
Abstract
Purpose:
We present our initial experience with microperc in patients with moderate-size renal calculi.
Patients and Methods:
A retrospective analysis of 30 patients (male 14, female 16) with moderate-size (1–3 cm) kidney stones who underwent microperc between August 2011 and July 2012 was performed. The demographic values, perioperative and postoperative measures including age, stone size and location, body mass index, operative and fluoroscopy time, hemoglobin decrease, success and complication rates were prospectively recorded into a patient entry system.
Results:
The average stone size was 17.9±5.0 mm (10–30 mm). The mean age of the patients was 41.5±18.2 years (range 3–69 years). The duration of the operation was calculated as 63.5±36.8 minutes (range 20–200 min). Mean fluoroscopic screening time was 150.5±90.4 seconds (range 45–360 seconds). The patients were discharged after a mean hospitalization period of 35.5±18.6 hours (range 14–96 hours). An overall success rate of 93% (including 10% of insignificant residual fragment rate) was achieved. In the follow-up, residual stone fragments were detected in two (7%) patients. Conversion to miniperc was necessitated in three (10%) patients. The mean hemoglobin drop was found to be 1.1±0.8 mg/dL (range 0–2.8 mg/dL). Complications were observed in five (13.3%) patients.
Conclusions:
Our initial results provide that microperc is a feasible, safe, and efficacious treatment modality for moderate-size kidney stones as well as small ones with its minimally invasive nature. Technical refinements are needed to achieve better results and overcome the limitations of technique.
Introduction
With the technologic advances of the endolithotripters and miniaturization in the instrument size, different treatment modalities such as flexible ureterorenoscopy and miniperc have been popularized in the management of small and/or medium sized renal calculi. 3 –6
