
Abstract
This year marks 12 years of the world's first robot-assisted radical prostatectomy (RARP) program, the Vattikuti Institute Prostatectomy (VIP). Experience with more than 7000 cases has helped standardize the operation, minimize complications, and enhance functional outcomes. In this article, we discuss our current technique of VIP including refinements such as Veil of Aphrodite nerve sparing using Harmonic ACE curved shears, high anterior release (super Veil), extended pelvic lymph node dissection, percutaneous suprapubic tube bladder drainage, and barbed suture for the urethrovesical anastomosis. In 2012, incorporation of the GelPoint access platform has the potential to further improve the oncologic performance of VIP, especially in high-risk patients.
Introduction
This year marks more than 12 years of the VIP technique; it is astonishing that within this short period, the unprecedented growth of robot-assisted radical prostatectomy (RARP) has seen it overtake ORP in the United States. 8 Data from recent population-based studies have also established its superiority in terms of complications and functional outcomes. 8 –10 While the VIP has come to be recognized as a standard in transperitoneal RARP, it has undergone several modifications over the years. 11,12 These include refinements such as endopelvic fascia sparing, late ligation of the dorsal venous complex (DVC), high anterior release (super Veil), extended pelvic lymph node dissection (PLND), two-layer anastomosis, 13 percutaneous suprapubic tube (PST) bladder drainage, 14 and use of a barbed suture for the anastomosis. 15 More recently, we have modified the GelPoint access port (Applied Medical, Rancho Santa Margarita, CA) to aid with prostate (organ) retrieval for pathologic examination (MORE) in high-risk patients. The description of the VIP presented in this article is our current technique, a result of the evolution of this operation over the last decade, and one that draws heavily on our experience of more than 7000 cases.
Methods
Indications and contraindications
Indications are identical to those for ORP. Patients with T3–T4 disease with or without nodal metastasis (N1) may be considered as part of a multimodal treatment strategy and constitute a highly selected population. Relative contraindications include obstructive lung disease and abnormalities of cardiac output because of difficulties in ventilation that may occur in these patients who are exposed to pneumoperitoneum and steep Trendelenberg position. Previous abdominal surgery may present difficulties but is not a contraindication. Patient factors, such as morbid obesity, large prostate, large median lobe, or surgery in the salvage setting, increase the complexity of RARP, and it should be reserved for experienced surgeons. 16
Preoperative workup
Anticoagulants and antiplatelet agents are ceased before surgery following local guidelines. Antibiotic and thromboprophylaxis are given according to hospital policy. A laxative is given the night before surgery; patients with Gleason score 8 to 10 or T3 disease are given a mechanical bowel preparation in case of rectal involvement.
Patient positioning and preparation
The patient is placed in the lithotomy position with arms secured to the sides and all pressure points protected using foam pads. The patient is fastened to the table with tape and straps. The thumbnails should face the ceiling and the arms held lax to avoid peripheral nerve compression. The legs are separated in flexion and abduction to allow the patient side-cart sufficient access. Sequential compression devices are placed on the calves. The abdomen down to the upper thighs is prepped with antiseptic and then draped. The bladder is drained with an 18F Foley catheter that is secured to the side so that the assistant can manipulate it during the operation. Intravenous fluids are limited to <1 L during surgery to reduce excessive urine production, which can obscure the view and necessitate copious suctioning.
