
Abstract
Background and Purpose:
During partial nephrectomy (PN), artery-only (AO) occlusion may mitigate ischemia/reperfusion injury because of retrograde venous flow. Using digital light processing-hyperspectral imaging (DLP®-HSI), we compared renal oxygenation during AO vs artery and vein (AV) occlusion in patients undergoing PN.
Patients and Methods:
Thirty-seven patients who were undergoing complex open PN (median R.E.N.A.L. nephrometry of 8) at our institution underwent renal oxygenation assessment using DLP-HSI. Percent renal parenchymal oxyhemoglobin (%HbO2) during AO vs AV occlusion was recorded and its correlation with postoperative estimated glomerular filtration rate (eGFR) was investigated using Pearson correlation. AO and AV occlusion was performed in 12 and 25 patients, respectively.
Results:
Comparing AO vs AV, mean ischemia time was 41 vs 35 minutes (P=0.02). The %HbO2 at baseline was 73.6% vs 71% (P=0.23). After hilar occlusion, %HbO2 quickly reached an “ischemic plateau” in both groups, with mean ischemic %HbO2 measures of 59.7% vs 62.2% (P=0.19). In the AV group, a lower mean ischemic %HbO2 was associated with lower eGFR at the most recent follow-up (r=0.46, P=0.02) and remained significant on multivariable analysis (odds ratio 2.31; 95% confidence interval 0.29–4.32; P=0.03).
Conclusions:
In this pilot clinical study, renal oxygenation profiles during PN as assessed by DLP-HSI were similar for AO vs AV occlusion. Significant retrograde venous oxygen delivery using an AO occlusion technique could not be demonstrated. There was also no renal functional advantage for AO occlusion in this population of difficult PN where prolonged ischemia times may have mitigated any advantage. Further study in cases with shorter ischemia times is warranted.
Introduction
Animal studies have suggested that renal artery-only (AO) occlusion during PN results in higher tolerance to ischemia than renal artery and vein (AV) occlusion. 1,2 In persons undergoing laparoscopic PN with warm ischemia, AO occlusion has also resulted in better postoperative renal function. 3 The protective mechanism of AO occlusion is unknown, although retrograde venous perfusion is thought to play a possible role by improving renal oxygenation during the ischemic interval. In a pilot study, using digital light processing-hyperspectral imaging (DLP®-HSI) technology in a porcine model, Tracy and associates 4 demonstrated that AO occluded kidneys had a higher percentage of oxyhemoglobin (%HbO2) between 16 and 24 minutes of renal ischemia, suggesting a possible ischemic window when AO occlusion could provide a protective benefit compared with AV occlusion. The present study evaluates whether this finding applies to humans undergoing open PN.
Patients and Methods
On approval from our Institutional Review Board, 37 consecutive patients undergoing open PN between March 2009 and July 2011 prospectively underwent intraoperative renal oxygenation measurement using DLP-HSI technology as described previously. 5,6 Each participant signed an informed consent.
Indication for PN in each case was an enhancing renal mass seen on CT or MRI that was worrisome for malignancy. Patients were not deemed candidates for laparoscopic or robot-assisted surgery because of tumor size or location. The type of vascular occlusion performed (AO vs AV) was at the discretion of the treating surgeon. Patient demographics, clinical characteristics, and perioperative outcomes were recorded in a prospectively maintained database. R.E.N.A.L. (radius; exophytic/endophytic; nearness; anterior/posterior; location) nephrometry score 7 was assigned by two urologists who were blinded to surgical modalities and outcomes.
PN was performed via a retroperitoneal flank approach in the standard fashion. Briefly, the kidney and investing Gerota fascia were fully mobilized and the renal hilum was isolated. The Gerota fascia was then opened and the tumor was exposed. Vascular occlusion by AO (n=12) or AV (n=25) clamping was performed at the surgeon's discretion, and the kidney was cooled during the first 7 to 10 minutes of ischemia using ice slush. The tumor was then excised sharply and the renal defect repaired.
DLP-HSI assessment of renal oxygenation was performed before vascular occlusion (baseline), at several intervals during ischemia, and after renal reperfusion. As previously described, 5 this system registers relative percentage of %HbO2 by recording reflectance spectra from the tissue surface after illumination with a predefined spectrum of light (in this case, the characteristic reflectance range of oxy- and deoxyhemoglobin, 520–645 nm) and delivering a real-time, color-coded map of the tissue surface oxygenation. From this image, a representative 81 pixel-square region is selected as an “optical biopsy,” and %HbO2 of this region is determined using a customized algorithm. Several recordings of %HbO2 were obtained during each of the time intervals specified above, and mean %HbO2 values at baseline, during ischemia, and during reperfusion were recorded for each patient. Images are taken with the room lights switched off momentarily to avoid interference with the visible spectrum of light. Image capture takes less than 2 seconds; thus, the impact on ischemia time is negligible.