Despite the high success rate of PCNL, the complication rates are reported in the range of 29% to 83% in different series. 7,8 Bleeding may sometimes be a worrisome complication that generally occurs during tract dilation. Therefore, to prevent hemorrhage, the idea of using less traumatic and finer instruments has led to the improvement of novel devices.
Micropercutaneous nephrolithotomy (microperc) has recently been introduced as a treatment modality in which percutaneous renal access is achieved under direct vision using a specialized optical puncture system called “all-seeing needle” (Figs. 1, 2). 9 The main advantage of this technique is its smaller size and the single-step performance without the necessity of tract dilation. Desai and associates 10 have just published their initial experience with this modified PCNL technique in 10 patients with renal calculi with a mean size of 14.3 mm. Recently, Tepeler and colleagues 11 presented the feasibility of microperc in the management of symptomatic lower pole renal calculi, which is a challenging issue. No study has been conducted, however, regarding the management of moderate-size stones until now.
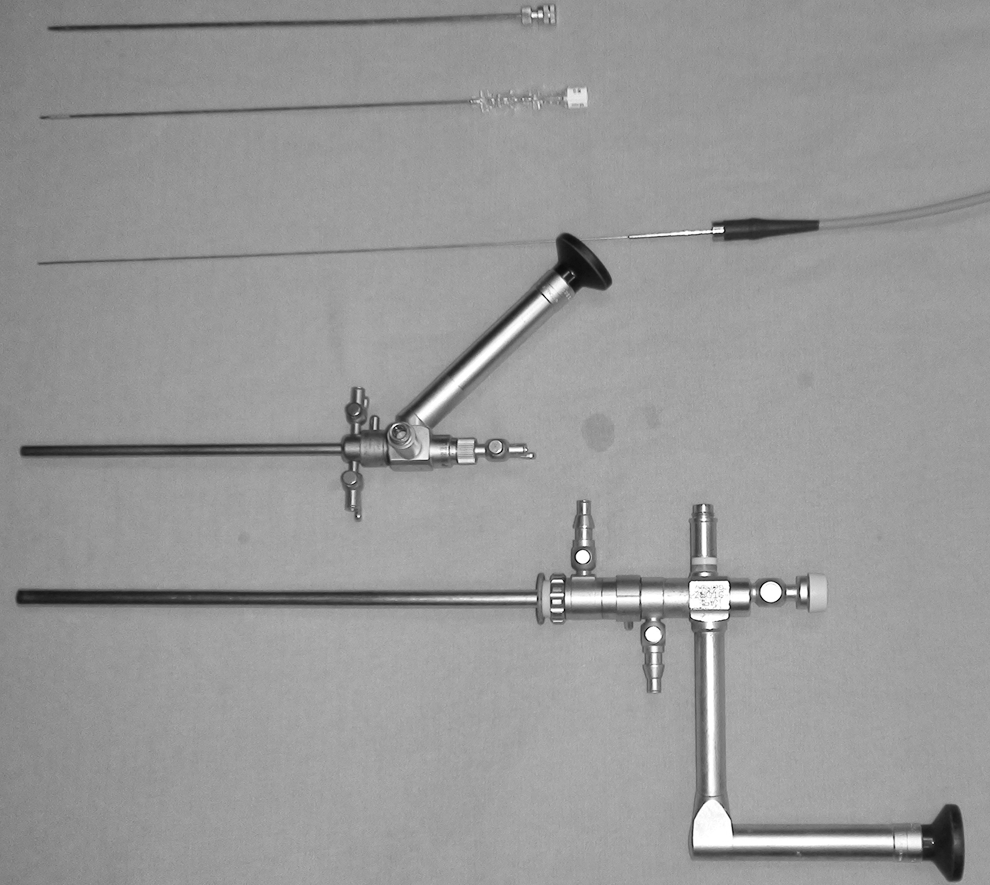
The 8F microsheath, 16-gauge microperc access needle, 0.9-mm microfiber optic, 17F mininephrocope, and 24F nephroscope.
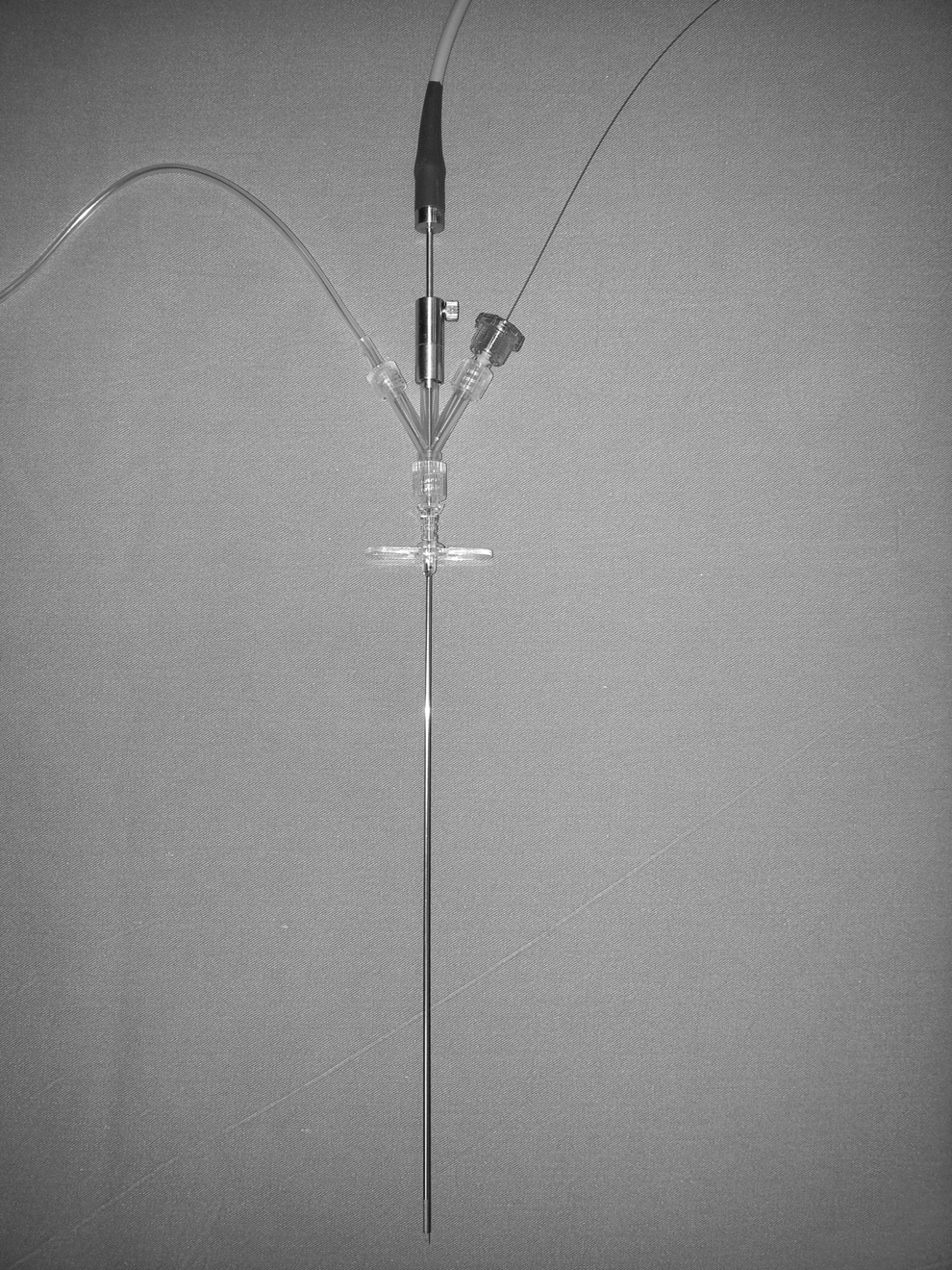
The microperc system: A three-way connector is attached to the distal tip of the 4.8F microshaft.
We present our initial experience with microperc in patients with moderate-size renal calculi. To our knowledge, this is the first and the largest clinical study introducing the safety and feasibility of this new modality in relatively large-size kidney stones.
Patients and Methods