Instrumentation
Nondisposable
• Monopolar hook
• Fenestrated bipolar forceps
• Round tip scissors
• Large needle driver
• 8-mm instrument cannula
• GORE® Suture Passer (WL Gore & Associates, Flagstaff, AZ)
Disposable
• 12×100 mm and 5×100 mm laparoscopic ports (Kii Fios First Entry port, Applied Medical, Rancho Santa Margarita, CA)
• Endopath® Veress needle (Ethicon Endo-Surgery, Blue Ash, OH)
• StrykeFlow 2 suction irrigator (Stryker, Kalamazoo, MI)
• Hem-o-Lok clips (Weck, Teleflex Medical, NC)
• 3-0 barbed polyglyconate suture (V-Loc®, Covidien, Mansfield, MA)
• No. 15 scalpel blade
• 10 mm Endopouch® bag (Ethicon Endo-Surgery, Blue Ash, OH,)
• Rutner 14F percutaneous suprapubic catheter (Cook Medical, Bloomington, IN)
• 1-0 polypropylene CT-1 needle (Ethicon, Somerville, NJ)
• 1 PDS™ CT-1 needle (Ethicon, Somerville, NJ)
• 4-0 Monocryl™ suture (Ethicon, Somerville, NJ)
• Polypropylene button (Ethicon Endo-Surgery, Blue Ash, OH)
• Mastisol® adhesive (Eloquest, Ferndale, MI)
• Steri-Strip™ (3M, St Paul, MN)
Optional
• Monopolar curved scissors
• Maryland bipolar forceps
• Harmonic™ACE curved shears
• 12×130 mm balloon port for camera (Kii Balloon Blunt Tip System, Applied Medical, Rancho Santa Margarita, CA)
• GelPoint Advanced Access Platform (Applied Medical, Rancho Santa Margarita, CA)
Surgical Steps
Port placement
We use two bedside assistants and use a six-port approach with three robotic ports and three assistant ports. The table is set to a steep Trendelenberg position and pneumoperitoneum established with a Veress needle. This is replaced with a 12-mm port for the 30-degree robotic laparoscope that is placed periumbilical and used at the end for specimen retrieval. Initial pressure is 20 mm Hg for port placement, which is then set to 15 mm Hg for the remainder of the surgery. All other ports are inserted under vision with a 30-degree lens angled upward to prevent visceral injuries and visualize the anterior abdominal wall. Robotic 8-mm ports are placed on each side approximately 3 to 5 cm below the umbilicus and lateral to the rectus. The right-side 12-mm assistant port is inserted in the midaxillary line, 2 to 3 cm cranial to the anterior superior iliac spine. There should be a handbreadth distance (∼8 cm) between these ports. Next, a 5-mm port for the sucker is inserted in the space between the right robotic port and camera port, but cranially by 3 to 5 cm. A further 5-mm port is placed on the left side in a similar position to the right-side 12-mm port.
As a rule, we place the camera port infraumbilical in taller patients (height ≥6 feet) and supraumbilical in shorter patients. The 12-mm port allows for needles and clips to be passed easily as well as removing tissue such as lymph nodes. In obese patients, a longer balloon port for the camera can prevent the port coming out during the procedure. Similarly, bariatric robotic ports should be considered in morbidly obese patients. Moreover, it is important to avoid inserting trocars through adhesions, where inadvertent bowel injury might occur. If needed, laparoscopic adhesiolysis can be performed before trocar placement. If using only a single bedside assistant, the left-side 5-mm assistant port is replaced for a robotic 8-mm port for the fourth robotic arm. Again, there should be sufficient space between these ports; otherwise, there will be clashing of instruments. If using the Harmonic ACE curved shears, the right-side robotic port should be placed 2 to 3 cm more caudal than normal to compensate for the shorter reach of this instrument.
Release of bowel
In the steep Trendelenberg position, the small bowel usually moves out of the pelvis. Often there can be adhesions between the large bowel and the peritoneum laterally. If present, these have to be released to allow PLND. Sharp dissection without energy is preferred in the setting of dense adhesions.
Development of extraperitoneal space (“bladder takedown”)
The peritoneal cavity is examined using a 30-degree–up lens. While the assistant retracts the medial umbilical ligament toward the ipsilateral shoulder, an incision is made lateral to this ligament and extended down to the vasa. Epigastric vessels are close by and should not be injured. The space of Retzius is entered and dissection proceeds in the loose areolar tissue (Fig. 1); the vertical limb of the incision is deepened inferiorly until the pubic bone is seen. The same maneuver is repeated for the opposite side. A transverse incision between the medial umbilical ligaments, high enough to avoid the bladder, converts it to a U-shape incision. With release of the bladder flap and the urachus, the whitish fibers of the transversalis fascia come into view. The bladder is mobilized caudally by following the contour of the abdominal wall inferiorly until the landmark of the pubic bone is visualized. Dissection is continued on either side to expose the endopelvic fascia.
