
Abstract
Background and Purpose:
Laparoscopic and robot-assisted partial nephrectomy (LPN and RPN) are common minimally invasive alternatives to open partial nephrectomy (OPN) for management of renal tumors. Cost discrepancies of these approaches warrants evaluation. We compared hospital costs associated with RPN, LPN, and OPN.
Patients and Methods:
Costs were captured for 25 patients in each group who underwent RPN, LPN, or OPN at our institution between November 2008 and September 2010. Variable costs included operating room (OR) time, supplies, anesthesia, and inpatient care costs. Fixed costs included equipment purchase and maintenance. Impact of variable and fixed costs were estimated using sensitivity analysis.
Results:
Overall variable costs were similar for RPN, LPN, and OPN ($6375 vs $6075 vs $5774, P=0.117, respectively). OR supplies contributed a greater cost for RPN and LPN than OPN ($2179 vs $1987 vs $181, P<0.0001, respectively), while inpatient stay costs were higher for OPN compared with LPN and RPN ($2418 vs $1305 vs $1274, P<0.0001, respectively). Sensitivity analysis of variable costs demonstrates that RPN and LPN can represent less costly alternatives to OPN if hospital stay for RPN and LPN is ≤2 days and OR time <195 and 224 minutes, respectively. Inclusion of fixed costs made OPN less expensive than LPN and RPN unless use of the robot increases and operative times are reduced.
Conclusion:
By minimizing OR time and hospital stay, RPN and LPN can be cost equivalent to OPN regarding variable costs. When including fixed costs, RPN and LPN were more costly than OPN, but equivalence may be possible with improvements in efficiency.
Introduction
Despite growing evidence for the clinical effectiveness of minimally invasive approaches to PN, few groups have compared costs of these approaches with those of OPN. 11 –17 As the use of these new surgical technologies increases, it is important to understand their economic implications. We compared variable and fixed hospital costs for RPN, LPN, and OPN at an academic medical center to better understand the drivers of overall costs and identify possible strategies to minimize costs.
Patients and Methods
After obtaining Institutional Review Board approval, the last 25 patients in each of the respective groups to undergo RPN, LPN, or OPN at our institution were identified. We excluded patients who underwent additional concomitant surgery, such as multiple kidney tumor resections, partial hepatectomy, distal pancreatectomy, and/or cholecystectomy. All of the RPNs and LPNs were performed by one surgeon with 5 years of experience as an attending. The OPNs were performed by five different surgeons, with between 6 and 30 years of experience. Individual direct hospital costs, not charges, were obtained from our Business Planning and Decision Support office. Costs were divided into variable and fixed costs. Variable costs were unique to each patient and included those for operating room (OR) time, supplies, anesthesia, postanesthesia care unit, inpatient care, radiology, pharmacy, laboratory, and blood bank charges. Fixed costs included the capital acquisition of laparoscopic and robotic systems and maintenance charges for the equipment, and were distributed among the patients, depending on use.The costs of the minimally invasive equipment (robotic and laparoscopic) were estimated and amortized over 7 years. No fixed costs were included for open surgical patients because all OR and equipment costs were more than 7 years old.
Surgical supplies varied according to approach. The OPN group was approached using a thoracoabdominal incision in 13 (52%) cases and a flank incision in 12 (48%) cases. Cold ischemia was used during tumor excision, and the resection bed was closed primarily without the use of hemostatic agents. The laparoscopic approach used standard laparoscopic instruments to induce warm ischemia, and the kidney defect was closed using tissue sealant and cellulose rolled bolsters. Disposable instruments included a 5-mm bipolar laparoscopic sealant device on all cases, and three of the LPN cases necessitated hand assistance for reconstruction during heminephrectomy. All RPN used a three-arm approach. Robotic instruments were consistent across all cases using one curved endoshears, one fenestrated bipolar grasper, and one needle driver. After resection and closure of the collecting system and obvious end arteries using a running 3-0 barbed suture (V-loc, Covidien Inc), the cortical tissue was closed primarily using a sliding clip renorrhaphy technique. 18,19 No tissue sealant or bolsters were used during the robotic cases.
