
Abstract
Background and Purpose:
Renal preservation in selected patients with upper-tract urothelial cancer (UTUC) has been well described, offering an alternative to radical nephroureterectomy. We present our experiences in performing percutaneous treatments after neoadjuvant chemotherapy in one such patient with a large, complex, high-grade UTUC in a solitary kidney.
Case Report:
A 55-year-old woman with a solitary kidney presented with a 5.2 cm enhancing mass with calcifications involving the left renal pelvis and lower pole. Cystoscopy and retrograde pyelography demonstrated normal bladder mucosa. Ureteroscopy revealed a large, papillary tumor occupying the renal pelvis. Ureteroscopic treatment was deemed impossible because of the lesion's volume. We proceeded with percutaneous resection after downsizing the tumor after a course of neoadjuvant chemotherapy. Using a 25F resectoscope via a percutaneous tract, resection was performed to fully excise the tumor, and the patient received two postoperative chemotherapy courses. A recurrence developed within an isolated calix 8 months postoperatively, which was also managed percutaneously.
Conclusion:
A multimodal approach in a highly motivated patient could represent a reasonable strategy for patients in whom such a therapy is desired.
Introduction
Radical nephroureterectomy (RNU) has long been the mainstay of therapy for UTUCs, which are multifocal, extremely large, or of high tumor grade, but there exist many indications in which maximal preservation of nephrons is desirable. In recent years, coincident with improvements in endoscopic equipment and cross-sectional imaging, ablative renal-sparing surgery has become increasingly popular for the management of low-grade, noninvasive upper-tract tumors. This conservative approach has been applied in selected cases when nephron sparing for preservation of renal function is needed, such as in patients with a solitary kidney or with simultaneous bilateral tumors. 3
We present our experiences in performing percutaneous treatments in one such patient with a complex, high-grade UTUC in a solitary kidney.
Case Report
A 55-year-old woman, with a surgical history significant for a right RNU for UTUC 6 years previous and a familial history of Lynch syndrome, presented with new gross hematuria. Her metabolic evaluation revealed normal renal function (serum creatinine concentration 0.7 mg/dL; glomerular filtration rate >60 mL/min). CT demonstrated a 5.2 cm enhancing mass with calcifications involving the left renal pelvis extending into the calices of the lower pole of the kidney and no evidence of lymphadenopathy (Fig. 1).

Initial CT scan, stent in place; 5.2 cm enhancing, partially calcified, left renal pelvis and lower pole mass.
Cystoscopy and retrograde pyelography showed a normal bladder without lesions and a filling defect within the renal collecting system. A large papillary UTUC occupying the renal pelvis was encountered, and biopsies were performed; pathologic evaluation confirmed papillary high-grade transitional-cell carcinoma (TCC). After discussion regarding treatment options, the patient was adamant in refusal of nephroureterectomy. Chest CT scan and metastatic workup produced negative findings. Because of the lesion size and high-grade nature, the plan was made for neoadjuvant chemotherapy using gemcitabine and cisplatinum to try to downsize the lesion to make percutaneous resection possible. With neoadjuvant therapy, progressive reduction of the lesion size on follow-up imaging was observed through treatment. The tumor decreased to 2.4 cm size (Fig. 2), without further decrease between cycle 4 and 5. She was then brought to the operating room for percutaneous resection.
