
Abstract
Purpose:
Fluoroscopy usage during endoscopic procedures exposes the patient and operating room staff to ionizing radiation. Pooled mean fluoroscopy usage time during ureteroscopy reported from recent literature is 144 seconds per case. The purpose of this study was to evaluate radiation exposure using a minimal-use fluoroscopy protocol during ureteroscopic treatment of urinary-tract calculi and determine patient and perioperative factors associated with increased fluoroscopy time.
Materials and Methods:
A protocol was developed to access the ureter with the ureteroscope without fluoroscopy usage, and minimize radiation utilization during each portion of the case. Over a 16-month period, fluoroscopy usage and radiation dose for all cases involving retrograde ureteroscopy for a single surgeon were prospectively recorded. A chart review was performed on patient factors and intraoperative events.
Results:
In 162 consecutive ureteroscopic procedures for nephrolithiasis, there were 156 renal units with fluoroscopic usage data, of which total mean and median fluoroscopy time, including stent placement, was 3.3 and 2.0 seconds (0–35 seconds), respectively. Excluding fluoroscopy usage to confirm ureteral stent placement, 75% of all cases did not require any fluoroscopy time (fluoroless), and 85% required 2 seconds or less. Of the 98 renal units with radiation dosage data, the total mean and median radiation dose measured as air kerma was estimated at 1.1 and 0.6 mGy (0.0–17.5 mGy), respectively. Reasons for utilization of total fluoroscopy time more than 5 seconds included stone impaction, ureteral tortuosity or narrowing, collecting system aberrant anatomy, and difficult ureteral stent placement.
Conclusions:
The reduced fluoroscopy protocol resulted in minimal fluoroscopy time and radiation exposure, significantly lower than reported in the literature. Fluoroless ureteroscopy is safe and feasible in the majority of ureteroscopic cases and lessens exposure to patients and staff.
Introduction
While radiation exposure from fluoroscopy is determined by machine settings, machine positioning, and patient factors, the most important determinant is fluoroscopy time. 3 It has been reported that the range of average fluoroscopy times during ureteroscopy is between 44 and 314 seconds, and reduced to 16 seconds in one series of select patients. 3 –10
To further reduce radiation exposure with fluoroscopy during ureteroscopy, a protocol was developed and implemented with the as-low-as-reasonably achievable (ALARA) principle in mind. The purpose of this study was to measure fluoroscopy time and radiation exposure during consecutive ureteroscopic surgery with this protocol, and to determine factors associated with increased exposure.
Patients and Methods
Between December 2010 and April 2012, consecutive patients undergoing flexible (7.5F Storz Flex-X2 ureteroscope, Germany) and/or semirigid ureteroscopy by a single surgeon for stone disease were entered into an institutional database prospectively. Cases performed to evaluate for malignancy- or nonstone-related indications were excluded. Demographic and perioperative information recorded included age at surgery, gender, body–mass index (BMI), laterality, presence of a preoperative ureteral stent, associated hydronephrosis, presence of stone impaction, stone location, use of ureteral access sheath, and operative time.
Radiation exposure for each case was recorded on a digital portableGE OEC 9900 Elite (GE Healthcare) C-arm with a 12-inch collimator, which provided total fluoroscopy time and air kerma measurements reported in milligray (mGy). Fluoroscopy times during ureteroscopy and during ureteral stent placement were recorded separately. Fluoroless ureteroscopy was defined as no fluoroscopy utilized during the entire ureteroscopic portion of the procedure. The effective dose measured in millisieverts (mSv) was estimated by multiplying fluoroscopy time by the effective dose rate of 0.024 mSv/sec, which has been previously calculated in a validated phantom model. 9 We have calculated a similar effective dose rate for our specific setup. To minimize radiation exposure, the fluoroscopic C-arm was most frequently set in the low dose and pulsed settings with last image save. The device was set to automatically adjust for voltage and tube current settings within the low-dose parameters. The X-ray emitter was placed below the operating room table with the image collimated to limit exposure to surrounding organs.
To minimize radiation exposure, a step-wise approach during ureteroscopy was created to reduce reliance on fluoroscopy (Fig. 1). First, a thorough patient assessment was performed to determine anticipated challenges during the case, such as stone impaction, a tortuous ureter, anatomic anomalies, stone burden, and locations. This information is obtained from the patient history, physical, and available imaging.