Clinical data were collected retrospectively to include patient demographics (age, sex, body mass index, American Society of Anesthesiologists score), tumor characteristics (side, size, R.E.N.A.L. [radius; exophytic/endophytic; nearness; anterior/posterior; location] score), operative parameters (OR time, clamp time, estimated blood loss [EBL]), and length of hospital stay (LOS). All R.E.N.A.L. scores were determined by a single fellowship trained expert in abdominal radiology. All patients were discharged when tolerating a regular diet and ambulating, and pain was well tolerated using an oral analgesic.
Statistics
Surgical approaches were compared for each cost category using the Kruskall-Wallis estimate. For significant differences between all three surgical approaches, post hoc pairwise analysis was conducted using the Tukey test with P<0.05 considered statistically significant. (StatCrunch, Pearson Education,
Results
Patient demographics and perioperative outcomes
Table 1 summarizes our patient demographics and perioperative outcomes. Differences were found between RPN, LPN, and OPN in regard to age, EBL, and LOS. Post-hoc analysis demonstrated that OPN patients were older than LPN patients (mean 61.9 vs 53.5 years, P<0.05, had greater EBL than LPN patients (275.4 vs 154 mL, P<0.05), and LOS was significantly longer than LPN and RPN (4.6 vs 2.48 vs 2.72 days, P<0.05, respectively). Readmissions were similiar between the groups with three readmissions for OPN (fever, ileus, postoperative bleed), two for RPN (syncope, pain), and two for LPN (chest pain, hematuria).
Significantly different on post hoc pairwise analysis (P<0.05).
LOS significantly longer for OPN vs LPN and RPN on post hoc analysis (P<0.05). No signficant difference between LPN and RPN.
R.E.N.A.L.=radius; exophytic/endophytic; nearness; anterior/posterior; location; BMI=body mass index; ASA=American Society of Anesthesiologists; OR=operating room; EBL=estimated blood loss; LOS=length of stay; OPN=open partial nephrectomy; LPN=laparoscopic partial nephrectomy; RPN=robot-assisted partial nephrectomy.
