
Abstract
Background and Purpose:
Numerous holmium:yttrium-aluminum-garnet laser fibers are available for flexible ureteroscopy. Performance and durability of fibers can vary widely among different manufacturers and their product lines with differences within a single product line have been reported. We sought to evaluate a newly developed nontapered, single-use 240-μm fiber, Flexiva™ 200 (Boston Scientific, Natick, MA), during clinical use and in a bench-testing model.
Materials and Methods:
A total of 100 new fibers were tested after their use in 100 consecutive flexible ureteroscopic lithotripsy procedures by a single surgeon (B.K.). Prospectively recorded clinical parameters were laser pulse energy and frequency settings, total energy delivered and fibers failure. Subsequently, each fiber was bench-tested using an established protocol. Parameters evaluated for were fibers true diameter, flexibility, tip degradation, energy transmission in straight and 180° bend configuration and fibers failure threshold with stress testing.
Results:
The mean total energy delivered was 2.20 kJ (range 0–18.24 kJ) and most common laser settings used were 0.8 J at 8 Hz, 0.2 J at 50 Hz, and 1.0 J at 10 Hz, respectively. No fiber fractured during clinical procedures. The true fiber diameter was 450 μm. Fiber tips burnt back an average of 1.664 mm, but were highly variable. With laser setting of 400 mJ at 5 Hz, the mean energy transmitted was 451 and 441 mJ in straight and 180° bend configuration, respectively. Thirteen percent of fibers fractured at the bend radius of 0.5 cm with a positive correlation to the total energy transmitted during clinical use identified.
Conclusion:
Fiber performance was consistent in terms of energy transmission and resistance to fracture when activated in bent configuration. Fiber failure during stress testing showed significant correlation with the total energy delivered during the clinical procedure. The lack of fiber fracture during clinical use may reduce the risk of flexible endoscope damage due to fiber failure.
Introduction
With the advent of small-caliber flexible ureteroscopes that allow access and treatment of the previously inaccessible lower pole kidney stones, technical enhancement aimed at optimizing optical laser fibers flexibility and durability is ongoing by various manufacturing companies. Flexiva™ (Boston Scientific, Natick, MA) is FDA-approved Ho:YAG single-use fiber that is available in different core size diameters (Fig. 1). The FlexShield™ cladding for the Flexiva 200 fiber is designed to permit high-energy transfer even in tightly bent configurations, such as lower pole lithotripsy, and is rated by the manufacturer to handle power settings up to 50 W. The Flexiva 200 fiber has a 240-μm core size, which is unique among commercially available fibers. The 240-μm core allows for a nontapered guided connector to be utilized. A previous testing has shown that tapered connecters introduce additional variability in fiber performance. 4,5,8

The Flexiva™ 200 (Boston Scientific) nontapered, single-use 240 μm laser fiber.
We have demonstrated in a previous testing that fibers performance and durability can vary widely among different manufacturers and their product lines. 4 Furthermore, differences in performance characteristics within a single product line from the same manufacturer may be detected. 5 In light of these results, our objective in the current study is to evaluate the performance characteristics of the newly developed Flexiva 200 fiber during both clinical use and when using an established bench testing protocol. 4,5
Materials and Methods
A total of 100 brand new Flexiva 200 (Boston Scientific) single-use nontapered Ho:YAG optical fibers were used for 100 consecutive flexible ureteroscopic lithotripsy procedures done by a single surgeon (B.K.). All fibers were purchased by the hospital from the manufacturer. Clinical data from each case were prospectively recorded and included laser pulse energy and frequency settings, total energy delivered per procedure, and any occurrence of fiber clinical failure, defined by fiber fracturing during ureteroscopy. A Lumenis (Santa Clara, CA) VersaPulse® 100 W laser was used for all clinical procedures.