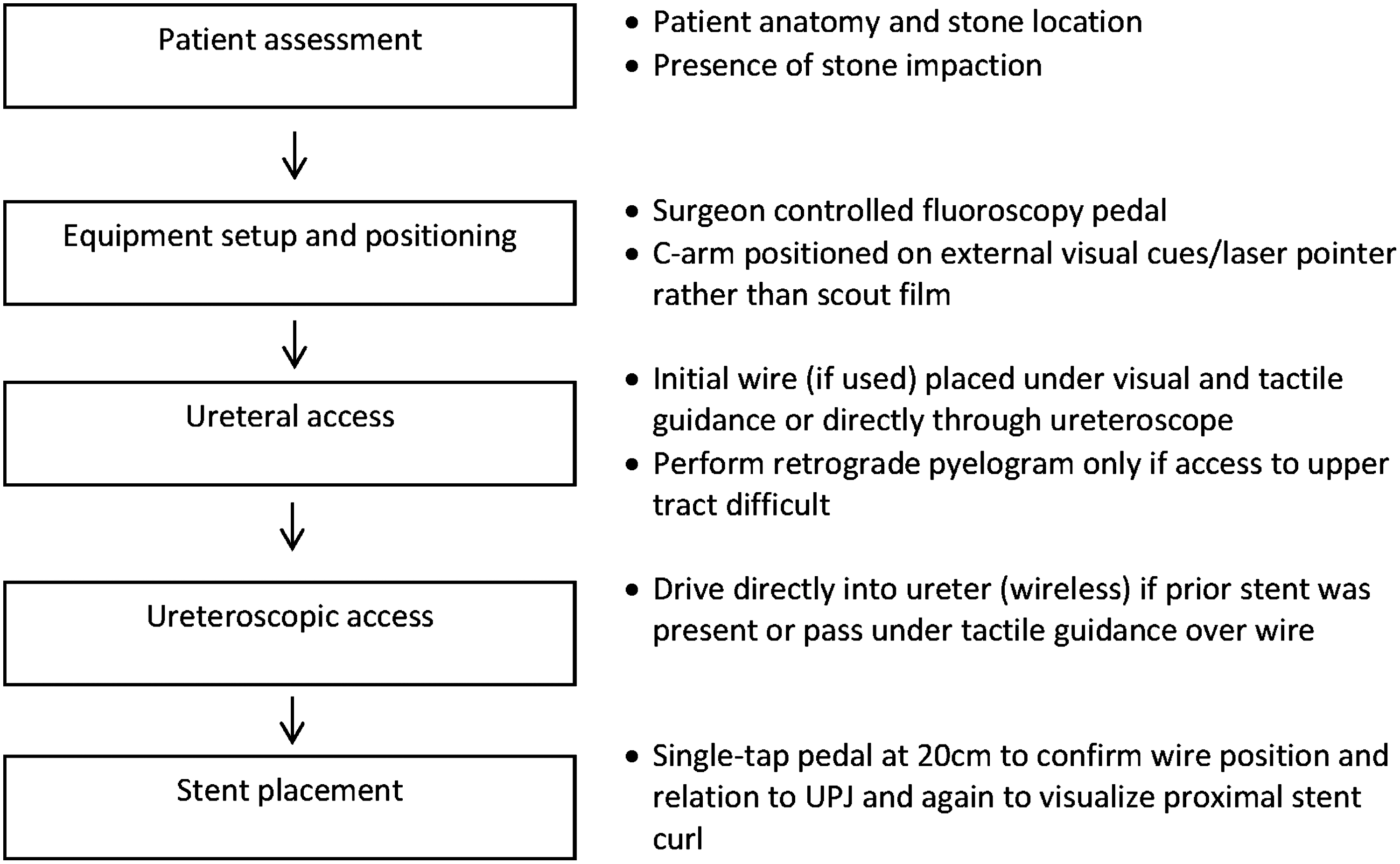
Flow diagram for fluoroless ureteroscopy protocol.
Next is the fluoroscopic C-arm setup, which includes a surgeon-controlled fluoroscopy pedal and use of external cues to position the image intensifier over the patient. The C-arm also has a laser guidance device that emits an aiming beam. Pulsed and low-dose settings are utilized to start each case.