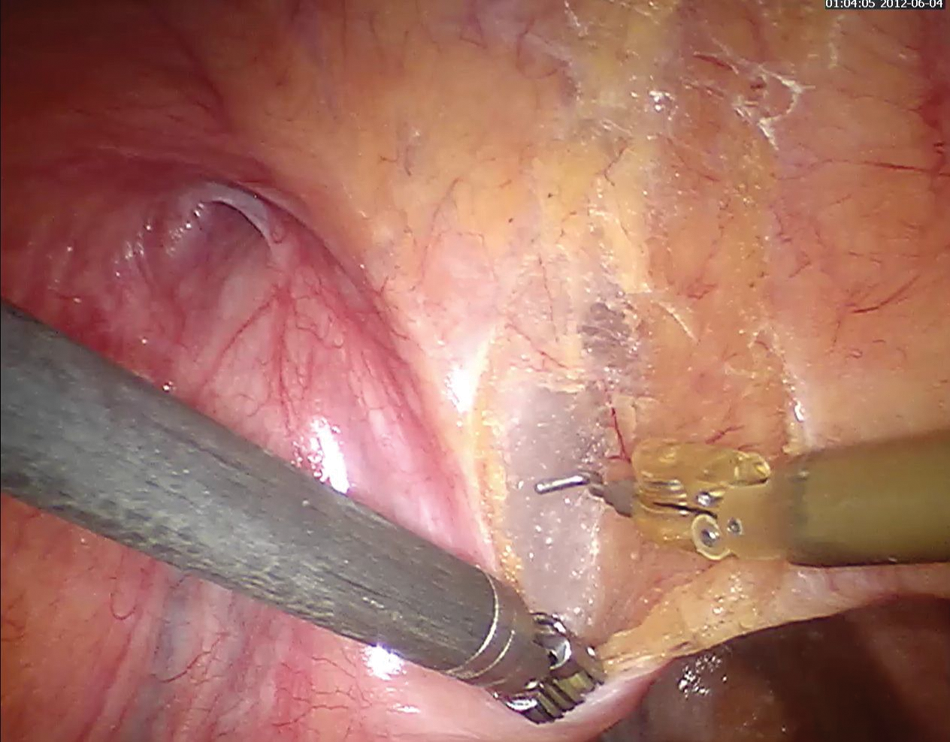
Mobilization of bladder at Vattikuti Institute prostatectomy. The vertical limb of the U-incision is lateral to the medial umbilical ligament: The dissection is performed in the avascular plane involving adipose and loose areolar tissue.
While the entire operation can be done with a 0-degree lens, we prefer a 30-degree lens for this part of the dissection, and switch to 30-degree looking down, once the bladder is down. The anastomosis is performed with the straight lens. The depth of perception, particularly for dissecting around the vessels, is greater with the 30-degree–down lens, and the risk of smudging the lens is lower.
Division of the bladder neck
The pubic bone is cleared of all fat and connective tissue. Dissection is lateral to medial to avoid avulsion of the superficial dorsal vein. The latter is coagulated carefully using bipolar cautery, after which the fat over the prostate is peeled off. Occasionally, an accessory pudendal artery may be present, and one should be careful not to damage it. We do not divide the puboprostatic ligaments.
The bladder neck is approached without releasing the endopelvic fascia or ligating the DVC. The Foley balloon is deflated and the catheter kept in the bladder. The anterior bladder wall is grasped by the right-side assistant in the midline and lifted upward. This maneuver helps in demarcating the bladder neck, as the bladder pulls away from the prostate. Another option is keeping the balloon inflated and moving the catheter backward and forward; the balloon helps identify the division between prostate and bladder. A 1-cm incision is made in the anterior bladder neck at 12 o'clock, and the incision deepened to reveal the catheter. The tip of the catheter is taken out of the bladder and given to the left-side assistant, who provides firm traction by placing it on the anterior abdominal wall. The remaining lateral fibers attaching the bladder to the prostate are now divided, and the posterior lip of the bladder neck is dissected off the prostate using electrocautery. The nearby ureteral orifices should be visualized and protected. Excessive bleeding can be a sign of being too close to the capsule of the prostate. If so, the plane of incision should be altered.
Posterior dissection of vas deferens, seminal vesicles, and Denonvilliers fascia
The anterior layer of Denonvilliers fascia is incised to expose the vasa and seminal vesicles. The vasa are then skeletonized, and the artery to the vas deferens is controlled. The vasa are transected and the cranial stump held by the right-side assistant while the proximal end is lifted upward by the left-side assistant. This helps with dissection of the seminal vesicles. The seminal vesicle artery is controlled with fine bipolar coagulation or clips. Limited use of cautery is preferred to optimize erectile function.