Variable costs
Figure 1 and Table 2 summarize the total direct hospital expenditures by type of cost. Overall variable costs were similar between all three surgical approaches (P=0.117), although there was a trend toward higher overall costs in the minimally invasive groups. Costs of OR supplies were greatest for RPN followed by LPN, and lowest in OPN (P<0.05). The cost of hospital stay was greater in OPN when compared with both RPN and LPN, as were costs for other charges including pharmacy, radiology, laboratory, and other (P<0.05).
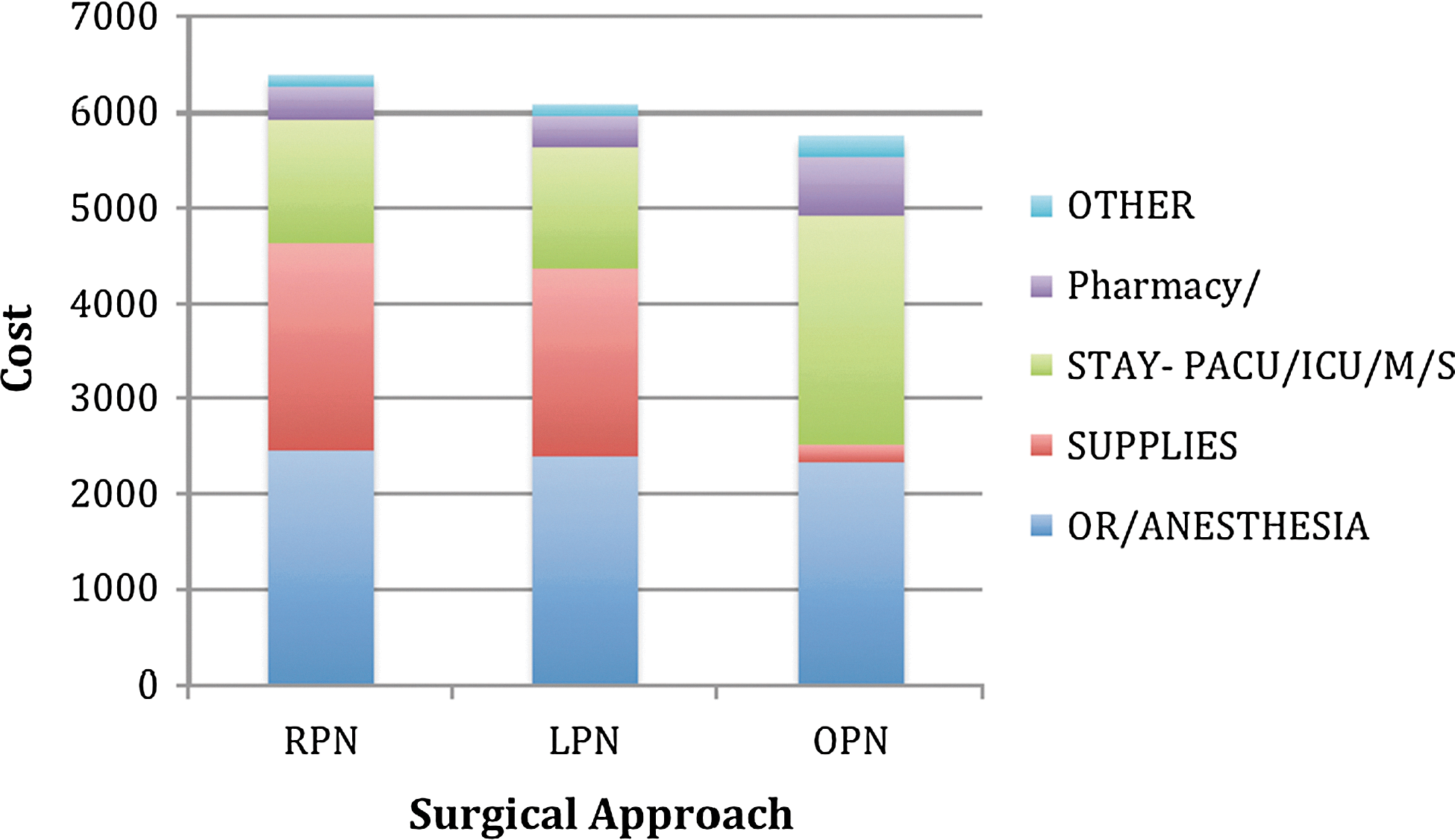
Variable costs of robot-assisted partial nephrectomy (RPN), laparoscopic partial nephrectomy (LPN), and open partial nephrectomy (OPN) by individual categories. PACU=postanesthesia care unit; ICU=intensive care unit; M=medical; S=surgical; OR=operating room.
Costs were lower on post hoc analysis for OPN vs LPN and RPN (P<0.05). No significant difference for LPN vs RPN.
Costs were greater on post hoc analysis for OPN vs LPN and RPN (P<0.05). No significant difference for LPN vs RPN.
OR=operating room; pharm=pharmacy; rad=radiology; lab=laboratory; OPN=open partial nephrectomy; LPN=laparoscopic partial nephrectomy; RPN=robot-assisted partial nephrectomy.
Multiway sensitivity analyses were performed on the variable costs only, not including fixed costs, to evaluate the impact of varying OR time and LOS for LPN and RPN, to achieve cost equivalence to average values of OPN (OR time and LOS not varied) (Fig. 2). For RPN to achieve cost equivalence to OPN, OR time would need to be less than 195 minutes, 146 minutes, and 96 minutes, for hospital stays of 2, 3, or 4 days, respectively. For LPN to be cost equivalent to OPN, OR time would need to be less than 224 minutes, 180 minutes, and 136 minutes for a hospital stay of 2, 3, or 4 days, respectively.