Following their clinical use, each individual fiber was tested in the laboratory in a standardized fashion. First, the true fiber diameter, that is, the total diameter of the fiber optical core, the cladding layer, and the surrounding outer protective jacket was measured using a digital micrometer (Mitutoyo, Tokyo, Japan) calibrated within±1 μm. Fiber flexibility was then assessed using a Stryker U-500 flexible ureteroscope. The baseline ureteroscope maximal deflection angle was measured with an empty 3.6F working channel. This was achieved by fully activating the primary deflection followed by the secondary deflection to allow for ureteroscope maximal deflection angle to be achieved. Then, the Flexiva 200 laser fiber was inserted into the working channel and any reduction in the scope maximal deflection from the baseline was recorded. The average value from repeated measurements was documented.
Fiber optical tip degradation (fiber burnback) defined as the change in core fiber length after use in the clinical procedure, was measured. The distance from the fiber tip to the cladding edge was taken on four new fibers as a baseline reading (Fig. 2). Using the digital micrometer, the optical tip of the fiber was measured and the percentage of undamaged tip length remaining was calculated. A statistical analysis was performed evaluating the amount of fiber tip degradation with the laser energy and pulse frequency settings as well as the total energy delivered per procedure.
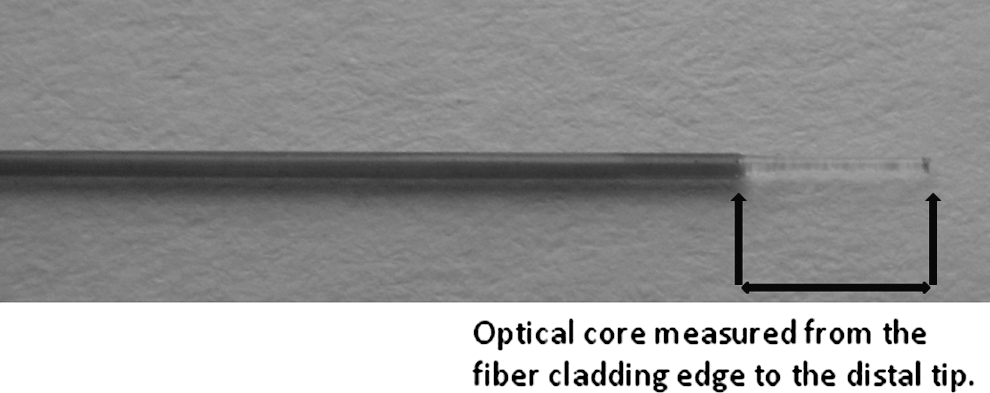
The Flexiva 200 fiber tip measurement.
Fiber energy transmission was evaluated in both straight and 180° bend configuration. Briefly, following fiber stabilization in the tested configuration, a Dornier (Wessling, Germany) Medilas H20 Ho:YAG laser was activated at energy setting of 400 mJ at 5 Hz. Energy output at the fiber tip was measured with an energy detector (Convergent Technologies, Alameda, CA). The averaged value of 50 pulses was recorded on each fiber in both configurations.
Fiber failure threshold was assessed with stress testing while energy transmitting. Each fiber was bent to 180° with an initial bend radius of 1.25 cm. The VersaPulse100 W Ho:YAG laser was activated at 1200 mJ at 10 Hz for 30 seconds. If no fiber failure occurred, testing was repeated with the bend radius reduced in 0.25-cm increments until fiber failure or a radius of 0.5 cm was achieved. Fibers that failed stress testing were compared to those that did not in terms of total energy delivered during their clinical usage. The fiber connector end was monitored during bench testing periodically with an infrared thermometer (Raytek®) to detect any increase in temperature.
The laser used for treatment and during testing has been serviced and calibrated with the rods aligned before study initiation. A Student's t-test and a two-way analysis of variance test were used for energy transmission and frequency setting comparisons, respectively. Statistical significance was defined as a p<0.05 for all tests and comparisons.