After the seminal vesicles are released, they are held upward by each assistant, so that the posterior prostate is retracted, revealing the longitudinal fibers of Denonvilliers fascia. A transverse incision is made in this fascia into the avascular plane between the perirectal fat and posterior prostate. Blunt dissection is used to push the rectum away from the prostate. Dissection is continued distally toward the apex and laterally. We have recently replaced the monopolar hook with the Harmonic ACE curved shears in some patients for dissection of the seminal vesicles and performing nerve sparing (veil of Aphrodite). This accounts for a subjective improvement in visibility and better hemostasis, with less energy spread to surrounding tissues. In patients with low-risk disease where potency is a priority, the tips of the seminal vesicles may be preserved.
Nerve sparing
The base of the seminal vesicle is retracted in the direction of the patient's contralateral ear by the assistant on the opposite side. The prostatic pedicle is defined and ligated using Hem-o-lok clips and bipolar coagulation. Nerve sparing may then proceed via three different methods:
Standard nerve sparing
In this, the dissection is in between the prostatic fascia on one side and the levator fascia on the other. The lateral prostatic fascia is incised anteriorly around the midprostate, and nerve sparing proceeds using cold scissors and bipolar coagulation as necessary. The posterolateral bundle opens up, and dissection is carried to the apex while staying close to the prostate capsule to prevent damage to the bundle. Smaller vessels entering the prostate can be controlled with fine bipolar coagulation or clips.
Veil of Aphrodite
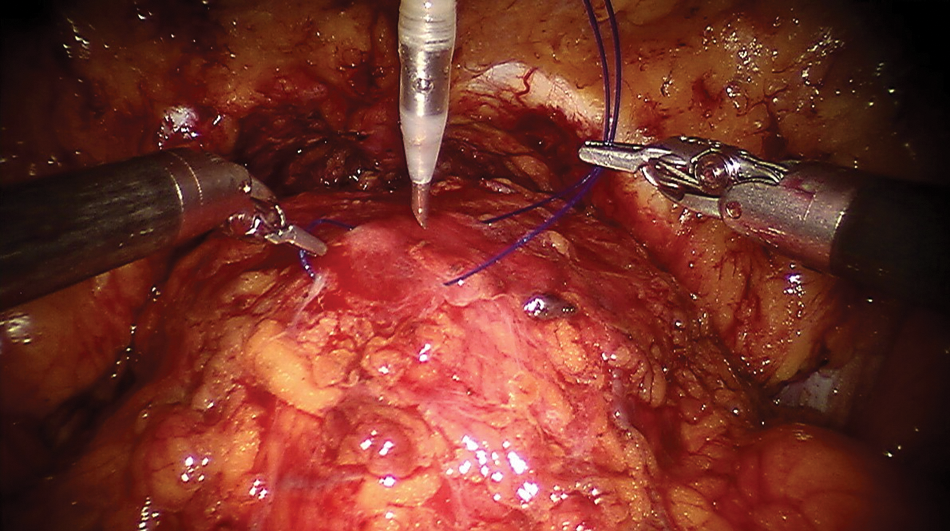
This begins by developing space between the prostatic capsule and fascia, starting at the base of the seminal vesicles. We find the curved shears of the Harmonic ACE particularly helpful for this. The plane can be developed by slowly teasing the tissues apart, deep to the venous sinuses. Interfascial dissection is performed between 1 and 5 o'clock for the right and 6 and 11 o'clock for the left. Dissection of the neurovascular bundle is performed until the entire prostatic fascia up to the pubourethral ligament is mobilized in continuity (Fig. 2). If in the correct plane, the dissection is mostly bloodless except where the fascia fuses with the puboprostatic ligament. At the end, curtains of periprostatic tissue hang from the pubourethral ligament—the veil of Aphrodite.
