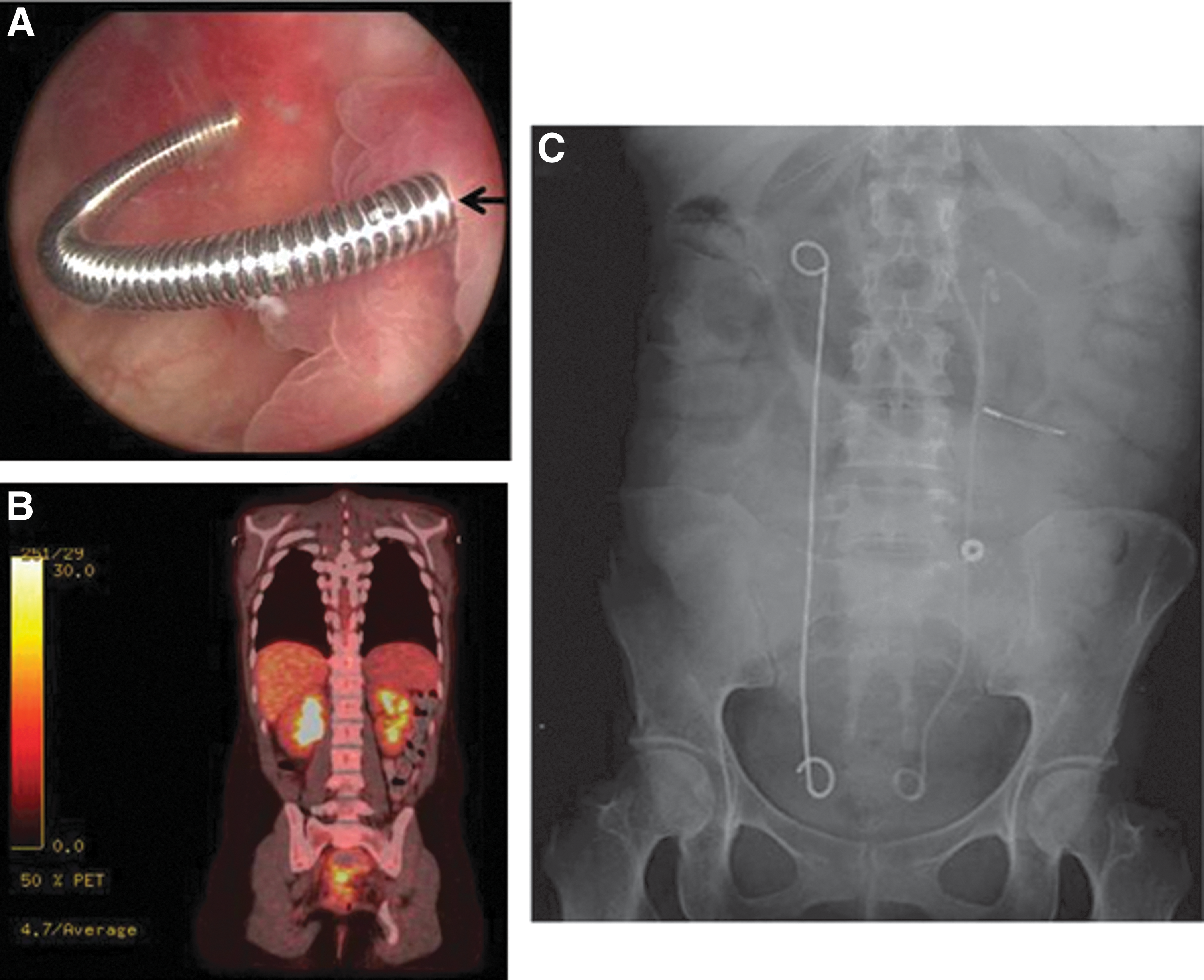
The metallic stent introducer system was then passed over the super stiff wire with the outer 8.3F sheath radio-opaque tip positioned at the UPJ. The wire and the inner introducer catheter were removed, leaving the outer sheath in place. The metallic stent was then placed through the sheath and advanced proximally using the previous introducer as a pusher. All stents are 6F in diameter, and the length is determined by prior ureteral measurements. Importantly, the metallic stent does not have an inner lumen and is not passed over a wire. When the proximal curl of the stent is seen beyond the tip of the sheath in the renal pelvis, the sheath is slowly removed, keeping the inner catheter in place. The outer sheath is completely removed when the distal curl is seen deployed within the bladder. Finally, correct intravesical positioning is confirmed with cystoscopy, making any adjustments necessary with flexible graspers. Figure 1 shows an intraoperative cystoscopic image and fluoroscopic image during placement of bilateral metallic ureteral stents. Preoperative PET scan is also shown.