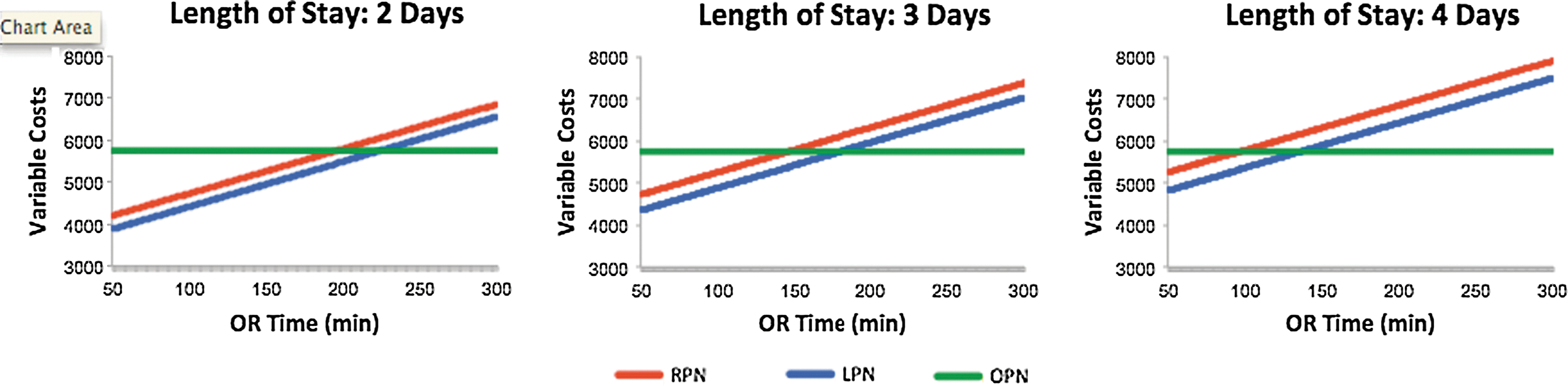
Sensitivity analysis of length of stay and operating room (OR) time (x axis) on cost per case (y axis). Variable costs only; fixed costs of equipment are not included.
Fixed costs
Costs of the robotic system (including $1,650,000 approximate purchase fee and $149,000 yearly maintenance) totaled $3,008,959.80 when amortized over 7 years, with a monthly cost of $23,320.95. Fixed costs of LPN included one million dollars for a minimally invasive surgery suite plus $40,000 in equipment costs incurred during development of our laparoscopic urology program, totaling $1,234,738.68 when amortized over 7 years, with a monthly cost of $14,699.27. We did not include laparoscopic equipment costs into robotic fixed costs because our robotic system is used in a standard OR, not a minimally invasive suite. Figure 3 demonstrates the additional fixed costs per case depending on the surgical volume and, as demonstrated, increasing use from a low to high volume setting decreases the fixed cost per case significantly.
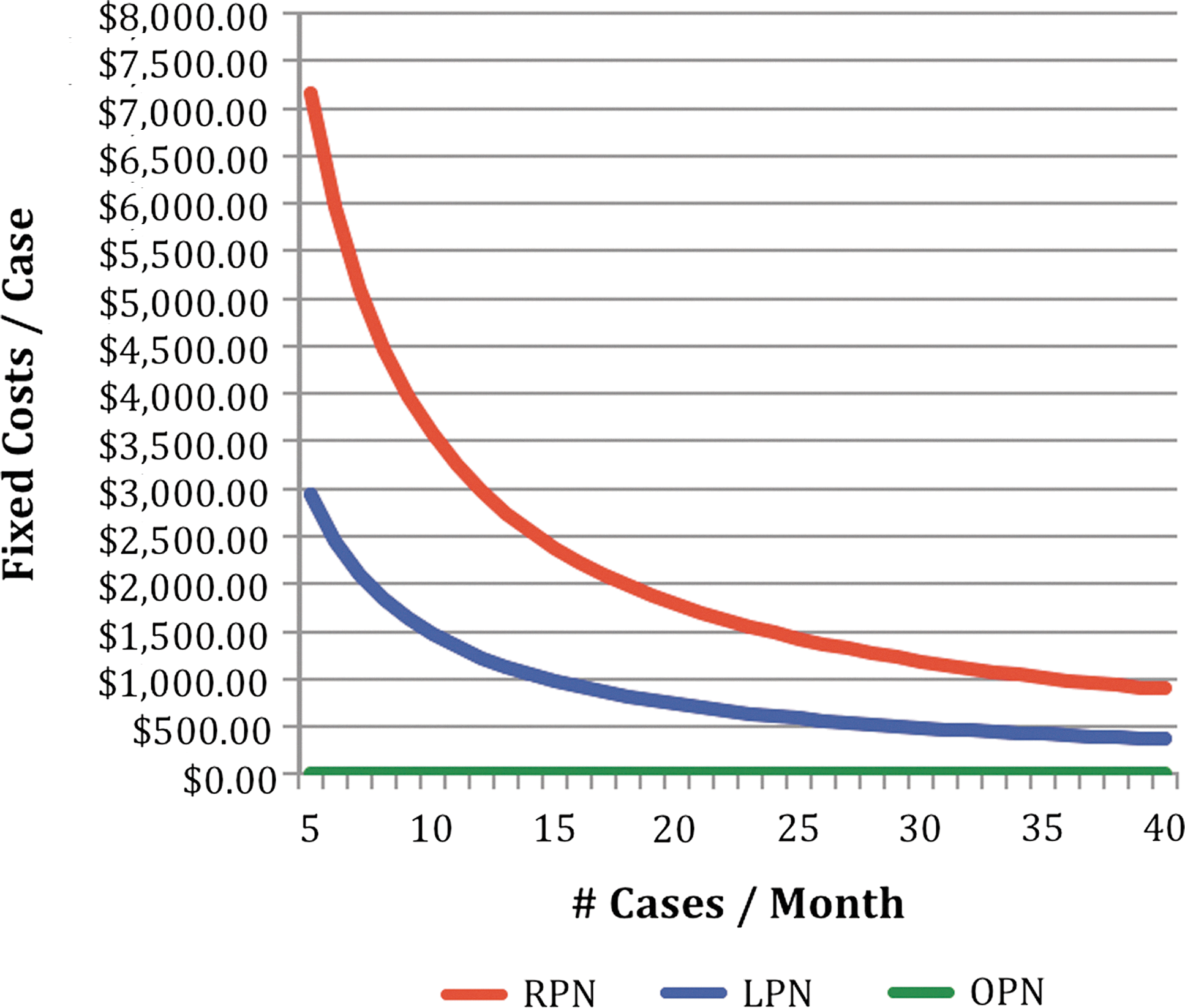
Fixed costs per case varying by number of cases per month. RPN=robot-assisted partial nephrectomy; LPN=laparoscopic partial nephrectomy; OPN=open partial nephrectomy.
Total costs (variable and fixed costs)
Figure 4 is a multiway sensitivity analysis identifying the lowest cost procedure as a function of OR time and number of cases performed monthly. We used the average LOS for each procedure to create a realistic scenario. The shaded green area to the right represents situations when OPN is the most cost effective. The shaded blue or red areas to the left indicate when LPN or RPN is the most cost effective. For example, using an OR time of 180 minutes for comparison, OPN would be more cost effective than LPN unless the overall case volume was more than 18 cases per month (Fig. 4A). For this OR time, RPN would never be less costly than OPN (Fig. 4B). If an OR time of 120 minutes was assumed, RPN would only be less costly than OPN if monthly case volume exceeded 42 cases per month. LPN is always less costly than RPN, so that comparison is not shown.