Results
Clinical performance
One hundred Flexiva 200 fibers were opened during consecutive flexible ureteroscopy procedures. Ninety-six of the 100 fibers were used during the procedures to treat renal calculi. In four cases, the fibers were opened from their sterile packaging, but not used due to successful basket extract of the calculi. Results for the clinical parameters evaluated are listed in Table 1. No fiber fractures occurred during the clinical cases. The mean total energy delivered was 2.20 kJ (range 0–18.24 kJ) and the most common laser settings used were 0.8 J at 8 Hz (49%), 0.2 J at 50 Hz (18%), and 1.0 J at 10 Hz (9%). Fiber tips burnt back an average length of 1.664 mm (range 0–4.552 mm), but the amount was highly variable with 66% of fibers retaining greater than half of their initial tip length following clinical use. Comparing fibers that burnt back more than the average (n=42) to the rest of cohort (54), no correlation to total energy transmitted during lithotripsy (p=0.88) was identified; however, a trend was noted between the burnback length and the laser settings, but it did not reach a statistical significance (p=0.07).
Bench testing performance
Results of the Flexiva 200 optical fiber bench evaluation are summarized in Table 2. The measured true fiber diameter was 450 μm. The baseline deflection of the Stryker U-500 ureteroscope was 275°. When inserted into the working channel, the Flexiva 200 fiber decreased the ureteroscope maximal deflection angle to 270° (Fig. 3). With the laser set at 400 mJ at 5 Hz, the mean energy transmitted was 451 and 441 mJ in a straight and 180° bend configuration, respectively (p=0.38). Eighty percent of fibers transmitted at least 400 mJ in either configuration. The fibers connector end did not show any increase above room temperature throughout testing. In terms of fiber failure threshold, 13% of fibers fractured at only the tightest bend radius of 0.5 cm during energy transmission. No fiber failed with bending alone. The remaining 87% of fibers did not fracture during bench testing. No fibers failed at bend diameters greater than 0.5 cm, and no fibers failures at the connector end occurred. For fibers that failed the stress testing, there was statistically significant difference in the amount of total energy that had been delivered during clinical use by these fibers (p=0.02). The mean total energy delivered by fibers that failed bend testing was 4.47 kJ (range 0.01–18.24 kJ) compared to 1.86 kJ (range 0–18 kJ) transmitted by those that did not fail.
The Flexiva 200 fiber flexibility assessment.
Baseline ureteroscope deflection was 275°.
Discussion
The ideal laser fiber for flexible ureteroscope should meet certain criteria. First, it should have a small true diameter. The small size fiber will allow better visualization of lithotripsy targets during ureteroscopy by increasing irrigant flow rate according to Poiseuille's equation. 4 Given the small fiber size, an increase in irrigation flow might be achieved without compromising scope deflection ability. 9 –11 While we have not encountered irrigation or visibility problems during the flexible ureteroscopic lithotripsy procedures, the Flexiva 200 fiber has a measured true fiber diameter of 450 μm. When compared to the true diameter of the current small core fibers, the 450 μm diameter is relatively large and comparable to the true diameter of fibers that have 270-μm core size, such as the SureFlex LLF-273 fiber. 5 According to the manufacturer, the smaller 240-μm core allowed them to use a thicker cladding (FlexShield) to increase the durability of the Flexiva 200 with the trade off being that the true diameter is similar to other fibers with 270-μm cores. The information on the package of the fiber varies among manufacturers. For the Flexiva 200 fiber, Boston Scientific neither the diameter of the core nor the total diameter of the fiber, cladding and jacket are listed, but rather only the maximum power rating of 50 W is stated. This lack of information on the fiber package may be misleading to the end user. We have previously proposed that fiber manufacturers standardize reporting of information on the packaging of fibers and include the power rating, the diameter of the core, cladding and jacket in μm, the numerical aperture (which reflects the acceptance angle and beam divergence), whether the fiber is tapered or not, and whether it is single use or reusable. 4,5 Fiber manufacturers should operate with transparency and include this information to allow for a fair comparison between products and not rely on misleading marketing names. The Flexiva 200 fiber comes packaged in a plastic circular holder, similar to what a guidewire comes in (Fig. 1). We have found this to be ergonomic and simplified the handling of the fiber in the operative room. We also pass the fiber across the leg of the draped patient, and then place a wet towel on top of the laser fiber to hold it securely. We have found this system secures the fiber and limits inadvertent damage to it during procedures.