Third, ureteral access may be achieved in several ways without use of fluoroscopy, utilizing tactile guidance and visual cues. If a prior ureteral stent is in place, most commonly the stent is removed, and we then directly drive the ureteroscope (semirigid or flexible) through the urethra and into the ureter under visual guidance only to gain access, as described previously. 11 Alternatively, the stent is partially externalized, and a wire is placed through the stent or directly into the ureter under cystoscopic guidance. The stent is then removed, and the ureteroscope is passed over the wire into the ureter estimated by the length of ureteroscope outside the body. No fluoroscopy is used to confirm wire placement if the wire passes without resistance. A visual cue that suggests adequate wire insertion is to compare the length of the external portion of the wire to the contralateral leg in the lithotomy position. If the tip of the wire is beyond the foot, then the internal portion of the wire is likely distal to the proximal ureter and may come out during scope insertion. If there is no prior stent and the ureteral orifice does not appear to be able to accommodate the ureteroscope using the above methods, a wire is passed through the cystoscope and advanced gently while visualizing the wire passing through the ureteral orifice until resistance is met. Again, no fluoroscopy is used to confirm wire placement if the wire passes without resistance to what is estimated to be at least the mid-ureter. A dual-lumen catheter or 8–10F coaxial dilation set (Cook Medical, Spencer, IN) is passed over the wire to dilate the ureteral orifice and intramural ureter only. The ureteroscope is then passed over the wire into the ureter, and the wire is removed. At this point, in most cases, there is no wire left within the ureter, which we find to allow easier navigation throughout the ureter. In cases where a ureteral access sheath is planned, it is only passed after ureteroscopy has been performed, and a wire has been left directly within the kidney. Typically, a small-diameter (9.5F) sheath is used and passed using tactile feedback unless resistance is encountered, at which time fluoroscopy is used. A safety wire is left outside the access sheath.
Once ureteral access is achieved, the ureteroscope can be driven to the renal pelvis under visual guidance. After stone treatment is complete, a wire is passed back through the ureteroscope and left directly at the level of the kidney. Pullback ureteroscopy is performed, leaving the wire in place with visualization of the entire ureter for residual fragments. At this point, no fluoroscopy has been used in the majority of cases. If there is difficult access, fluoroscopy may be used during wire or scope insertion, retrograde pyelogram, balloon dilation, or placement of ureteral access sheath.
Finally, stent placement is performed over the wire under cystoscopic guidance rather than fluoroscopic guidance. When the stent is passed to the ureteral orifice at the 20-cm mark, a single tap of the pedal confirms wire placement and shows the relation of the proximal stent to the UPJ. After the stent is deployed, the proximal stent curl is confirmed with a single tap of the pedal, whereas the distal curl is observed directly through the cystoscope.
Results
Over the 16-month study period, 162 renal units in 105 patients were treated for stone disease with ureteroscopy. Patient characteristics are listed in Table 1. Renal units treated were predominately from male patients (59%) and on the left unit (61%). The median BMI was 28.6±8.9 kg/m2; 43% of renal units had an indwelling ureteral stent at the time of ureteroscopy, which we presume that were all placed under fluoroscopic guidance. Stone impaction and associated hydronephrosis were observed in 28% and 50% of renal units, respectively. No intraoperative complications, including ureteral perforations, were observed. There were no cases of silent hydronephrosis or stricture found on renal ultrasound 6 weeks postoperatively. One patient underwent an unplanned procedure for a residual ureteral stone fragment, followed by an uneventful recovery.
BMI=body–mass index.
Fluoroscopy time data were available for 156 renal units, whereas radiation dosage data were available for 98 renal units (Table 2). Median fluoroscopy time and air kerma were 2.0±4.8 seconds and 0.6±2.1 mGy, respectively. The median effective dose was estimated at 0.05±0.05 mSv. Fluoroless ureteroscopy was performed in 117 cases (75%). The ureteroscopy and stent placement times using fluoroscopy were recorded separately in 135 cases. Of these cases, the mean and median times for the ureteroscopic portion were 0.45 and 0 seconds, respectively, and for confirmation of stent placement were 1.8 and 1.8 seconds, respectively.
Radiation dosage data available for 98 renal units. Fluoroscopy time available for 156 renal units.
Conversion based on effective dose of 0.024 mSv/sec from Lipkin et al. (see discussion).