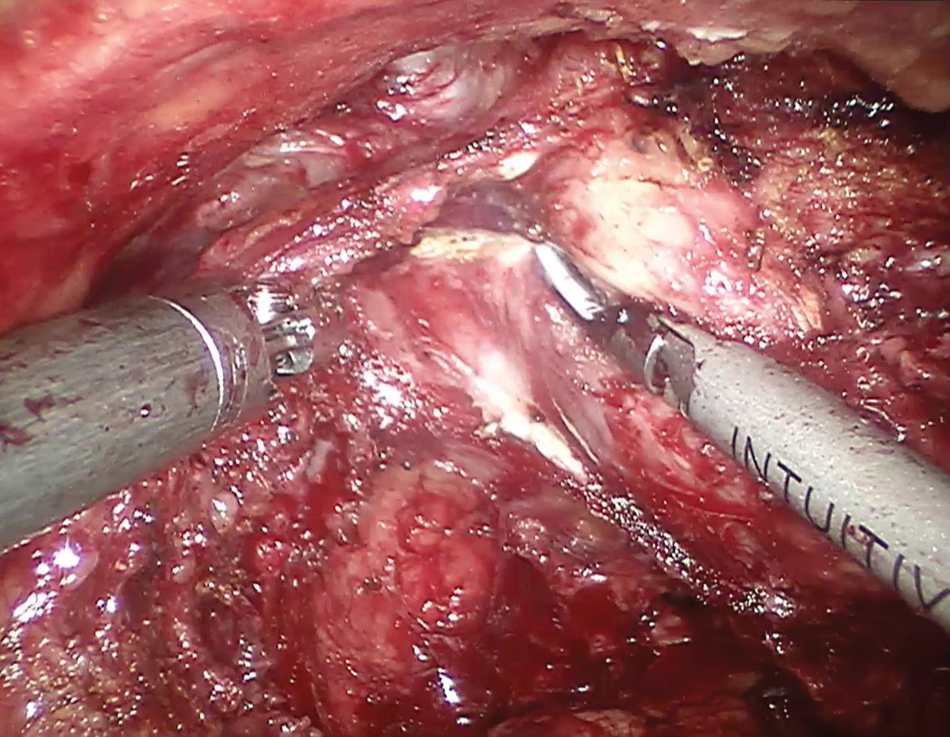
Veil of Aphrodite nerve-sparing procedure using Harmonic ACE curved shears. We find it easier to develop the veil plane using this instrument, with lower thermal spread compared with monopolar or bipolar cautery.
Super veil
Because up to a quarter of neural tissue can be identified on the anterior surface of the prostate, 17 we modified the veil to incorporate dissection extending anteriorly, whereby tissue between 11 and 1 o'clock was preserved including the pubovesical ligaments. The “super veil” procedure is slightly more challenging than the veil because this anterior surface is fibromuscular making exact separation difficult. For these reasons, we reserve this for low-risk disease patients whose priority is optimal potency.
In most cases, we use the Harmonic ACE when performing a veil or super veil procedure; we find it is easier to get into the interfascial plane with this instrument while dissection of the anterior surface for the super veil can be relatively bloodless. Furthermore, the DVC can be ligated without suturing. One drawback with the Harmonic, however, is that it lacks wristed articulation. Regardless of which instrument is used, it is important to avoid excessive traction on the neurovascular bundles during nerve sparing.
Apical dissection, urethral transection, and control of the DVC
The camera is switched to a 0-degree lens. The right assistant grasps the anterior prostate and retracts it cephalad making the DVC and urethra taut. The puboprostatic ligament and DVC are divided using cautery or the Harmonic instrument. Rotating the prostate helps with dissection and delineation of the apex laterally and posteriorly. After the apex is freed circumferentially, the urethra is dissected into the prostatic notch and transected anteriorly a few millimeters distal to this. The catheter is then withdrawn so that the posterior urethral wall is visible, which is then cut. The prostate may still be attached to the perirectal tissue by fascia. If so, this can be divided carefully with the left robotic instrument protecting the rectum. The freed prostate is placed in a 10-mm Endopouch bag.
The rectum is intimately related to the apex, and this part of the operation is at most risk of rectal injury. It helps if the anterior apical dissection is attempted only after maximal posterior dissection all the way to the apex. Bleeding from the DVC occurs during apical dissection. Because of the pneumoperitoneum, most times this is manageable. After the prostate is freed, the DVC is controlled with a running suture (2-0 V-Loc, RB-1 needle). Perineal pressure at this point helps identify all bleeding sinuses. If bleeding during apical dissection is profuse, the DVC should be controlled early so that oncologic principles are not compromised.