All patients were prospectively followed in the hospital postoperatively for resolution of symptoms and azotemia. Patients were also assessed at 6 months with sonography to evaluate for hydronephrosis. Lastly, stent failures, complications, and mortality were recorded.
Results
From July 2007 to May 2009, 20 patients (27 renal units) underwent retrograde ureteral stenting with RES. Patient characteristics are shown in Table 1. Mean age of the patient cohort was 49.9 years (SD=18.9). The patient group consisted of 6 men and 14 women. The primary malignancies causing MUO were gastrointestinal (8), gynecologic (6), genitourinary (2), or other (4). All patients with the exception of one had documented metastatic disease. The one patient without metastatic disease had prostate cancer treated with external beam radiation therapy, and it is unclear whether his obstruction was secondary to his primary malignancy or as a complication of his radiation therapy. All but two patients (three ureters) had previously been stented with conventional polyurethane ureteral stents. There were no peri-operative complications from stent placement noted.
Eight of 20 patients (40%) required further interventions for their MUO, with a mean time to failure of 7.5 months (range 0–18 months). Two of these six patients required conversion to percutaneous drainage for persistent azotemia.
Four patients required a change to traditional stents, and two patients required removal of metallic stents secondary to obstructive symptoms. Of note, one patient who was converted for obstructive symptoms continues to have similar complaints with indwelling traditional ureteral stents.
At the last follow-up, sixteen patients died at a mean age of 9 months (range 1–28 months) from stent placement. Fourteen of the sixteen patients died with metallic stents in place.
In the subgroup of the patients still living (four patients), two patients have metallic ureteral stents in place. The mean follow-up to date is 11.4 months (range 6.5–46 months). At follow-up, there did not appear to be any evidence of persistent obstruction or infection, as documented by renal ultrasound or urine culture when available.
Discussion
MUO is a very difficult problem to treat with a dire prognosis. Patients can present with renal colic, infection, urosepsis, and progressive azotemia. Other patients may be discovered incidentally on routine follow-up imaging for their primary cancers. The urologist is typically a consultant, called on to provide advice and treatment regarding renal decompression. Regretfully, the traditional treatment choices have been ineffective, with potentially significant morbidity and deleterious effects on quality of life.
Wong et al. retrospectively reviewed clinical outcomes of 102 patients who underwent renal decompression (NT or conventional stent) for MUO. Median overall survival was 6.8 months (range 4.8–9.3), and the overall survival rate at 12 months was only 29%. 1 Univariate analysis found inferior overall survival associated with metastasis, nephrostomy insertion, prior treatment for cancer, and diagnosis of MUO in previously established malignancy. Overall survival was 63% versus 12% for patients with 0 or 1 versus 3 or 4 risk factors, respectively. While the initial failure rate for decompression was low (5%), there was a significant complication rate (53%).
In a similar cohort retrospectively analyzed by Shekarriz et al., 103 patients with advanced malignancy underwent palliative diversion. 4 The median survival and days in the hospital were 112 and 45, respectively. Overall, 51% of patients had unsuccessful ureteral stenting requiring secondary percutaneous procedures, and 68.4% had complications. The mean remaining lifetime spent in the hospital after diversion was 52%, with 15% of patients never leaving the hospital. Both studies highlight the dismal survival associated with MUO, and the substantial complications and questionable benefits of urinary diversion.
The recent introduction of the RES (Cook Urological, Spencer, IN) provides another alternative in the management of MUO. This stent is constructed of MP35N® alloy, a composite of nickel-cobalt-chromium-molybdenum. In comparison with the traditional polyurethane/polyethylene stents, this stent is nonfenestrated and is a continuous metal coil with an inner wire welded to both closed ends. Thus, introduction (antegrade and retrograde) is through a ureteral sheath rather than over a guide wire. Proposed advantages of this stent include its high tensile strength, which reduces extrinsic compression, corrosion–resistance, and nonferromagnetic properties, making it MRI compatible.