A total 30 patients (male 14, female 16) with moderate-size (1–3 cm) kidney stones underwent micro-PCNL between August 2011 and July 2012. The demographic values, perioperative and postoperative measures including age, stone size and location, body mass index (BMI), operative and fluoroscopy time, hemoglobin decrease, success and complication rates were prospectively recorded into a patient entry system. The study was approved by the local ethics committee.
Preoperative evaluation included detailed history, physical examination, routine biochemical tests, creatinine level, complete blood cell count, coagulation profile, and urinalysis. Whenever detected, positive urine cultures were treated with appropriate antibiotics preoperatively. The patients were evaluated with radiography of the kidneys, ureters, and bladder (KUB), ultrasonography, and intravenous pyelography and/or CT preoperatively. The stone size was assessed by measuring the longest axes of the stone or sum of the axes of the multiple stones.
Surgical technique
After the insertion of a 6F open-end ureteral catheter with the patient in the lithotomy position, the patients were turned into the prone position allowing the use of fluoroscopy when necessary. The renal collecting system was distended with the instillation of contrast medium via the ureteral catheter. Renal access was achieved by two experienced urologists (AT, AA) in PCNL using the micro-optical system (PolyDiagnost, Pfaffenhofen, Germany) under fluoroscopy as described previously. 9 –11 Then, the three-way connector was adapted to the proximal side of the instrument (Fig. 2). The stone fragmentation was accomplished using a 200-μm holmium:yttrium-aluminum-garnet laser fiber (Quanta System, Group Italy) with the settings of 0.8 J at 8 Hz (6.4 W) under direct visualization (Fig. 3). The safety of the procedure was maintained without a need for a safety guidewire, because all manipulations were performed under direct vision. The maintenance of vision and clearance of stone fragments was provided by an irrigation pump-system controlled by the surgeon.