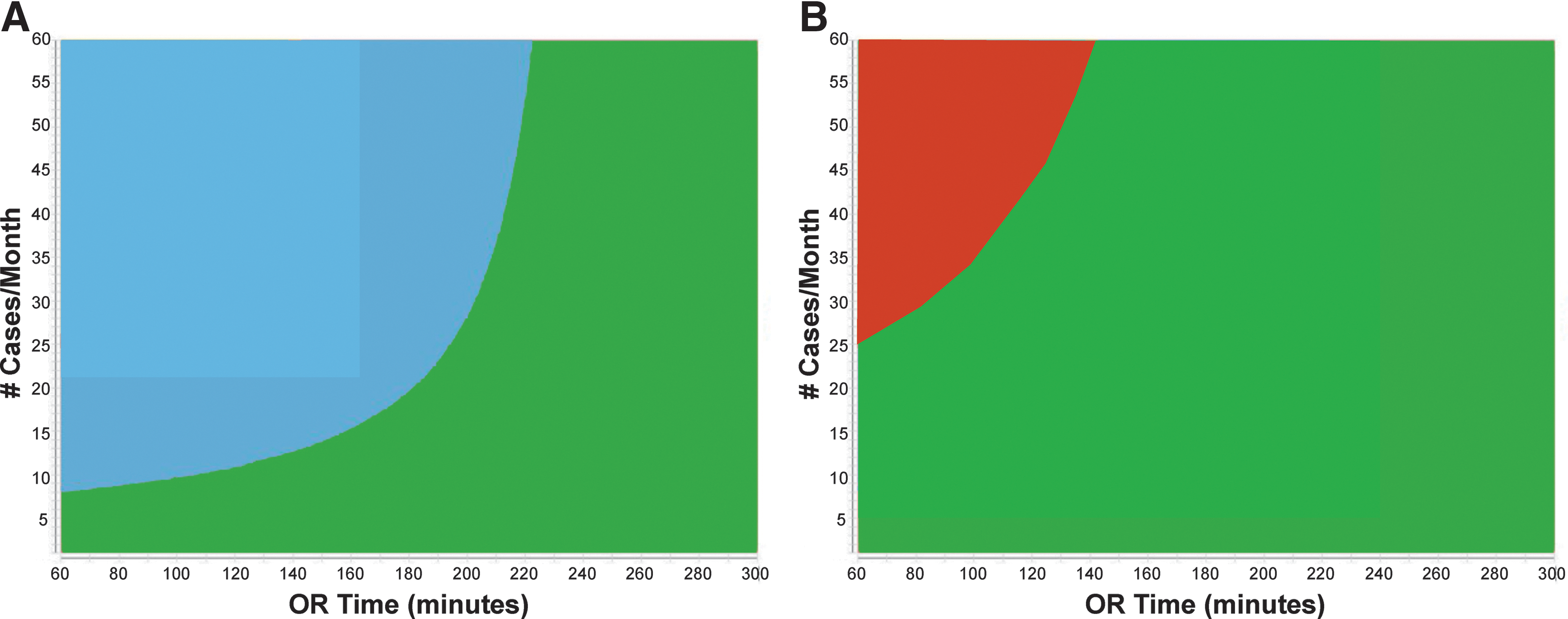
Multiway sensitivity analysis identifying the lowest cost procedure as a function of operating room (OR) time and number of cases monthly. Average length of stay was used for each procedure. Laparoscopic as always cheaper than Robotic partial therefore that comparison is not shown.
Discussion
We compared direct costs of RPN, LPN and OPN, including variable (OR time, supplies, anesthesia, and inpatient care costs) and fixed (robotic and laparoscopic equipment purchase and maintenance) costs at our institution. We found little actual differences in overall variable costs for RPN, LPN, and OPN. The inclusion of fixed costs, however, did result in greater total costs in the RPN and LPN groups. Fixed costs for LPN and RPN can be reduced by decreasing the LOS, OR time, or increasing use of equipment (across different procedures and specialties).
Another way to decrease RPN and LPN costs is to streamline surgical supply costs, as has been demonstrated in studies evaluating robot-assisted radical prostatectomy. 20,21 There was little actual difference in the supply costs between LPN and RPN, probably because of the relatively high costs of disposable laparoscopic equipment, such as absorbable laparoscopic clips, fibrin and thrombin-based products, and laparoscopic sealing/cutting instruments. One particularly expensive disposable, which was only used in three LPN cases, is the hand port assistance device. Many surgeons use this technology to help bridge their progression from the open to the minimally invasive approach, adding $500 to $700 per case. Regular use of a hand port in our series would have made the LPN supply costs and overall variable costs greater than RPN.