Pelvic lymphadenectomy
From 2008, we changed PLND in low- and intermediate-risk patients from a limited external iliac and obturator node to an internal iliac node dissection (zone 2 of Studer classification 18 ). With this approach, the % of positive nodes is significantly higher. 11 High-risk patients undergo extended PLND including external iliac, obturator, and internal iliac nodes (zones 1 and 2). The vasa are divided and the ureter identified where it crosses the bifurcation of the iliac vessels. The ureter can be followed all the way distally where it lies under the superior vesical artery. As the dissection is distal to this artery and medial to the external iliac vein, the ureter is protected. Tissue around the obturator nerve and along the lateral pelvic wall is dissected to clear the obturator fossa. All tissue from the obturator fossa to the lateral aspect of the bladder is also cleared.
Posterior reconstruction
Posterior reconstruction of Denonvilliers fascia and the rhabdosphincter is undertaken to facilitate the anastomosis and reduce any tension on it. A barbed V-Loc suture (3-0, RB-1 needle, 6 inches) is anchored by passing it through the posterior layer of Denonvilliers fascia and the far lateral aspect of the posterior bladder neck. The suture is then passed to the posterior rhabdosphincter and back to the posterior bladder neck, incorporating Denonvilliers fascia with each throw (Fig. 3). After four passes from right to left, and cinching the sutures with each throw, the bladder neck and urethral stump lie in close proximity.
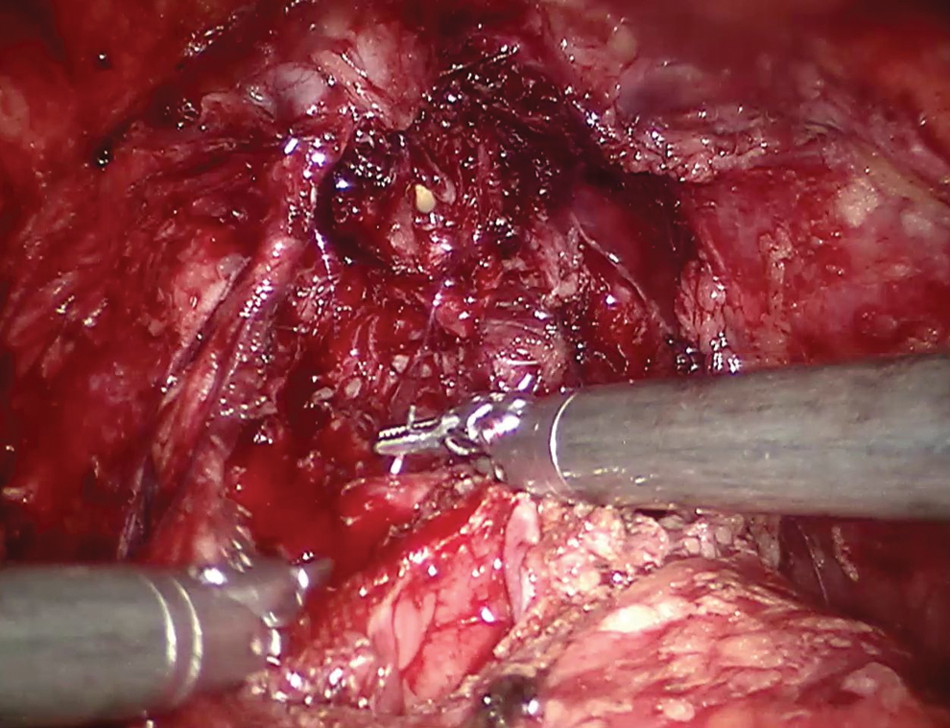
Posterior reconstruction during Vattikuti Institute prostatectomy. The barbed suture is passed through the posterior layer of Denonvilliers fascia, while making its way from the posterior rhabdosphincter to bladder neck.
Urethrovesical anastomosis (UVA)
We reported the first safety and feasibility study for using a barbed polyglyconate suture for the UVA during RARP. 15 Two 3-0 V-Locs (6-inches, RB-1 needle) are made into a double-armed stitch with a total of 11" of barbs, or 14" in larger bladder necks. The unidirectional barbs prevent slippage and therefore do not require the assistant to follow the suture. In one study, barbed suture reduced the anastomotic time without an increase in adverse events. 19 The suture starts at the 4-o'clock position on the posterior bladder wall outside-in, continuing into the urethra on the opposite site, inside-out. Once the posterior urethral wall is anastomosed to the bladder neck, the direction of the stitch is altered at 9 o'clock so as to get passage of the needle in the bladder to inside-out. The anastomosis continues until the 11-o'clock position and is stopped. The other needle is run counterclockwise from 4 to 11 o'clock (Fig. 4) while the assistant intermittently manipulates the tip of the catheter in and out of the urethra to check for inadvertent suturing of the back wall. Both arms of the suture are cinched down at 11 o'clock to complete the anastomosis; the needles are cut without tying knots. The bladder is filled with 250 mL of saline via the urethral catheter to assess for leak.