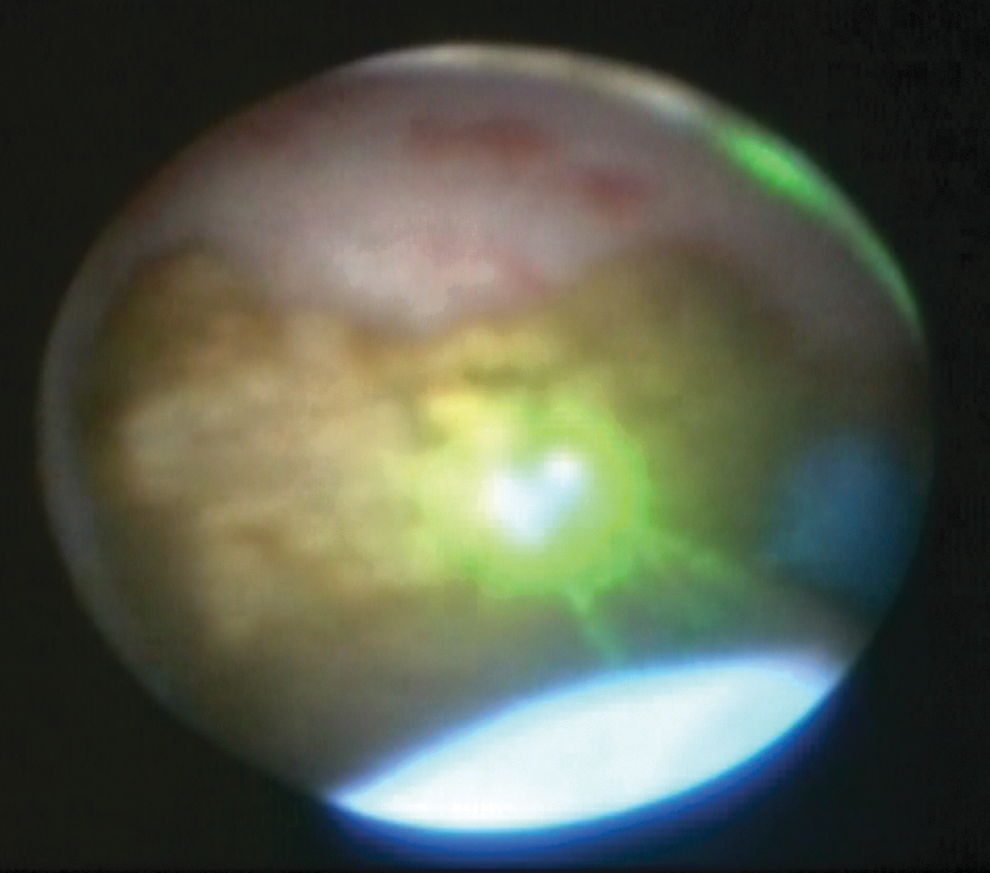
The stone disintegration with laser fiber under direct vision in the pelvis.
In patients with renal calculi larger than 2 cm, an 8F microsheath that allows better manipulation, use of a larger laser fiber, insertion of a Double-J stent in antegrade fashion, and stone retrieval with a basket was preferred. 11 In those cases, the 8F sheath was placed over a guidewire that was previously inserted through the access needle under fluoroscopy guidance. Subsequently, the micro-optical system was inserted through the sheath.
The ureteral catheter was removed on postoperative day 1 in all cases. After the mobilization of the patient and evaluation of the stone-free status with radiography of the KUB, the patients were discharged within 24 hours if no complication occurred. The patients were reevaluated with CT after 1 month. The asymptomatic, nonobstructive and noninfectious stone fragments ≤4 mm were accepted as “clinically insignificant residual fragments” (CIRF). 12 Complications were classified according to the Clavien system. 13 The values were presented as the mean±standard deviation.
Results
The mean age of the patients was 41.5±18.2 years (range 3–69 years). Seventeen of the patients had a history of failed shockwave lithotripsy, and 2 patients had a history of failed ureteroscopy. The average stone size was 17.9±5.0 mm (range 10–30 mm). The majority of the stones were radiopaque except for four radiolucent stones. The accompanying anatomic abnormalities were horseshoe kidney (n=1), pelvic kidney (n=1), and kyphoscoliosis (n=1). The stones were located in the pelvis, lower pole, midpolar, upper pole, and pelvis, in 4, 16, 2, 1, and 7 patients, respectively. The demographic values of the patients are summarized in Table 1.
SD=standard deviation; BMI=body mass index.