Minimizing use of the robot to three arms and using only those robotic instruments that are truly necessary provides opportunity for cost savings during RPN. The robotic approach can be safely and efficiently performed using three arms and three instruments per case, avoiding the additional costs of draping and providing an instrument for the fourth robotic arm. Other technical differences can account for some of the observed differences in costs; for example, we used tissue sealant in the LPN group only and no sealants or bolsters in the RPN or OPN groups.
Sensitivity analysis was performed to investigate opportunities for cost savings among the variable costs. As expected, hospital stay costs were higher in the OPN group because of longer inpatient stays; of note, our LOS was consistent with other reports of recovery from OPN. 16 We found that cost equivalence of RPN to OPN was possible if operative time was under 195 minutes for a hospital stay of 2 days, and some experienced centers have been able to achieve such outcomes. 4,22 Our variable cost findings are in agreement with a recent cost analysis that was based on averaged data modeled for OPN, LPN, and RPN. 16 Our study, however, uses actual costs occurring during cases, not model estimations, which might make for a more realistic comparison and one that can be used by other programs to base cost expectations during programmatic planning.
Although evaluating variable costs is a useful exercise, the true measurable costs incurred by an institution include both variable and fixed costs. Fixed costs are amortized over 7 years, which is the typical depreciation rate for capital equipment. We also included laparoscopic equipment costs in our analyis. While not all hospitals invest in minimally invasive suites, nor does laparoscopic surgery need one of these suites, at our institution, most of the laparosopic procedures are performed in minimally invasive operating suites and they do involve a major investment by the institution. We believe the inclusion of these costs gives a more realistic picture of costs incurred for these procedures.
