
Abstract
Objectives:
To evaluate the efficacy and safety of holmium laser enucleation of the prostate (HoLEP) versus transurethral resection of the prostate (TURP) for relief of bladder outlet obstruction (BOO) on benign prostatic hyperplasia (BPH).
Methods:
A systematic literature search for randomized controlled trials (RCTs) comparing HoLEP and TURP in several databases from 1996 to 2011 were performed. Meta-analysis was conducted with the Review Manager Software.
Results:
Of 248 potential citations, 6 RCTs were included into our meta-analysis. There was no significant difference between the two groups in the maximum urinary flow rate (Qmax) and international prostate symptom score (IPSS) at 1 month (p=0.41 and p=0.87) or 6 months (p=0.07 and p=0.37) after treatment. However, at 12 months postoperatively, the Qmax and IPSS in the HoLEP group were significantly better than those in the TURP group (p<0.0001 and p=0.01). The results also suggested a benefit of HoLEP over TURP in blood loss (p=0.001), catheterization time (p<0.0001), hospital stay (p=0.001), and blood transfusion rate (p=0.04), while the results favored TURP over HoLEP for operative time (p=0.001) and the incidence of postoperative dysuria (p=0.003).
Conclusions:
Comparing with TURP, HoLEP showed slightly better postoperative results in Qmax and IPSS during 12-month follow-up, as well as significantly better perioperative results and similarly low complication rates. However, the operative time and the incidence of postoperative dysuria favor TURP. Generally, HoLEP is a promising minimal invasive alternative to TURP for treatment of BPH.
Introduction
Holmium laser techniques have been introduced for the surgical treatment of BPH more than 15 years. Holmium laser resection of the prostate (HoLRP) was first described by Gilling et al 4 in 1995, and then combined with transurethral tissue morcellation, evolved into holmium laser enucleation of the prostate (HoLEP). 5 Since then, Holmium laser has shown therapeutic potential advantages in BPH, especially in the treatment of large prostate gland. Refinement of the holmium laser technique and development of an efficient tissue morcellator has led to the true anatomic enucleation of prostatic adenomas of any size. 6 According to the results of clinical trials comparing HoLEP and TURP, improvements in symptom scores, quality of life (QoL) indices, and flow rate after the HoLEP procedure approach those obtained after TURP in the short-term postoperative period. 7 –9 Many authors argued that HoLEP is a promising procedure to replace TURP. 6 –9 Nevertheless, the lack of long-term results of randomized studies and the long learning curve restricted more widespread adoption of this procedure. 10 –12 The question still remains, however, what the potential benefits HoLEP can offer to BPH patients over traditional TURP? Whether this new procedure worth the investment in a 100-watt Holmium equipment of the hospital and the extra training that physicians will need?
Our aim was to investigate the impacts of HOLEP versus TURP on BPH in patients with symptomatic prostatic obstruction, and to quantify the efficacy and safety by a systematic review and meta-analysis of randomized controlled trials (RCTs).
Methods
Literature search
A systematic review of the literature was performed to identify articles published between 1996 and 2011 on the management of symptomatic prostatic obstruction. We conducted a systematic search of MEDLINE, EMBASE, Cochrane Library and Web of Science using the search terms of “holmium laser enucleation (or HoLEP),” “transurethral resection the prostate (or TURP)”and “prostate.” No temporal, regional, publication status, or language restrictions were set. Additionally, a manual search of references from identified clinical trials and review articles were performed.
Study selection
Inclusion and exclusion criteria were defined pre literature search. Studies were included if met the following criteria: (1) RCTs comparing the efficacy and safety of HoLEP with TURP; (2) patients with lower urinary tract symptoms caused by BPH; (3) patients with maximum flow rate (Qmax) ≤15 mL/s and an international prostate symptom score (IPSS)≥8. Exclusion criteria included: neurogenic bladder; previous urethral, prostate, and bladder surgeries; suspected prostate cancer.
Validity assessment
The reference lists of all traced articles and general reviews of this topic were examined manually by two reviewers (L.Y. and J.F.T.), and all disagreements were resolved by consensus. The methodological quality of included studies in the meta-analysis was scored by using the Jadad composite scale. 13,14 This is a 5-point scale, a score of 2 or less indicates low quality of the study and a score of at least 3 indicates high quality. 15,16
Data extraction
The following variables were recorded: authors, journal and year of publication, number of patients, age, IPSS, QoL, postvoid residual volume (PVR), detrusor pressure at maximum urinary flow rate (PdetQmax), Qmax, operative time, blood loss, catheterization time, hospital stay, urethral stricture, stress incontinence, blood transfusion, and reintervention.