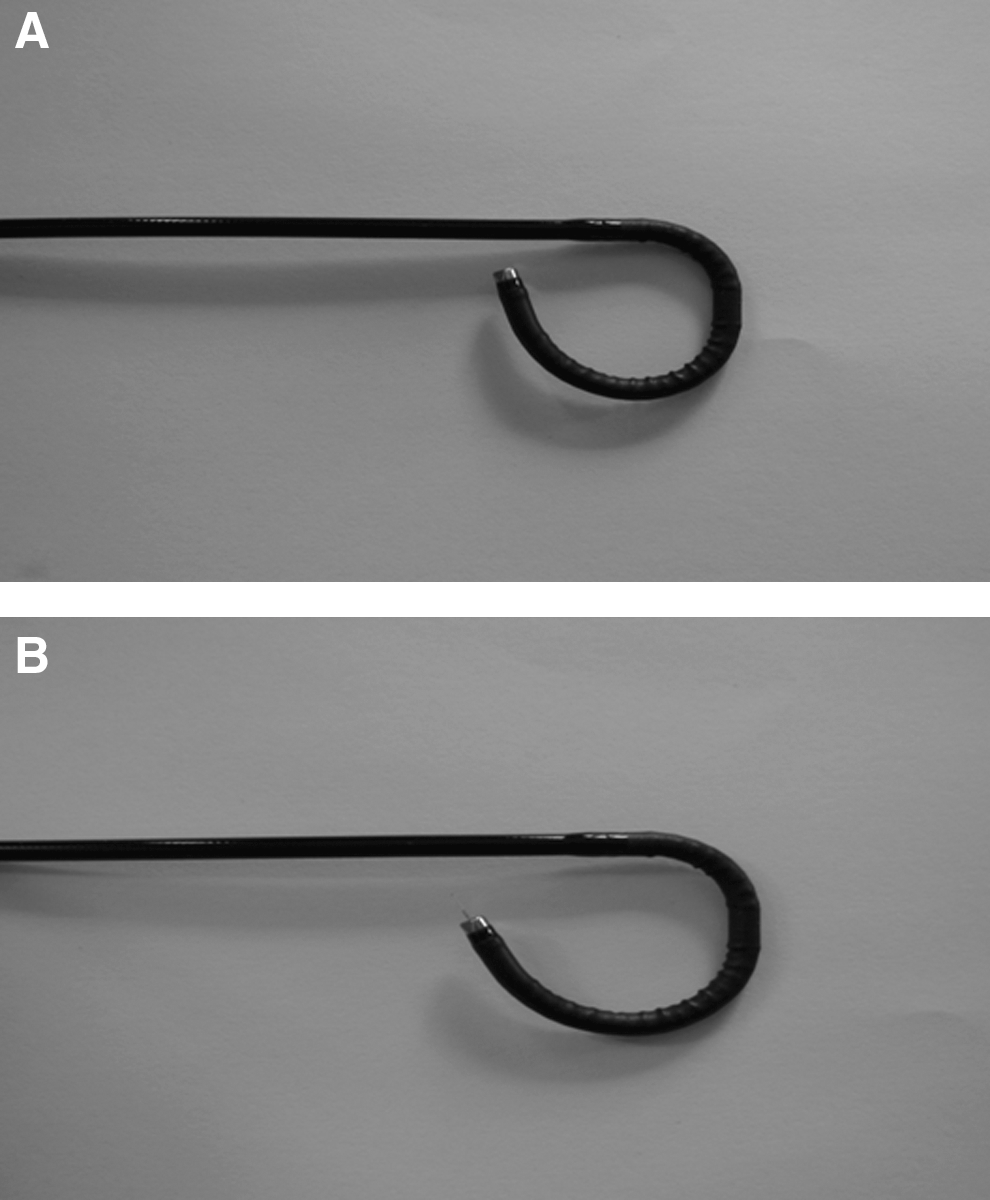
Unfortunately, small-size fibers have been reported to have an increase failure rate when the laser pulse energy increases. 12 Failure during clinical procedures could lead to endoscope damage. If a portion of the fiber breaks off, extraction of the fiber piece can be very challenging. It is theorized that fiber failure occurs by increase in energy evanescence, a phenomenon by which more photons extend beyond the core–cladding interface. 4,13 The fluorine-doped fused silica cladding should have a refractive index lower compared with the fiber core to protect the silica core from optical damage and help minimizing fiber failure. A high refractive index for the cladding will increase amount of photons that are reflected at the core–cladding interface by the total internal reflection process. 14 Subsequently, an increase in the photon total internal reflection will minimize the amount of laser energy escaping into the cladding and the fiber jacket. 13 Ultimately, preventing the laser energy from entering the fiber jacket will prevent thermal breakdown and fiber fracture. Compared to our previous testing of new small core size fibers, Flexiva 200 fiber failure threshold during bench testing was on par with the best fibers tested. 4,5 Whether this low rate of fiber failure can be attributed to the new FlexShield cladding of the new fiber is not known, but the fiber design appears to be robust with only 13% of the fibers failing at a bend radius of 0.5 cm, which is tighter than what can be achieved by bending in current generation flexible ureteroscopes (Fig. 4).