Blaschko et al. examined in-vivo flow characteristics of the RES compared with standard stents. 13 In a porcine model, flow assessments were performed via infusion through a nephrostomy tube. The standard stent was found to have significantly greater combined flow (intra and extraluminal) than the RES, but not intraluminal flow alone. Thus, under extrinsic compression where intraluminal flow is dominant, the RES would have superior flow. Importantly, while the standard stent could be occluded completely with a ureteral ligature, it was not possible to occlude the RES regardless of the tension of the ligature. Thus, the authors postulated that the RES might be beneficial in the management of MUO. In an in-vitro study by Pedro et al., two wire-based ureteral stents were compared with a standard ureteral stent in terms of tensile strength and radial compression force. 14 Both the RES and a coil-reinforced Applied Medical Silhouette (SIL) (Applied Medical, Rancho Mirage, CA) ureteral stent were more resistant to extrinsic stent compression than ureteral stents, which were not wire based. Comparing the two wire-based stents, the RES had a higher tensile strength, while the SIL was more resistant to extrinsic compression.
The worldwide experience with the RES stents is substantial, but there are limited data published in the literature. The first case report by Borin et al. in the United States described the successful retrograde insertion of an RES in a woman with metastatic breast cancer that had previously failed a single 7F and subsequently failed two 6F standard stents. 15 Successful drainage was documented with a postoperative Whitaker test and ensuing renal scintigraphy at 4 months. Wah et al. reported on their initial experience with RES in 15 patients (17 ureters) with MUO. 12 All stents were inserted antegrade with three stents failing from the outset secondary to bulky pelvic lymphadenopathy. One patient had a stent change at 12 months, and three had their stents changed at 6 months. Four patients were alive with functioning stents (2–10 months), and seven patients died with functioning stents (1 week-8 months). Finally, Nagele et al. recently reported on 14 patients (18 ureters) with ureteral obstruction (benign 5 and malignant 13) who underwent retrograde placement of RES stents. 16 Of those renal units being treated for MUO, stents had to be prematurely removed in 7 cases secondary to persistent hematuria (1), severe dysuria and pain (2), and insufficient drainage (4).
Liatsikos et al. recently published their experience using RES stents in 50 patients, 25 of whom had MUO. 17 They found a 100-percent success rate using full-length metallic stents in their cohort of patients with MUO. The advantage of the RES stent is its increased dwell time and resistance to encrustation. Liatsikos et al. also performed macroscopic, microscopic, and spectroscopic analysis on the stents to detect encrustation. They found that 12 of 54 stents had macroscopic evidence of encrustation, but all stents had microscopic and spectroscopic evidence of encrustation. However, the clinical significance of the latter is unknown. Figure 2 shows stents removed from patients at various lengths of times in our patient cohort. There was no macroscopic evidence of clinically significant encrustation in any of the stents removed or exchanged in our patient cohort, supporting the theory that the metallic stents are advantageous for their increased dwell time and resistance to encrustation.