Statistical analysis
The risk ratio was used for binary outcomes, and mean difference or standardized mean difference was used for continuous variables. Pooled estimates were calculated using the fixed-effects model (Mantel-Haenszel method) 16 if no heterogeneity was presented, otherwise, the random-effects model (DerSimonian-Laird method) 17 was used. The overall effects were determined by the Z-test and p<0.05 was considered as statistically significant. The Cochrane χ2-test and Inconsistency (I 2) were used to assess the heterogeneity among studies. p<0.10 indicated the present of heterogeneity, I 2<50% indicated that the heterogeneity was acceptable. All tests were performed using the Review Manager Software (RevMan 5.1, Cochrane Collaboration, Oxford, England).
Results
Study characteristics
Our initial search yielded 248 potential citations, of which 242 were excluded for reasons presented in Figure 1. The literature search and study selection process therefore identified 6 RCTs that examined a total of 541 patients who were treated using either HoLEP (n=271) or TURP (n=270). 18 –23 The Jadad scores of the studies included are shown in Table 1. Of the 6 RCTs, 4 studies reported follow-up data collected at 1, 3, 6, and 12 months after treatment 18,20 –22 and 2 presented 3- 19 and 7-year 23 long-term follow-up results, respectively. It was decided to use the data obtained within the 12 months after operation for the meta-analysis. Table 2 provides an overview of the composite baseline characteristics of all trials included in the meta-analyses.

Flow chart for study selection. HoLEP=holmium laser enucleation prostatectomy; TURP=transurethral resection of the prostate.
Unit: mL.
nr=not reported; Qmax=maximum urinary flow rate; PVR=postvoid residual volume; PdetQmax=detrusor pressure at maximum urinary flow rate; IPSS=international prostate symptom score.
Quantitative data synthesis
Micturition parameters
At baseline, the Qmax of patients randomized to HoLEP or TURP appeared similar (Table 2). There was no statistically significant difference between the two groups in Qmax and IPSS at either 1 month (1.45 [−2.01, 4.92], p=0.41 and 0.21 [−2.18, 2.59], p=0.87) (Fig. 2) or 6 months (1.26 [−1.02, 2.63], p=0.07 and −0.57 [−1.80, 0.67], p=0.37) (Fig. 3) after treatment. However, at 12 months postoperatively, the Qmax in the HoLEP group were significantly greater than that in the TURP group (1.46 [0.98, 1.93], p<0.0001) and the IPSS in the HoLEP group were significantly better than that in the TURP group (−0.78 [−1.39, −0.17], p=0.01) (Fig. 4).

HoLEP versus TURP at 1-month follow-up assessment. Qmax=maximum urinary flow rate; IPSS=international prostate symptom score; SD=standard difference; CI=confidential interval.