Statistical analysis
Demographic and perioperative outcomes were analyzed using independent-samples t test for continuous variables and chi-square for categorical variables. Mean %HbO2 and estimated glomerular filtration rate (eGFR) as estimated using the Chronic Kidney Disease Epidemiology Collaboration equation 8 were compared between cohorts using the independent-samples t test. Association between %HbO2 and eGFR were investigated using the Pearson correlation. Multivariable linear regression was used to quantify independent predictors of eGFR. All statistical tests were two-sided, and statistical significance was set at P≤0.05. Analyses were performed with SPSS v.13.0 (SPSS Inc, Chicago, IL).
Results
Table 1 summarizes perioperative variables and patient and tumor characteristics. Patients in the AO group had significantly longer ischemia times. While the AO cohort had larger masses, the mean R.E.N.A.L. nephrometry scores were the same. All other baseline patient characteristics and perioperative outcomes were similar.
Postoperative Hct: Hct of patients >18 hours and <24 hours after surgery end time.
AV=artery and vein; AO=artery-only; SD=standard deviation; Hct=hematocrit.
Figure 1 displays representative color-coded renal oxygenation maps. Baseline %HbO2 in the AO vs AV group was 73.6% and 71%, respectively (P=0.23). Respective mean %HbO2 during ischemia were 59.7% vs 62.2% (P=0.19) and were significantly lower than baseline values in both cohorts (P<0.001). %HbO2 for the AO and AV groups decreased by 14.5% (P=0.001) and 15.2% (P<0.001), respectively (Fig. 2). There was no statistically significant difference between the groups in mean %HbO2 at any of the time points sampled (Fig. 2). A small nonsignificant rise in nadir %HbO2 was observed beyond 45 minutes of vascular occlusion (P=0.18) (Fig. 2). Four patients in the AO group and one patient in the AV group had ischemia times >45 minutes. The %HbO2 during ischemia in this subgroup fell below plateau levels after 45 minutes (P=0.023). After reperfusion, %HbO2 returned to near baseline levels within 3.6 minutes in the AO group and 5.8 minutes in the AV group (Table 2).