By increasing case volume, these costs are spread out over more individual cases, resulting in a lower fixed cost per case. For example, if a low volume institution performs 10 cases per month and robotic equipment and maintenance is $23,320 per month, then the fixed cost per case is $2332. If 40 cases are performed per month, then the fixed cost becomes $583 per case (Fig. 3) Based on our sensitivity analysis (Fig. 4), it is possible to make up for the increased supply costs of RPN and LPN by decreasing LOS and OR time, and increasing case volume. Mir and associates 16 found similar trends suggesting PN costs can be equivalent when robotic costs come down with either increased volume or decreased equipment costs.
We found overall costs for RPN to always be more than LPN when variable and fixed cost parameters were simultaneously varied (Figs. 2 and 4). That is, unless RPN operative times or LOS become significantly lower than LPN, then RPN will always be more costly because of the increased fixed costs of robotic equipment. Lower robotic equipment costs would mitigate this difference in the future. It remains to be seen whether the robotic platform offers a shorter learning curve for minimally invasive PN than the standard laparoscopic approach; however, it has been suggested that RPN affords easier dissection and suturing than LPN, 4 allowing an easier transition to minimally invasive PN. At this point, the safety profile and outcomes of each technique, like that of radical prostatectomy, likely depends more on surgeon expertise rather than actual approach per se. There are situations when both LPN and RPN can become less costly than OPN (Fig. 4); however, without adequate volume, it would be challenging for a program to achieve the lower OR times necessary for the cost equivalence that is demonstrated in Figure 4.
We did not factor in the costs of postoperative complications into our analysis, although the actual complication rate was similar among all three groups (data not shown). Others have suggested an increase in complication rate with minimally invasive PN 7 ; however, our experience does not support those conclusions, and our readmission rate was three, two, and two for OPN, LPN, and RPN, respectively. A recent study using Markov modeling to evaluate long-term cost-effectiveness of managing small renal masses found that LPN was the most cost-effective approach when compared with OPN or percutaneous ablation for healthy patients younger than 74 years (RPN was not included in this analysis). 11 Evaluating actual societal savings realized by shorter convalescence in the outpatient setting from minimally invasive surgery is worthy of future study.
Limitations of our study include its single institution, retrospective design. RPN patients had smaller tumors with a slightly lower R.E.N.A.L. nephrometry score suggesting less complicated tumors, raising the possibility of selection bias. Notably, we did not see a difference in OR time and EBL—other potential surrogates for operative difficulty. Individual surgeons and institutions have different surgical techniques and clinical care pathways, resulting in variable use of disposable equipment and hospital resources, likely resulting in different costs.
Our study was based at a single academic institution, and thus costs may not be applicable to the community setting, where daily hospital costs are less, but surgical volume is lower. This relationship has been described by others investigating the role of robot-assisted radical prostatectomy in the community compared with tertiary settings. 23 It is important to stress that although we have performed a thorough overview of costs associated with these three procedures, given the particulars of our surgeons and cost structures, the actual costs are specific to our institution. In addition, our results need to be interpreted in the context of the reimbursement and cost structure in the United States and therefore may not be applicable to other countries. Also, the lack of significance in overall hospital costs seen between the groups may be from the study being underpowered to detect small differences.
Conclusion
Overall variable costs did not differ significantly between RPN, LPN, and OPN. Inclusion of the fixed costs of acquisition of the robotic and laparoscopic systems make RPN and LPN more expensive than OPN. Overall costs of minimally invasive surgery can be limited by reducing the use of disposable equipment, shortening LOS, reducing OR time, and increasing surgical volume. Use of the minimally invasive equipment is an important variable, and therefore only high-volume programs may be able to achieve cost equivalence to OPN. Our results can be used as a guide to evaluate further cost saving methods, and further work should focus on multi-institutional evaluation of costs and evaluation of societal cost differences from quicker convalescence after RPN and LPN.
Footnotes
Acknowledgments
This project was supported by a joint Developmental Award from the Dana Farber/Harvard Cancer Center Kidney Cancer SPORE and the Kidney Cancer Association.
Disclosure Statement
Dr. Wagner has served as a teaching proctor for Intuitive Surgical. For all other authors, no competing financial interests exist.