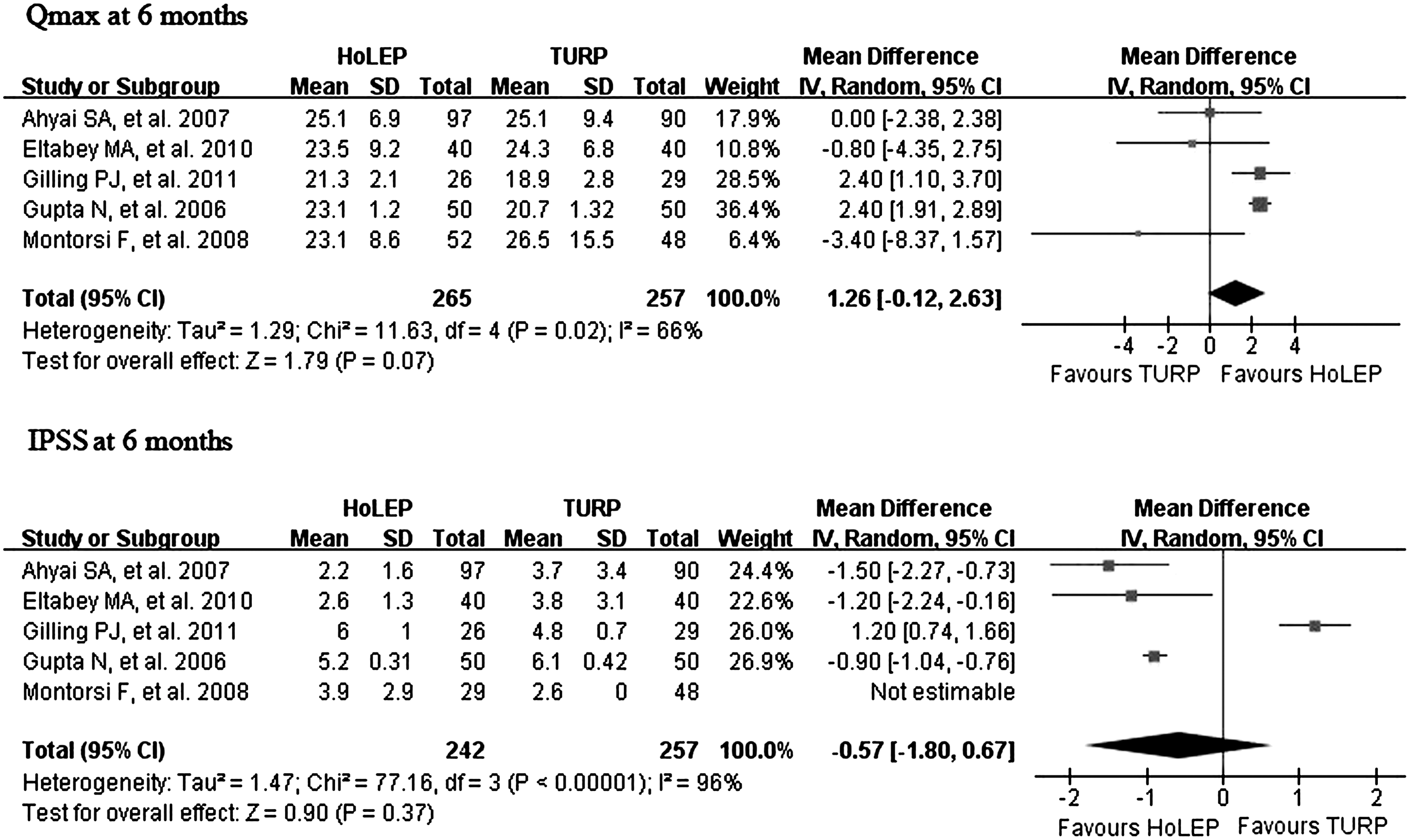
HoLEP versus TURP at 6-month follow-up assessment.
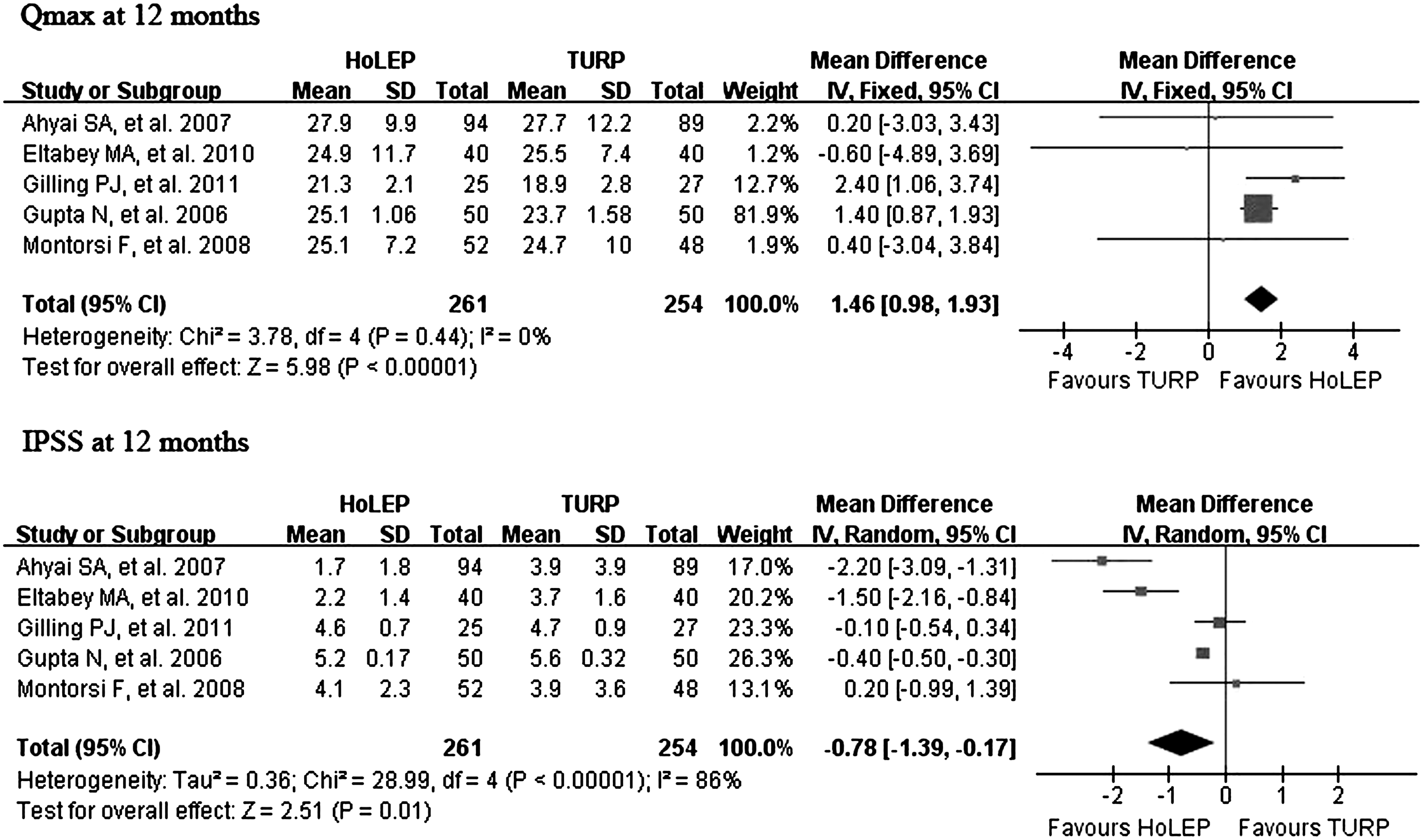
HoLEP versus TURP at 12-month follow-up assessment.
Perioperative results
The statistically significant differences in pooled estimates suggested a benefit of HoLEP over TURP in catheterization time (−1.50 [−2.22, −0.79], p<0.0001), blood loss (−0.46 [−0.81, −0.11], p=0.001), and hospital stay (−1.92 [−2.91, 0.93], p=0.001). In contrast, the pooled estimates favored TURP over HoLEP in the operative time (15.91 [5.45, 26.36], p=0.001). There were no significant differences between the two groups in the weight of resected tissue (4.12, [−7.26, 15.51], p=0.48) (Table 3).
Mean difference [95% Confidence interval].
Standard mean difference [95% Confidence interval].
Risk Ratio [95% Confidence interval].
HoLEP=holmium laser enucleation prostatectomy; TURP=transurethral resection of the prostate.
Adverse events
Table 3 shows the adverse events after surgery. It suggests that dysuria was more frequent in the HoLEP group than that in TURP group (1.87 [1.25, 2.80], p=0.003), while the blood transfusion rate in the HoLEP group was significantly lower than in the TURP group (0.23 [0.06, 0.92], p=0.04). No statistically significant difference was noted between the HoLEP and TURP groups in urethral stricture (0.86 [0.38, 1.97], p=0.73), stress incontinence (1.11 [0.40, 3.12], p=0.84), and recatherization (0.63 [0.28, 1.43], p=0.38).
Discussion
Laser treatments for BPH can offer a number of benefits over the alternative approaches, including decreased morbidity and shortened hospital stay. There are several techniques for laser prostatectomy that continue to evolve, among which HoLEP is a main competing technique currently. The HoLEP, using the Holmium: YAG laser (Ho:YAG), has been shown to be as effective as open surgery in generating cavity, since the tip of the fiber mimics that of the surgeon's index finger during open prostatectomy. 24 Besides, HoLEP is suitable for patients on anticoagulation as well as those with large prostates. 25,26,27 Some studies suggested that HoLEP versus TURP results in less blood loss, lower transfusion rates, and a shorter hospital stay. 18,28 However, the advances of HoLEP over TURP still need to be confirmed by high-quality prospective RCTs.