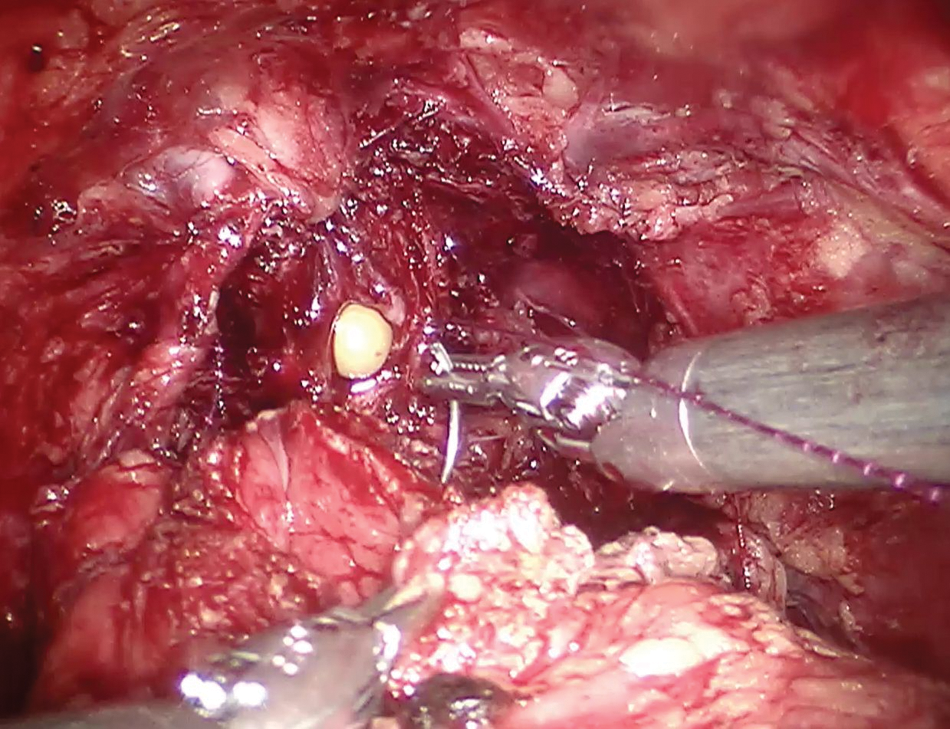
Urethrovesical anastomosis during Vattikuti Institute prostatectomy. Beginning the anastomosis with the left side of the double-armed barbed suture at 4-o'clock starting outside-in of the bladder wall.
Percutaneous suprapubic tube bladder drainage
We replaced the urethral catheter with a PST for bladder drainage more than 4 years ago, and it is now our standard of care. Advantages are greater patient comfort with no increase in the urethral stricture rate. 20 While the bladder is distended, a horizontal mattress suture (1-0 prolene, CT-1 needle) is placed through the full thickness of the anterior bladder wall. The suture serves to anchor the bladder to the abdominal wall and is brought outside to the abdominal skin using a GORE suture passer. Under robotic visualization, a 14F Rutner suprapubic catheter is percutaneously placed in the midline approximately one-third of the distance between the pubic symphysis to the umbilicus. Upward traction on the bladder sutures with robotic needle drivers tents the bladder wall, allowing the assistant to insert the needle obturator through the bladder between the sutures (Fig. 5). Immediate drainage of fluid indicates proper passage of the catheter. The PST is secured by inflating its balloon with 4 mL of sterile water.
Guided placement of the percutaneous suprapubic catheter under vision. The needle obturator is inserted into the distended bladder between the two limbs of the suture under direct robotic visualization.