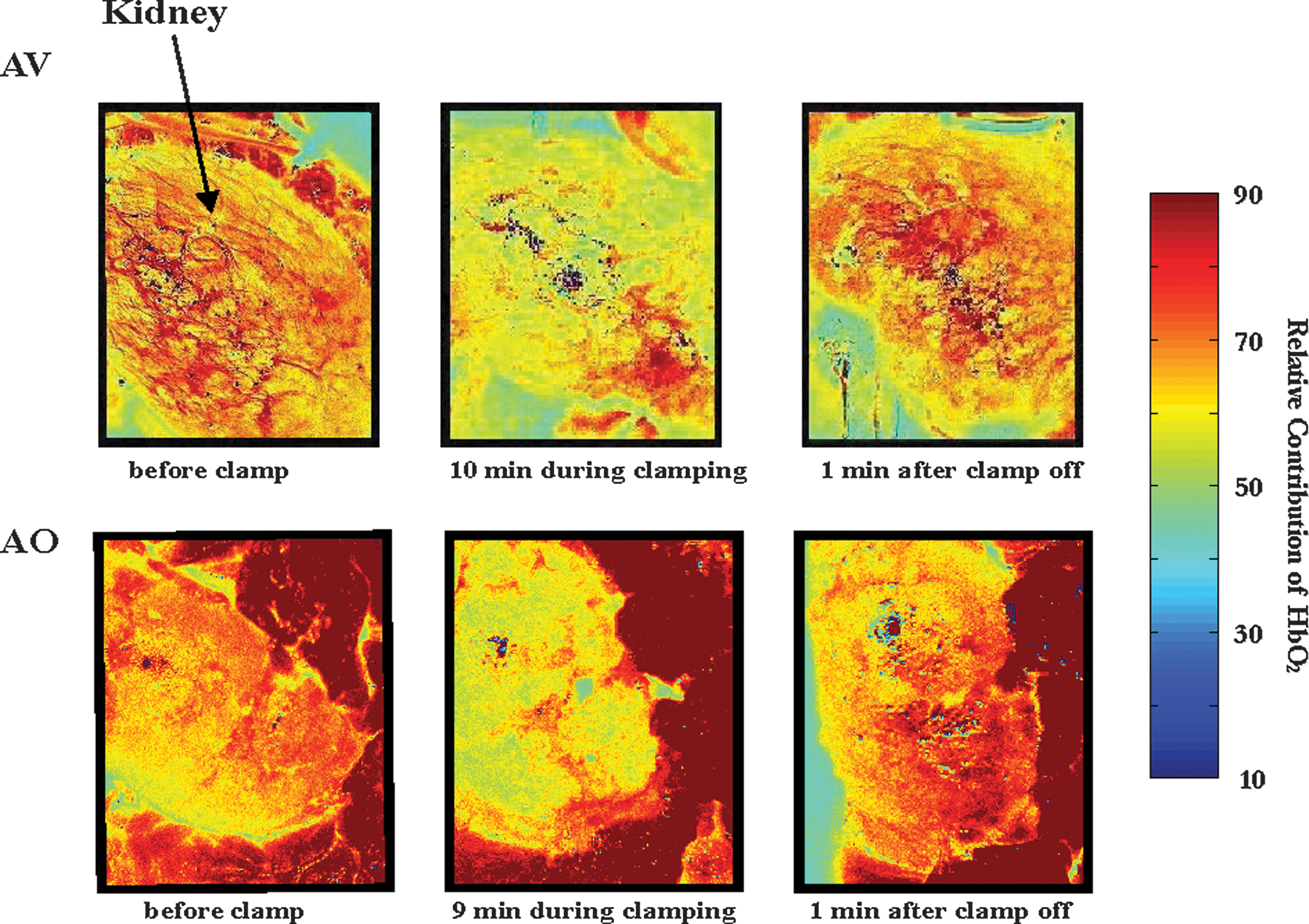
Renal oxygenation maps. AV=artery and vein; AO=artery-only.

Oxyhemoglobin (%HbO2) of renal cortex after hilar occlusion. AV=artery and vein; AO=artery-only.
During 0–5 minutes of occlusion.
During 5–10 minutes of occlusion.
During 45–50 minutes of occlusion.
Clinical and operative factors were evaluated for their ability to predict mean %HbO2 during vascular occlusion. Ischemia time, diabetes mellitus, and hypertension were not correlated with mean ischemic %HbO2 (t0–t52 min) (P=0.24, 0.84 and 0.39, respectively).
The ability of %HbO2 to predict postoperative renal function was also assessed. The correlation between mean ischemic %HbO2 (t0–t52 min) and eGFR at most recent follow-up (median 6.8 mos for AO and 2.7 mos for AV) was evaluated. In the AV group, but not the AO group, a lower %HbO2 was associated with a lower eGFR at the most recent follow-up (r=0.46, P=0.02). On multivariable analysis, mean ischemic %HbO2 in the AV group remained a significant predictor of postoperative eGFR, independent of ischemia time (odds ratio 2.31; 95% confidence interval 0.29–4.32; P=0.03). Because mean ischemia time was longer in the AO group, which could explain the lack of a correlation between %HbO2 and eGFR, a subset analysis was performed for patients with ischemia time <45 minutes (Table 3). There remained no difference in postoperative renal function between cohorts and still no correlation between mean ischemia %HbO2 and most recent GFR in the AO group. When considering all patients, there was no difference between AO and AV in postoperative eGFR, including eGFR at last follow-up and % decrease in eGFR (Table 4).
Last follow-up eGFR=eGFR of patient at last follow-up after discharge; change of eGFR=(last follow-up eGFR–preoperative eGFR)/preoperative eGFR.
AV=artery and vein; AO=artery-only; eGFR=estimated glomerular filtration rate; SD=standard deviation.
Last follow-up eGFR=eGFR of patient at last follow-up after discharge; change of eGFR=(last follow-up eGFR–preoperative eGFR)/preoperative eGFR.
AV=artery and vein; AO=artery-only; eGFR=estimated glomerular filtration rate; SD=standard deviation.