The present meta-analysis compared the efficacy and safety profile of HoLEP and TURP for BPH. There was no statistically significant difference between the two groups in Qmax and IPSS at 1- and 6-month follow-up postoperatively, while the higher Qmax values and the lower IPSS were noticed in the HoLEP group at 12-month postoperative follow-up, although it is not necessarily clinically significant. However, it showed that HoLEP is at least equivalent to TURP in the early postoperative period. 28,29 The question is whether the patients who were improved from baseline to early follow-up would sustain these improvements at later follow-up. Unfortunately, we fail to assess the long-term efficacy of HoLEP due to the lack of data. In fact, most of the minimally invasive treatments, which are proposed as an alternative to TURP, lack the long-term follow-up data comparing with TURP.
Among the 6 trials included in the present meta-analysis, Ahyai et al 19 presented a 3-year follow-up comparing the outcome of HoLEP and standard TURP. AUA-SS were significantly better 2 years postoperatively in the HoLEP group (1.7 vs. 3.9, p<0.0001) and similar at 3 years (2.7 vs. 3.3, p=0.17). PVR volume was significantly better 2 years (5.6 vs. 19.9 mL, p<0.001) and 3 years (8.4 vs. 20.2 mL, p=0.012) postoperatively in HoLEP patients. Qmax was similar in the HoLEP and TURP groups at 2 years (28.0 vs. 29.1 mL/s, p=0.83) and at 3 years (29.0 vs. 27.5 mL/s, p=0.41) postoperatively. Gilling et al 23 reported the results of a randomized trial comparing HoLEP and TURP at 7 years postoperatively. The mean (±SD) values (HoLEP vs. TURP) were as follows: Qmax, 22.09±15.47 vs. 17.83±8.61 mL/s; AUA-SS, 8.0±5.2 vs 10.3±7.42; QoL score, 1.47±1.31 vs 1.31±0.85. Other authors also reported that HoLEP has expected durable effects. Elzayat and Elhilali 10 reported that, for patients who underwent HoLEP (n=26), six-year postoperative mean Qmax increased from 6.3 to 16.2 mL/s, while PVR decreased from 232 to 41.2 mL (p<0.0001). Mean IPSS improved from 17.3 to 5.6 (p<0.0001). Elmansy et al 30 reported the long-term durability of clinical outcomes of HoLEP during the 10-year follow-up in 949 patients. Postoperatively, all variables showed significant improvement starting at month 1 of follow-up and remained improved for the entire follow-up period. Postoperative mean PVR was 45, 25.7, and 52 mL, mean Qmax was 21.5, 24.3, and 23.4 mL per second, mean IPSS was 7.3, 4.4, and 3.8, and mean QoL was 1.7, 1, and 0.7 at 1 month, 1 year, and 10 years, respectively. Only one study 23 addressed the reoperation rate due to recurrence, three patients in the TURP group, while none in the HoLEP group. These data suggested that HoLRP was indeed a promising technique for treating BPH.
The operative time of HoLEP was consistently longer compared with TURP, while HoLEP offered the advantages over TURP in terms of blood loss, catheterization time, and hospital stay during the perioperative period. The fact that HoLEP needs a longer operative time than TURP had been reported by previous studies. In our study, the prostate size between groups is similar; thus, the extra time needed for morcellation of the enucleated tissues, difficulties in the operation, and an unskilled surgeon might contribute to this. Besides, some authors believed that HoLEP removes much more prostatic tissues than TURP, 29 which is supported by its greater drop in postoperative serum PSA levels, 11 and when operative time was adjusted for tissue retrieved, HoLEP was equally efficient. 23 However, in our meta-analysis, the resected weight was similar between groups. This might be explained by the fact that about 10% of the retrieved tissues by HoLEP were vaporized during the enucleation procedure. 31
Several articles had reported the rare need of blood transfusion for the HoLEP procedure. 32 In fact, among the studies included in the current meta-analysis, no patients in the HoLEP group required blood transfusions. This can be explained by the nature of Ho:YAG laser. The penetration depth in prostatic tissue is 0.4 mm and dissipating heat causes simultaneous coagulation of small- and medium-sized vessels to a depth of 2–3 mm, resulting in excellent hemostasis. 33 The hemostatic benefit of HoLEP leads to subsequent omitted or shorter postoperative irrigation time and quick discharges. 18 The less happened hyponatremia due to irrigation by saline also contribute to a shorter hospital stay. 34
It had been reported that the Holmium laser has minimal association with many side effects, such as irritative voiding symptoms or immediate postoperative dysuria, which are associated with other laser treatments. 35 However, our study showed the incidence of irritative symptoms after HoLEP is higher than TURP. Other study also reported dysuria was significantly more frequent in the HoLEP group than that in the TURP group. 36 This can be explained by the fact that the coagulated and necrotic tissues, which are not entirely removed during HoLEP have to slough off within weeks to months postoperatively. 37
Studies on sexual function after HoLEP and TURP are indeed lacking. Briganti et al 38 found a slight increase of IIEF (international index of erectile function) score and a significant higher retrograde ejaculation rate in each group, postoperatively. However, no significant difference was found between HoLEP and TURP groups on these parameters. Meanwhile, Gilling et al 23 also reported the similar data. Due to the lack of data, we did not assess sexual function in our meta-analysis.