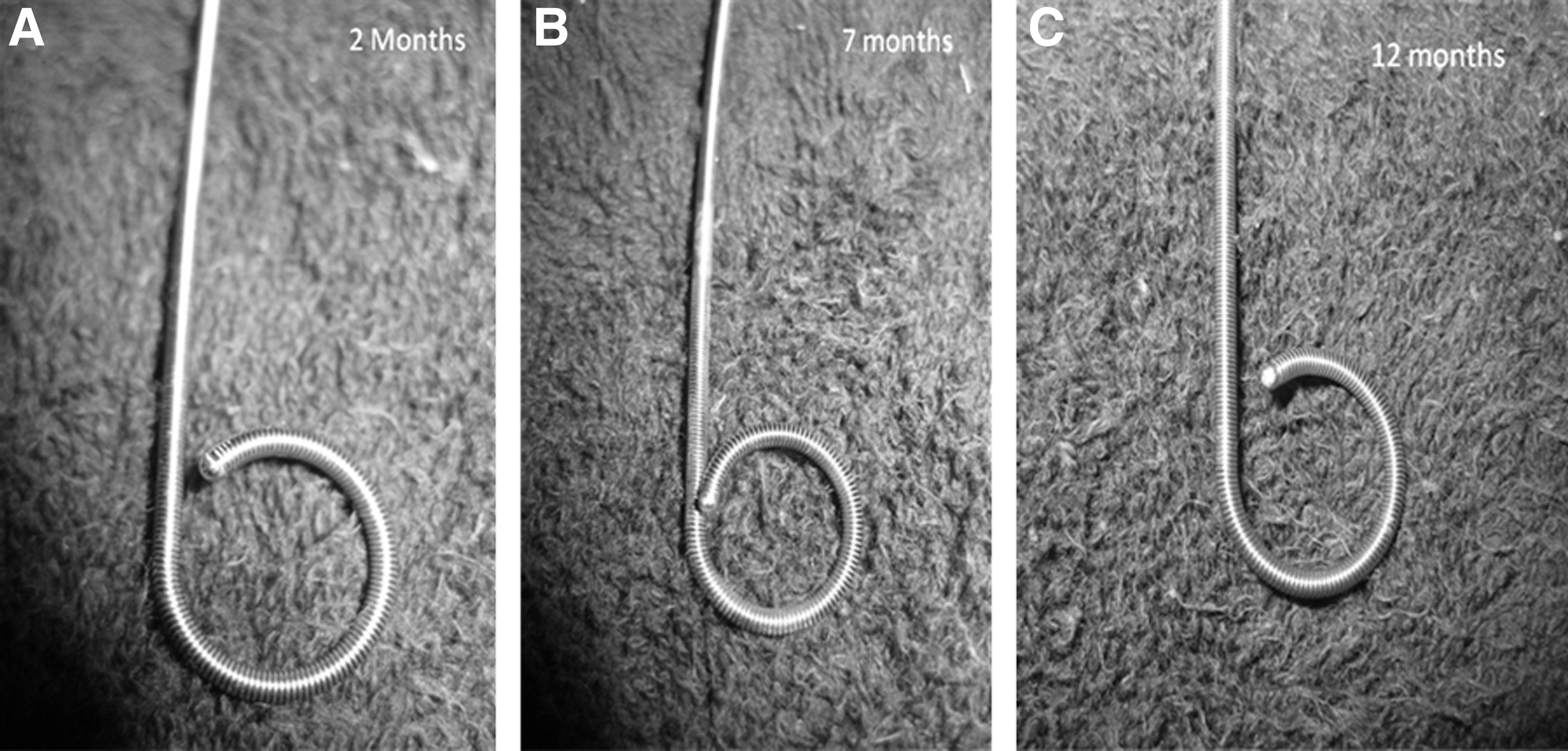
Stents removed from patients at various time intervals.
In our cohort, 8 out of 20 patients (40%) required further intervention for their MUO. This ranged from removal of the metallic stent to placement of PCNs. This failure rate is similar to that of previously published studies using traditional stents. However, the mean time from placement of stent to failure was 6.3 months, which is twice the dwell time for traditional stents. It, therefore, seems that the true advantage of the RES stent compared with a traditional stent is its increased dwell time, as opposed to its decreased failure rate. An increased dwell time is clearly a benefit in these patients, as this would mean a decreased number of stent exchanges and procedures in these patients who have been shown in multiple studies to have a significantly limited life span. This point can be further enforced by the fact that 14 of 16 patients in our cohorts who died had functioning metallic stents at the time of their death.
The economic impact of MUO is also an important factor to be considered in the treatment of these patients. Ganatra and Loughlin retrospectively reviewed a cohort of 133 patients (212 ureters) who had successfully undergone conventional ureteral stenting for MUO. In these patients, the average number of stent changes was 2.8, and the stent change interval was 130.8 days. The estimated yearly cost (billings) for these patients was $4,123 (range, $2,770–10,140), excluding complications and those patients who required PCN tubes. 18 This underscores the need for stents with a longer dwell time that could decrease the number of stent changes required. Thus, while the RES stents are substantially more expensive than traditional stents, they may actually result in cost savings, as stent cost is only a minority of the overall operative cost. The importance of the economic impact is magnified by the fact that these patients have such limited life spans.
Our series highlights the utility of the RES stent in MUO. As documented in other reports, MUO was a very poor prognostic factor that was associated with a dismal survival rate despite urological intervention. In our cohort, the RES stent had a failure rate which was comparable to that of the traditional stents. However, the time to failure was longer when compared with traditional stents. We, therefore, propose that the advantage of the RES stent is its increased dwell time, as opposed to its decreased failure rate. This increased dwell time and time to failure means that patients with these metallic stents will need less frequent changes, which would result in cost savings, and more importantly, an improved quality of life for these patients. In conclusion, we feel that this is an improved option for the urologist in the treatment of the difficult problem of MUO.
Footnotes
Disclosure Statement
No competing financial interests exist.