Excluding fluoroscopy time used to confirm stent placement, ≤2 seconds and ≤5 seconds of fluoroscopy time were utilized in 85% and 90% of cases, respectively. Including fluoroscopy time used for stent placement, ≤2 seconds and ≤5 seconds of fluoroscopy time were utilized in 57% and 88% of cases, respectively. In 10 cases (6%), fluoroless ureteroscopy was performed without ureteral stent placement. When a ureteral access sheath was used (14%), the mean and median total fluoroscopy time was 2.2 and 2.0 seconds, respectively; 17 cases (11%) utilized more than 5 seconds of total fluoroscopy, including stent placement. Increased utilization of fluoroscopy was attributed to stone impaction (71%), ureteral tortuosity or narrowing (29%), collecting system aberrant anatomy (12%), and difficult ureteral stent placement (12%).
Discussion
The cumulative risk of cancer attributable to radiation exposure from diagnostic X-rays is estimated at 0.4%–0.9% in the United States. 1,12 Radiation-induced malignancy is a stochastic effect, because any amount of radiation could theoretically injure DNA. In contrast, deterministic effects such as cataracts, erythema, and skin burns require a threshold dose before the effects appear, with increased severity as dosage rises. While fluoroscopy is a significant source of radiation, the radiation exposure during ureteroscopy is far below the threshold for deterministic effects. Based on a cadaver study measuring tissue-specific dosing, it is estimated that one in 1000 patients would develop a malignancy at the posterior skin after a single ureteroscopy based on a linear nonthreshold model. 13 To minimize the stochastic effects of fluoroscopy, the principle of using ALARA should be applied to ureteroscopic procedures.
The total fluoroscopy time has been reported to be the major determinant of radiation dose, followed by dose rate setting, anterior-posterior diameter, and the source to skin distance. 3 In our consecutive series of patients undergoing ureteroscopy for stone disease, fluoroless ureteroscopy was able to be performed in 75% of cases. Including fluoroscopy time used for ureteral stent placement, median fluoroscopy time and air kerma were 2.0±4.8 seconds and 0.6±2.1 mGy, respectively. The median effective dose was estimated at 0.05±0.05 mSv, equivalent to ∼2 posteroanterior chest X-rays (0.02 mSv each), and 10× less than one kidney ureter bladder (0.7 mSv). 14 Our median fluoroscopy time and radiation dosage compare favorably to other series in the literature (Table 3). The pooled mean fluoroscopy time reported in the literature is 144 seconds, while in our series, the mean fluoroscopy time was 3 seconds.
ESD=entrance skin dose measured from fluoroscopy unit dosimeter as air kerma 70 cm from radiation source.
MLD=midline absorbed dose calculated from ESD at midpoint of umbilical anterior-posterior diameter.
Other groups have also reported significantly less fluoroscopy utilization after implementing reduced fluoroscopy protocols. Greene and colleagues reported reduction in mean fluoroscopy exposure from 86.1 to 15.5 seconds after instituting a protocol that included increased reliance to visual and tactile cues, pulsed fluoroscopy, and avoidance of the scout film and retrograde pyelogram. 5 A limitation of this series is that the reduced-fluoroscopy protocol patients were selected, thinner, and nonobese. In contrast to their technique, we utilize a surgeon-controlled fluoroscopy pedal while the technician is present to assist with C-arm setup and positioning. We do not time the C-arm activation to respiration and do not instill contrast to map the collecting system if all calyces were felt to be fully inspected. Ngo and colleagues reported a 24% decrease in mean fluoroscopy time to 128 seconds after providing surgeons with periodic reports of fluoroscopy times compared to their peers. 6 Reduction of fluoroscopy utilization in these studies may be attributable to the Hawthorne effect, where subjects modify their behavior in response to knowing that they are being studied. A general awareness of minimizing fluoroscopy use to reduce its stochastic effects during ureteroscopy may be a first step to decrease overall radiation exposure.
The underlying approach of our protocol assumes that the use of fluoroscopy is a last resort. It may be assumed that fluoroscopy is classically used during all aspects of ureteroscopy, including C-arm setup and scout film, initial wire placement, and placement of a second wire, retrograde pyelogram, balloon dilation, passage of ureteroscope, and access sheath, to help access and confirm location within the kidney, and stent placement. Live and continuous fluoroscopy may be performed during many of these steps as well. A strength of our protocol is that it utilizes techniques and equipment already present in the surgeon's toolkit. It relies on visual and tactile cues to access the ureter. If needed, fluoroscopy is used with a spot technique by the surgeon-controlled foot pedal and positioned using a laser-guided C-arm. The initial steps are aimed toward obtaining ureteroscopic access into the ureter, after which access to the proximal ureter and renal pelvis can be readily obtained under visual guidance. Wireless ureteroscopic access is frequently performed, or the scope is inserted over a wire that has been passed through the ureteral orifice and advanced with visual and tactile guidance only. Good endoscopic principles are necessary such as maintaining awareness of wire position when used to pass the ureteroscope or access sheath, disassembling the scope without dislodging the wire, and backing out the ureteroscope while leaving the wire at the level of the kidney. A limitation of the approach is the generalizability of some of the techniques, including driving directly into the distal ureter without a wire in place. The maneuverability of the ureteroscope in the bladder can be challenging. However, the ureteroscope can always be passed over a wire into the ureter. Finally, it is also important to involve the radiation technologists, surgical assistants, and trainees to adopt a minimal-use mentality toward fluoroscopy use.