It is reported that TURP has an increased risk of TUR syndrome, especially when treating a larger prostate,. 39 while HoLEP almost has no risk of the TUR syndrome since physiologic saline was applied as the irrigation fluid. 31 Among the six included studies, only Montorsi et al 21 reported one TUR syndrome in the TURP arm, while none in HoLEP. Therefore, it is impossible to assess the TUR syndrome rate between groups in our meta-analysis.
The prevalence of transient stress urinary incontinence after HoLEP has been reported to be as high as 44% and it might reduce the interests in adopting HoLEP as an alternative procedure. 40 However, Elmansy et al 41 reported that HoLEP-originated stress urinary incontinence is comparable to that of other surgical techniques for the treatment of BPH. Although in our meta-analysis, we did not find any significant difference in the incidence of stress urinary incontinence between the HoLEP and TURP group, we must keep in mind one thing: On multivariate analysis, prostate volume greater than 81 g, the presence of diabetes mellitus, and greater than 84% reduction in prostate-specific antigen were the risk factors associated with stress urinary incontinence. To prevent sphincter injury, it is essential for surgeons who are in the first stage of the learning curve to avoid performing HoLEP on large-size prostates.
Bipolar TURP and transurethral vapor resection of the prostate (TUVRP) are other commonly used techniques for treating BPH. It is reported that the functional outcomes of bipolar TURP and TUVRP are comparable to those of standardized TURP. 18,42 However, bipolar TURP enjoyed less complications and morbidity over standardized TURP. 42 According to Gupta N, 18 the catheterization time and blood loss with TUVPR is less than with TURP. Compared to HoLEP, bipolar TURP and TUVRP need shorter operation time. 18,31
Our findings must be interpreted within the context of several limitations.
First, some PVR, QoL, BPH recurrence, etc. data were unavailable in the original studies; this may limit the analysis of these outcomes compared to trials providing complete information.
Second, the follow-up time was different among studies, only two study conducted a 3-year and 7-year follow-up, respectively, and most studies were followed up for 1 year. Therefore, the long-term efficacy and safety (beyond 1 year) of HoLEP versus TURP cannot be evaluated due to a lack of data.
Third, great heterogeneity existed among studies; however, we did not carry out a meta-regression to further investigate the cause of heterogeneity. Instead, the random-effect model was introduced to analyze these data.
Fourth, the inadequate RCTs and patients in our meta-analysis might be another limitation.
Conclusion
Comparing with TURP, HoLEP showed slightly better postoperative results in Qmax and IPSS during the 12-month follow-up, as well as significantly better perioperative results and similarly low complication rates. However, the operative time and the incidence of postoperative dysuria favor TURP. Generally, HoLEP is a promising minimal invasive alternative to TURP for treatment of BPH.
Footnotes
Author Contributions
Lei Yin and Jingfei Teng had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Disclosure Statement
We certify that all conflicts of interest, including specific financial interests, relationships and affiliations relevant to the subject matter or materials discussed in the manuscript (e.g., employment/affiliation, grants or funding, consultancies, honoraria, stock ownership or options, expert testimony, royalties, or patents filed, received, or pending), are the following: None.