The stone disintegration was accomplished using 4.8F or 8F microsheaths in 16 and 14 patients, respectively. The duration of the operation was calculated as 63.5±36.8 minutes (range 20–200 min). The longest operative time was 200 minutes in a 3-year-old girl with a pelvic kidney stone who underwent laparoscopic-assisted microperc. The mean fluoroscopic screening time was 150.5±90.4 seconds (range 45–360 seconds). The patients were discharged after a mean hospitalization period of 35.5±18.6 hours (range 14–96 hours). The perioperative data are listed in Table 2.
CIRF=clinically insignificant residual fragment; PCNL=percutaneous nephrolithotomy.
An overall success rate of 93.3% (including 10% of the CIRF rate) was achieved. In three (10%) patients, conversion to mini-PCNL was necessitated because of bleeding leading to impairment of vision (n=1) and maneuvering disability to reach the displaced stone fragments (n=1) and high stone burden (n=1). In the follow-up, residual stone fragments were detected in two (6.7%) patients.
The mean decrease in hemoglobin level was found to be 1.1±0.8 g/dL (range 0–2.8 g/dL). Transfusion was not needed in any of the patients. Complications were observed in five (13.3%) patients. Intravasation of the irrigation fluid leading to abdominal distention was managed intraoperatively with percutaneous drain placement in a patient with an impacted pelvic stone (Clavien grade IIIb complication). Although medical treatment was sufficient in two patients with postoperative renal colic (Clavien grade I complication), Double-J stent placement was needed for two patients with persistent postoperative renal colic related to stone fragments (Clavien grade IIIa complication) (Table 2).
Discussion
The treatment of patients with renal stone disease has dramatically changed, and endoscopic methods have been popularized with their minimally invasive nature. Today, the endoscopic treatment modalities are being performed with finer instruments with the aim of reducing the complication, morbidity, and mortality rates. The indications for endourologic procedures (PCNL and flexible ureteroscopy) have been extended in the recent European Association of Urology guidelines. 2 PCNL, however, is still accepted as the primary treatment modality for moderate- and large-size renal calculi.
With the effort to reduce renal trauma, two researchers have initially reported the results of the miniperc technique by using smaller (11–15F) vascular sheaths. 14,15 The miniperc is the procedure performed with the same technique using smaller-size instruments ranging 12F to 20F (Fig. 1). 16 The investigations comparing the outcomes of miniperc vs standard conventional PCNL revealed that the miniperc is significantly superior to PCNL regarding bleeding and hospitalization time. 3,17 Although there is still a debate about the advantages of miniperc, one might predict that the size of the tract used for access may affect the hemorrhagic complications. 18
Recently Bader and coworkers 9 have reported the smallest size (Fig. 4) of optical puncture system to obtain a safe and optimal renal access. In that study, they successfully achieved renal access under direct vision with the all-seeing needle in 15 patients. This way, they avoided the complications related to access such as adjacent organ injury, intraoperative bleeding, and perforation of the collecting system. In the next step, Desai and colleagues 10 have advanced and initially used this system to fragment small kidney stones with a mean size of 14.3 mm through a 4.85F tract in 10 patients and named this procedure: “microperc.” In this technique, after performing a proper access with visual control and removal of the beveled inner needle, the stone disintegration was achieved with a laser fiber inserted through the three-way connector attached to the proximal end of the needle. In a multicentric study, Tepeler and coworkers 11 have recently published the outcomes of microperc for lower pole stones. 11 Similarly, in the present study, we performed microperc in 30 patients with moderate-size kidney stones with the stone-free rate of 83.3%. This is the largest study from a single institute that presents the feasibility of microperc for 1- to 3-cm renal calculi.

The comparison of different sizes of nephroscope shafts (4.8F, 8F, 17F, and 24F shafts) that allow stone disintegration.