Discussion
The kidney is exquisitely sensitive to vascular occlusion during PN because metabolic activities in the normal state are predominantly aerobic. Tissue hypoxia contributes to the pathogenesis of acute kidney injury, 9 although there is no consensus regarding the safe threshold ischemia time for patients with two functional kidneys. Furthermore, studies have suggested that maintenance of retrograde venous perfusion (AO) may mitigate some of the ischemic injury. Animal studies have demonstrated that solitary kidneys subjected to AO clamping tolerated longer periods of ischemia under hypothermic conditions and demonstrated improved renal blood flow after occlusion during warm ischemia. 1,2
Work by Orvieto and colleagues 10 recently showed that renal function was better protected in animals undergoing AO compared with AV occlusion during open warm ischemia, but not in animals undergoing laparoscopic warm ischemia for 2 hours. A subsequent human study found AO was associated with renal function preservation when laparoscopic PN was performed within a mean 35 minutes of warm ischemia. 3
We hypothesize that assessing renal oxygenation intraoperatively during PN may enhance our understanding of the response of the individual renal unit to ischemia and the related impact on postoperative functional decline. In a preclinical study, Tracy and associates 4 showed that %HbO2 during ischemia was higher for animals subjected to AO occlusion, corroborating the findings of Orvieto and colleagues. 10 In the present study, we similarly evaluated renal oxygenation in humans undergoing open PN using DLP-HSI as described previously. 5
In this open PN study, the absolute and change in %HbO2 were similar for patients undergoing AO vs AV vascular occlusion, differing substantially from the animal study of Tracy and coworkers. 4 AO was not superior to AV based on eGFR measures, although any advantage of AO may have been mitigated by prolonged ischemia. Nevertheless, when patients with ischemia times >45 minutes were excluded, there was still no difference observed in postoperative eGFR. This result is consistent with our finding that %HbO2 did not differ significantly between the two cohorts.
It is not clear why AO vs AV make a difference in animals, but in humans, AO vs AV may not. Previous porcine studies have shown that AO results in lower eGFR decline than AV. 10 Human studies, however, are more conflicting. One retrospective study suggested a benefit of AO clamping, 3 while another recent prospective human study found AV clamping was associated with lower eGFR decline in the early postoperative period, although there was no difference in differential function of the operated kidney. 11
The utility of HSI as a clinical tool could be its ability to guide surgeon decision-making during PN. After 45 minutes of occlusion, a further drop in HbO2 saturation was observed for both AO and AV clamping. This time point could represent a critical human threshold in renal perfusion and subsequent renal injury. Indeed, others have found a high risk of renal insufficiency in solitary kidneys undergoing PN under cold ischemia in excess of 45 minutes, 12 We acknowledge that this finding alone has limited application because ischemia times >45 minutes are rare. We did observe, however, that mean ischemic %HbO2 was correlated with postoperative renal function. While this finding was only significant in the AV group, lack of statistical significance in the AO cohort may have been a result of inadequate sample size. If this correlation is supported in future studies, patients with lower intraoperative mean %HbO2 would alert the surgeon to the need to minimize ischemia time, perhaps through measures such as early unclamping.
The DLP-HSI tool has some limitations that are worth mentioning. It detects only Hgb saturation so it cannot be used as a measure of oxidative damage unless recalibrated to measure other molecules. While it only measures oxygenation of the renal surface, this should be reflective of the entire kidney during hilar clamping. Finally, measurements need ambient darkness despite lasting only a second to take the snapshot.
Limitations of this study include the small sample size and nonrandomized study design. The small number of AO patients, in particular, may have impaired detection of %HbO2 differences from AV. Along with the longer AO ischemia time, the small AO cohort number may also explain why, unlike AV, postoperative GFR was not correlated with %HbO2. The longer ischemic times in the AO cohort, a limitation of the nonrandomized study design, suggest the tumors were more technically challenging, and indeed they were larger, although R.E.N.A.L. nephrometry was similar to the AV cohort. The slightly longer ischemia times (mean 6 min) could have had an overall detrimental affect on postoperative renal function and may have mitigated any measurable advantage of artery only occlusion. Although this was partially adjusted for with a subset analysis excluding patients with more than 45 minutes of ischemia time, the resulting small patient numbers limit interpretation.
Finally, the difference in median GFR follow-up between AV and AO cohorts (2.7 vs 6.8 mos) may have allowed more time for GFR recovery in the AO cohort. This difference, however, was not statistically significant (P=0.68), and some studies have shown no improvement in GFR 3 months after PN. 13,14 In addition, when a subset analysis was performed for those who were followed beyond 6 months, the change of eGFR was still similar between two groups (AO vs AV: 16.44% vs 14.01%, P=0.78).
Conclusion
Hyperspectral imaging is a noninvasive method of measuring real-time, renal-specific oxygenation during PN. Renal oxygenation as assessed by DLP-HSI was similar for AO vs AV occlusion. Significant retrograde venous oxygen delivery using an AO occlusion technique could not be demonstrated in this population of difficult PN where prolonged ischemia times may have mitigated any advantage. Further study is necessary, however, because %HbO2 during ischemia may be prognostic of postoperative renal function.
Footnotes
Disclosure Statement
Dr. Zuzak works for Digital Light Innovations. Dr. Cadeddu has been a member of an Ethicon advisory committee. For the remaining authors, no competing financial interests exist.