Specimen retrieval and closure
The bagged specimen is retrieved by extending the camera port incision. After evacuating pneumoperitoneum, dedocking the robot, and moving to the supine position, the external sutures of the PST are pulled and fixed to the skin over a sterile plastic button, thereby bringing the cystotomy toward the anterior abdominal wall. The tails of the suture are wrapped around the tube with adhesive (Mastisol) and Steri-Strip. Fascia is closed with two interrupted 1 PDS sutures in a figure-of-eight. Skin is closed with subcuticular stitches.
MORE
One criticism of RARP has been the lack of tactile sensation, which might compromise surgical margin rates.
21,22
To address this issue, in early 2011, we incorporated the GelPoint access port with the VIP technique, because this has allowed us to modify retrieval of the whole prostate at an earlier stage of the operation for pathologic examination (
Postoperative care
A saline bolus is administered in the recovery room. Medications for pain control include intravenous ketorolac and oral acetaminophen with codeine. We avoid morphine because it can lead to ileus. A clear liquid diet is started immediately and advanced to a soft diet the following day. Patients are encouraged to mobilize within 6 hours to minimize thromboembolic complications and encourage bowel motility. Blood for routine tests is not drawn. Patients are discharged within 24 hours. Patients with a PST are instructed to clamp the catheter on postoperative day 5 and record postvoid residuals. If <50 mL per void, the catheter can be removed on postoperative day 7.
Management of intraoperative complications
Intraoperative complications include bleeding and injury to adjacent organs. Small bowel injury may occur during adhesiolysis or as a result of instrument passage, and can be closed robotically in two layers. Rectal injury is a concern in patients with T3 to T4 disease, or history of radiation therapy or cryotherapy. Most injuries occur posterolaterally, close to the apex. If dissection is difficult, sharp dissection is preferred. In cases of small rectal tears, primary closure can be performed in two layers using the barbed suture. If the rectal suture and the urethrovesical anastomosis are watertight, a colostomy is not necessary. After instituting broad-spectrum intravenous antibiotics and a clear liquid diet, the majority of patients can be discharged within 72 hours. 23 Ureteral injury is a rare complication and may occur during extended PLND or during posterior dissection. It can be repaired primarily or with a ureteral reimplantation if very low; both can be performed robotically.
Management of postoperative complications
Deep venous thrombosis should be managed with anticoagulation. The patient may present with symptomatic lymphoceles in the first few weeks after lymphadenectomy with fever, pain, or leg swelling. This is managed by placing a percutaneous drain. Bladder neck contractures are rare and can usually be managed with office dilation. Incisional hernias are also a rare occurrence. We use dilating trocars, which contributes to a lower incidence of port site hernias.
Summary of Results
For a comprehensive analysis of complications after RARP, the reader is referred to the study by Agarwal and coworkers. 24 In 3317 patients undergoing RARP (median follow-up 24 months), the overall complication rate was 9.8%. Surgical complications occurred in 8% of patients, of which a third were Clavien grade III to V. 24 Functional outcomes have been detailed in previous publications. 11,13,25 –27 More recently, we evaluated continence in patients undergoing the PST technique; at 1 year, 86.4% had total urinary control with only 2.7% of men needing >1 pad/d. 20 The median time to 0 to 1 pad/d and total urinary control were 2 and 6 weeks, respectively. Erectile function outcomes are assessed using Sexual Health Inventory for Men (SHIM) questionnaires. Independent predictors include the level of nerve sparing, preoperative SHIM score, and patient age. 28 In a previous study of patients undergoing super veil with a preoperative SHIM >17, 42% had SHIM scores between 18 and 25, 19% had SHIM 12 to 17, 14% had SHIM 8 to 11, and 25% had SHIM <7 at 18 months follow-up. 11
Table 1 demonstrates the biochemical recurrence (BCR) rates after RARP in individual case series. In all but two series, the median follow-up is less than 2 years, and in only two is the follow-up more than 5 years. 29,30 In the most detailed report, the median time to BCR was 20 months—65% occurring within 3 years and 86.2% by 5 years. 29 This suggests that the shorter follow-up recorded in other series may not underestimate BCR, and indeed that cancer control with RARP is not inferior to that achieved with open surgery.
Mean not median.
30-month data.
BCR=biochemical recurrence rate; PSA=prostate-specific antigen; FU=follow-up.
Footnotes
Acknowledgment
Khurshid R. Ghani is supported by a Fellowship from The Urology Foundation, United Kingdom.
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.