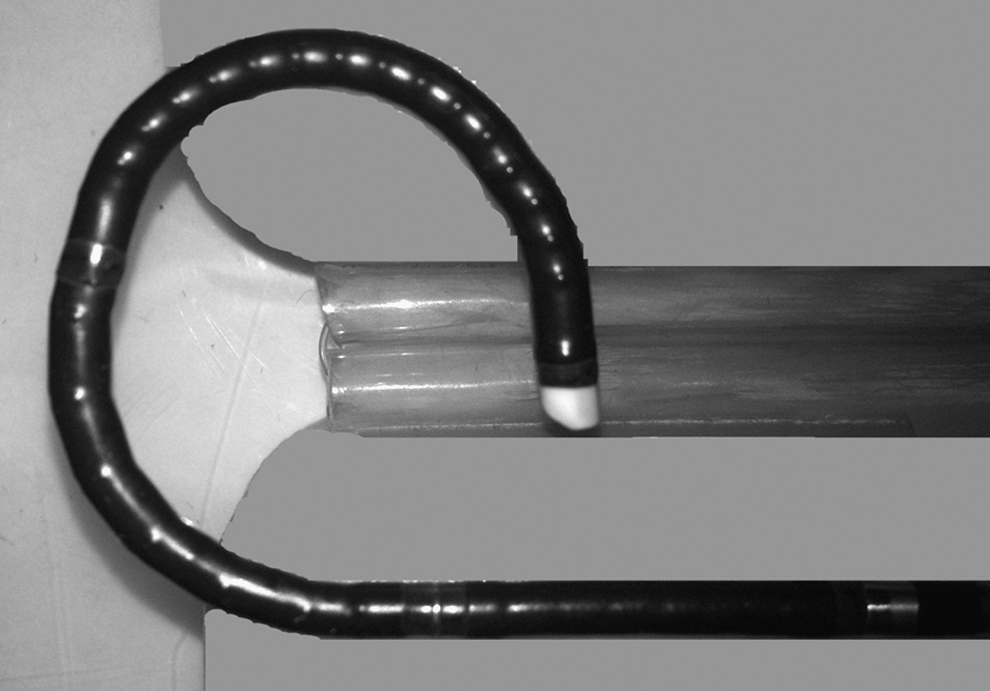
Comparison of bend diameter of URF-P5 ureteroscope to the bend diameter required for Flexiva 200 fiber failure.