Bleeding is a major complication of PCNL with the incidence of 0.8% to 45% in the literature. 8,18 –22 The size and the multiplicity of the tract, stone size, and presence of diabetes are found to be the main factors affecting blood loss. It has been suggested that bleeding generally occurs during access creation, dilation, or stone disintegration phases of PCNL. 8,19 –21 Therefore, it is believed that microperc may minimize this risk because of its size and the single-step performance. In the series of Desai and colleagues, 10 the mean hemoglobin drop was calculated as, 1.4±1.0 g/dL. 10 In the other series, the mean hemoglobin drop was 0.8±0.6 g/dL for lower pole stones. 11 In the present study, blood transfusion was not required for any of the patients, and the mean hemoglobin drop was 1.1±0.8 g/dL. Hence, it is also our impression that microperc may minimize the risk of bleeding. On the other hand, although bleeding rarely occurs, vision is easily affected even by minimal bleeding because of low resolution of the optical system. This may lead to failure of the procedure, especially in patients with larger renal stones. In a patient with intraoperative bleeding leading to impairment of vision, conversion to miniperc was needed in our series.
Microperc have some different technical details from the standard PCNL or miniperc that need to be discussed. The smallest size of the access sheath used for miniperc was 11F whereas microperc is performed through a 4.8F needle that permits a safety access and stone disintegration. Although this technique is very successful for small calculi, some technical modifications may be needed for larger stones. The body of the 4.8F shaft is very fine and is not feasible for some conditions needing excessive torque. To overcome this limitation, we have used an 8F microsheath in patients with stones larger than 2 cm. The 8F microsheath allows the use of a larger laser fiber, removal of stone fragments using a basket catheter, placement of a 6F catheter for drainage in the presence of pelvicaliceal perforation, and placement of a Double-J stent in an antegrade route. 10,11 We have used 4.8F and 8F microsheaths in 16 and 14 patients, respectively. On the other hand, in one patient with a displaced stone that was not reached with the 8F sheath, conversion to miniperc was needed.
The short duration of operation, hospitalization, and fluoroscopic imaging are the other advantages of microperc. The phase of tract dilation is time consuming and necessitates fluoroscopic imaging. This phase and associates are excluded in the microperc technique. In the present study, the operation and fluoroscopy times were calculated as 63.5±36.8 minutes and 150.5±90.4 seconds, respectively. In addition, the lack of postoperative nephrostomy is an important factor decreasing the hospital stay and pain. 23 In our series, we have found that the mean hospital stay was 35.5±18.6 hours.
The microperc is based on the principle of “break and leave,” similar to the retrograde intrarenal surgery of renal calculi. The lack of stone extraction after disintegration might be considered as a limitation factor for microperc. We have succeeded, however, in retrieving stone fragments for analysis using a basket catheter through the 8F microsheath in an 8-year-old girl.
Although the clearance of stone fragments is facilitated by irrigation during surgery, 10,11 these fragments may lead to renal colic episodes postoperatively, especially in patients with large renal stones. At the beginning, we witnessed renal colic episodes in four of our patients. The renal colic resolved with medical treatment in two, and stent placement was performed in the other two patients. After this experience, we decided to routinely insert a Double-J stent in patients with ≥2 cm renal stones in antegrade (n=4) or retrograde fashion (n=10) during the procedure. Finally, none of our patients experienced renal colic afterward.
The other point that needs to be underlined is balancing the intrarenal pressure. The prolonged pressurized irrigation during the procedure could increase the intrarenal pressure if sufficient drainage of the collecting system is not provided via the ureteral catheter. Although Desai and associates 10 inserted 5F ureteral catheter in their series, we placed a 6F open-end ureteral catheter that provides better drainage to overcome this limitation. In a child with an impacted renal pelvis stone, however, we have observed abdominal distention and intravasation of the irrigation fluid. The patient was treated with ultrasonography-guided percutaneous drain placement intraoperatively. The drainage of the collecting system and placement of large ureteral catheter plays a key role in preventing the complications associated with high intrarenal pressure. In obstructed systems with impacted calculi, mini or standard PCNL seems to be safer than microperc.
Conclusion
This is the first and the largest study presenting the outcomes of microperc in the management of renal calculi with the size of 1 to 3 cm. Our initial results provide that microperc is a feasible, safe, and efficacious treatment modality for moderate-size kidney stones as well as small ones with its minimally invasive nature. Technical refinements are needed to achieve better results and to overcome the limitations of the technique.
Footnotes
Disclosure Statement
No competing financial interests exist.