While time is a major determinant of radiation exposure, few studies have reported an effective dose of radiation, which assumes a nonuniform absorption of radiation in different organs. The effective dose is a derived value from radiosensitive tissues and organs that indicate the relative risk of malignancy. 15 Rebuck and colleagues reported data on 103 patients undergoing ureteroscopy with mean fluoroscopy time of 314 seconds. The mean effective dose of 6.0 mSv was calculated using a dose–area product (rad×cm2) obtained from the C-arm and converted using accepted conversion tables. 8 Lipkin and colleagues used a validated phantom model to calculate effective dose rates and compare them to 30 nonobese men performed using the same machine and settings. 9 The mean ureteroscopy effective dose rate was 0.024±0.0019 mSv per second in their model. In our study, we calculated our median effective dose at 0.05±0.05 mSv per procedure based on this conversion. A limitation of this conversion is that our patients were more overweight with a median BMI of 28.6 kg/m2 compared to their nonobese cohort. The conversion may also actually overestimate the actual effective dose in our series, since our portable C-arm unit was placed below the operating room table, which may cause radiation scatter and reduce the radiation absorbed by the patient. However, when table attenuation was measured using our setup, we found that the air kerma representing the absorbed dose closely approximated the entrance skin dose, measured in mGy. The calculated entrance skin dose was used to estimate a mean fluoroscopy effective dose rate of 0.021±0.009 mSv, using simulation software and a model based on an equivalent radiographic projection. This compares similarly to the mean fluoroscopy effective dose rate from Lipkin and colleagues. 9
Adjustments in C-arm machine settings can reduce radiation exposure. Dose reduction techniques include pulsed fluoroscopy, last image hold, narrow collimation, removal of grid, low-dose settings, and maximizing source-to-patient distance. 16 Elkoushy and colleagues changed the fluoroscopy rate from 30 to 4 frames per second and observed a decreased mean fluoroscopy time from 109.1 to 44.1 seconds. The authors reported that the pulsed low-frame fluoroscopy did not have any significant impact on image quality or stone-free rates. 10 In contrast to their technique, we do not place a second wire for proximal ureteral and renal stones unless a ureteral access sheath is used and/or difficult anatomy is anticipated. In our experience with the low-dose setting on our portable fluoroscopic units, the image quality with obese patients is almost always sufficient for determination of wire or stent position without the need for the standard higher dose setting.
Our findings must be interpreted within the context of limitations of our study design. This is a series from a fellowship-trained single surgeon in endourology, and generalizability of all of the techniques may be limited. Despite these limitations, the strengths of this article include the consecutive nature and the patients treated at a referral center with complex anatomy and stone burden. One's training, experience, and comfort level affect the reproducibility of fluoroless ureteroscopy. Fluoroless ureteroscopy is feasible in many cases; however, we have fluoroscopy available and the C-arm positioned in every ureteroscopic procedure. Importantly, the findings of this study do not support the notion that fluoroscopy is unnecessary for ureteroscopy. The goal of this study was to report our technique and educate providers as a whole. The radiation exposure to the surgeon and staff is not insignificant. 4 With some modification of technique, reducing seconds of radiation exposure at each step makes a difference, especially for the recurrent stone former and the surgeon/staff involved in a high volume of these cases.
Conclusions
Fluoroless ureteroscopy can be performed in the majority of cases for stone disease. The protocol relies on tactile and visual feedback and frequent use of wireless ureteroscopic access with avoidance of scout film and retrograde pyelogram. There is no safe threshold below which the stochastic effects of radiation cannot occur. Using an ALARA approach, all techniques to reduce the amount of radiation exposure, however, incremental, should be practiced.
Footnotes
Acknowledgments
The authors would like to acknowledge David Zamora and Kalpana Kanal for their assistance.
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.