Another criterion for an ideal laser fiber for flexible ureteroscopy is its degree of flexibility. Urologists require a laser fiber that does not limit the deflection of flexible ureteroscopes, thereby not reducing access into difficult to reach areas, such as the lower pole. The Flexiva 200 fibers demonstrated to be highly deflectable and only limited the deflection angle of the Stryker U-500 endoscope by 5°. This compares favorably to the previously tested nontapered sub-200-μm fibers, such as the BSci Accuflex 150 fiber. 5
Small-diameter laser fibers with core sizes of less than 300 μm carry the risk of proximal fiber failure at the connector end. 13 This is especially common for fibers that overfill or when there is a misalignment at the subminiature version A connector (SMA) and the laser. 8 Whereas a tapered connector may lower the risk of fiber failure at the connector end by better coupling of the laser to the fiber and acting as funnel aiding smooth delivery of laser energy into the core; 3 however, this increases the complexity of the fiber design. Our previous testing has shown that the tapered fibers were more likely to fail at the connector end than the similar size, nontapered fibers. 4 It is postulated that the tapered connector end may convert off-axis laser rays into higher order rays, which can exceed the fiber numeric aperture size resulting in fiber failure at the proximal connector end. Furthermore, the high-order rays may also increase the evanescent laser waves downstream and lead to failure at points of maximal deflection. 8,13 The Flexiva 200 fiber has a nontapered connector end and a core size diameter of 240 μm, which is smaller than the input spot size of the Lumenis and Dornier lasers used in this study. Although not tapered, the manufacturer reports the connector guides the energy into the core of this fiber. With no fiber failing during clinical use, including no connector end failures, and with both no connector end failures during bench testing nor any increase in temperature, it appears that this fiber couples well with both the Lumenis VersaPulse 100 laser used during clinical procedures and the Dornier Medilas H20 laser used during bench testing.
Fiber tip degradation (burnback) may occur during Ho:YAG laser lithotripsy. 12,15 If it happens, it may impact stone fragmentation efficiency and may require the surgeon to pause and re-cleave the fiber, thereby increasing operative time. 16 The exact mechanism by which fibers burn back their tips is still not fully understood; however, it has been hypothesized that fiber tip degradation relate to the absorption of laser energy by adherent carbonaceous material at the core tip; this could increase the fiber tip temperature and causes melting of the silica core material. 13 Mues et al examined different types of Ho:YAG optical fibers with a variety of core size diameters in a bench testing experiment. 17 The fibers were submerged in water and the laser was activated at 1.2 J and 10 Hz for 180 seconds. The amount of burnback of the fiber tip was measured with and without fiber contact with an artificial Bego stone. The authors concluded that fibers burnback occurred when the tip of the fiber is brought into direct contact with the stone. Our approach during flexible laser lithotripsy is to not bury the fiber tip into the stone, but rather paint the stone surface with the laser and work on a broad front. During our clinical use of the Flexiva 200 fibers, we measured a variable degree of burnback. We attempted to correlate the burnback to either the laser energy and pulse frequency settings used as well as the total energy delivered, but were not able to. The variable degree of burnback may be related to differences in stone composition, but we were unable to assess this as we did not have enough stones of pure composition to allow for a meaningful statistical analysis. Future bench testing with stones of known composition may shed further light on this area. Another possible variable is whether some differences between fibers could be introduced during the manufacturing and packaging process. We did not specifically assess this, but all the fibers in this study were off the shelf and not specifically provided by the manufacturer for our testing.
We have previously demonstrated that the reusable Ho:YAG optical laser fibers are more cost-effective than their single-use equivalants. 6 The Flexiva 200 is a single-use fiber and if compared to the similar size re-usable fibers, it might be more expensive on the long term. However, the use of this fiber eliminates the need for reprocessing and repackaging should a reusable fiber was used clinically. Additionally, the new design of this fiber appears to be robust as demonstrated by our bench testing. Lastly, when considering that no fibers failed during clinical use, the overall procedural cost may be reduced by minimizing the scope damage and the associated high costs of repair.
While the performance characteristics of this new Ho:YAG optical fiber are promising, we encourage laser fiber manufacturers to continue their efforts in creating more ideal fibers that would help urologist to address any unforeseen needs during endoscopic lithotripsy procedures.
Conclusions
The Flexiva 200 fiber performed well in both clinical and bench testing settings. No fibers failed during 96 consecutive laser lithotripsy procedures. Bench testing of this fiber demonstrated that it performed on par with the best fibers tested. The fiber did demonstrate a variable degree of burnback during clinical procedures and is an area where performance of this fiber could be improved.
Footnotes
Disclosure Statement
Dr. Knudsen is a consultant for Boston Scientific, and a hands-on course instructor for Storz and Cook. Dr. Teichman received research support from Cook Urologic and Boston Scientific. For all other authors, no competing financial interests exist.