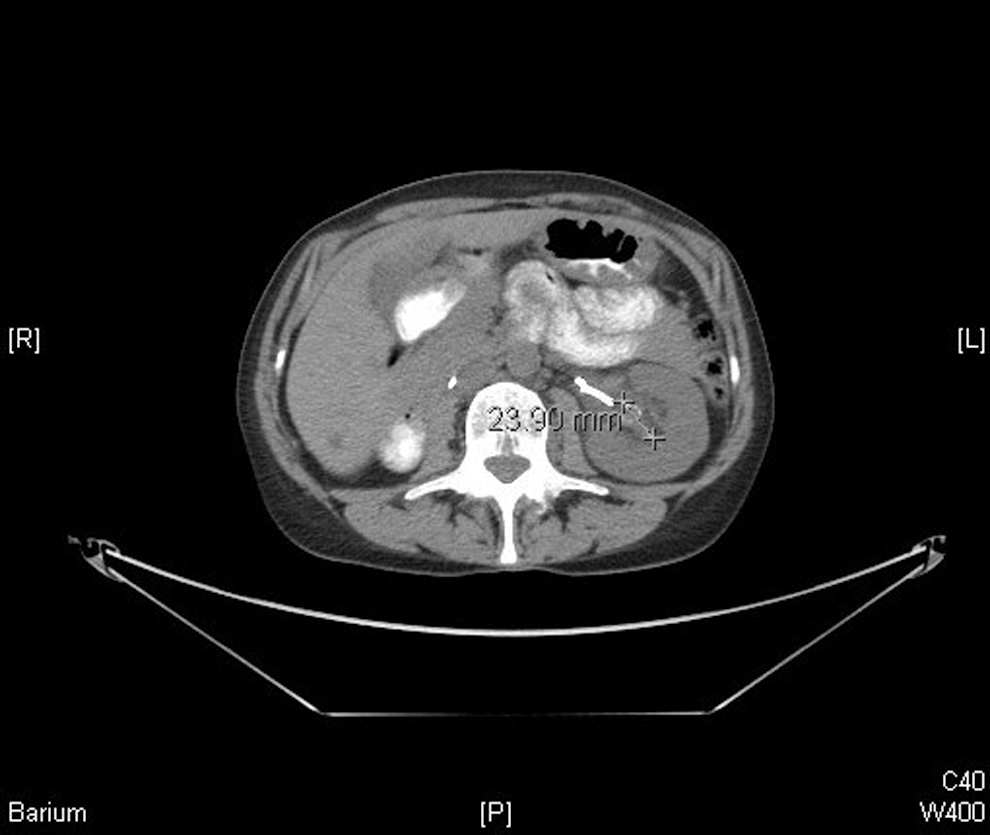
CT scan after five cycles of neoadjuvant chemotherapy, with reduction of left renal pelvis mass to approximately 2.4 cm.
Under general anesthesia in the operating room, with the patient in the prone position, flexible cystoscopy and retrograde access with flexible ureteroscopy was established. Percutaneous access was performed with the ureteroscope in place to facilitate visualization and contrast injection. A 30F renal balloon dilation/access sheath system was placed and a 25F resectoscope was used to resect the tumor under sterile water irrigation. Deep mucosal biopsies were obtained using the resectoscope loop, through the renal pelvis mucosa. Hemostasis was ensured using a rollerball electrode and cautery. A “tubeless” approach was used; an indwelling stent was placed, and no nephrostomy was used. The tubeless approach was selected after resection revealed no evidence of residual tumor throughout the kidney, in an effort to decrease the potential for tract seeding through decreased leakage of urine from the nephrostomy site afforded by this technique.
The procedure was completed in 80 minutes, with an estimated blood loss of 200 mL. The patient's hospital stay was 23 hours without any postoperative complications. Pathologic evaluation demonstrated high-grade papillary TCC with areas suspicious for stromal (lamina propria) invasion. A further two cycles of chemotherapy were administered postoperatively.
Interval cystoscopy performed 3 months later revealed no abnormalities. CT scan performed 6 months postpercutaneous resection, however, revealed a possible filling defect in the renal pelvis. Diagnostic ureteroscopy was performed at that time, which revealed no gross abnormalities. Repeated imaging was performed at 8 months postoperatively; MRI revealed a new, enhancing, 1.2 cm nodule located within a dilated left lower pole calix of the kidney (Fig. 3).

MRI with dilated lower pole calix and enhancing soft tissue structure (arrow).
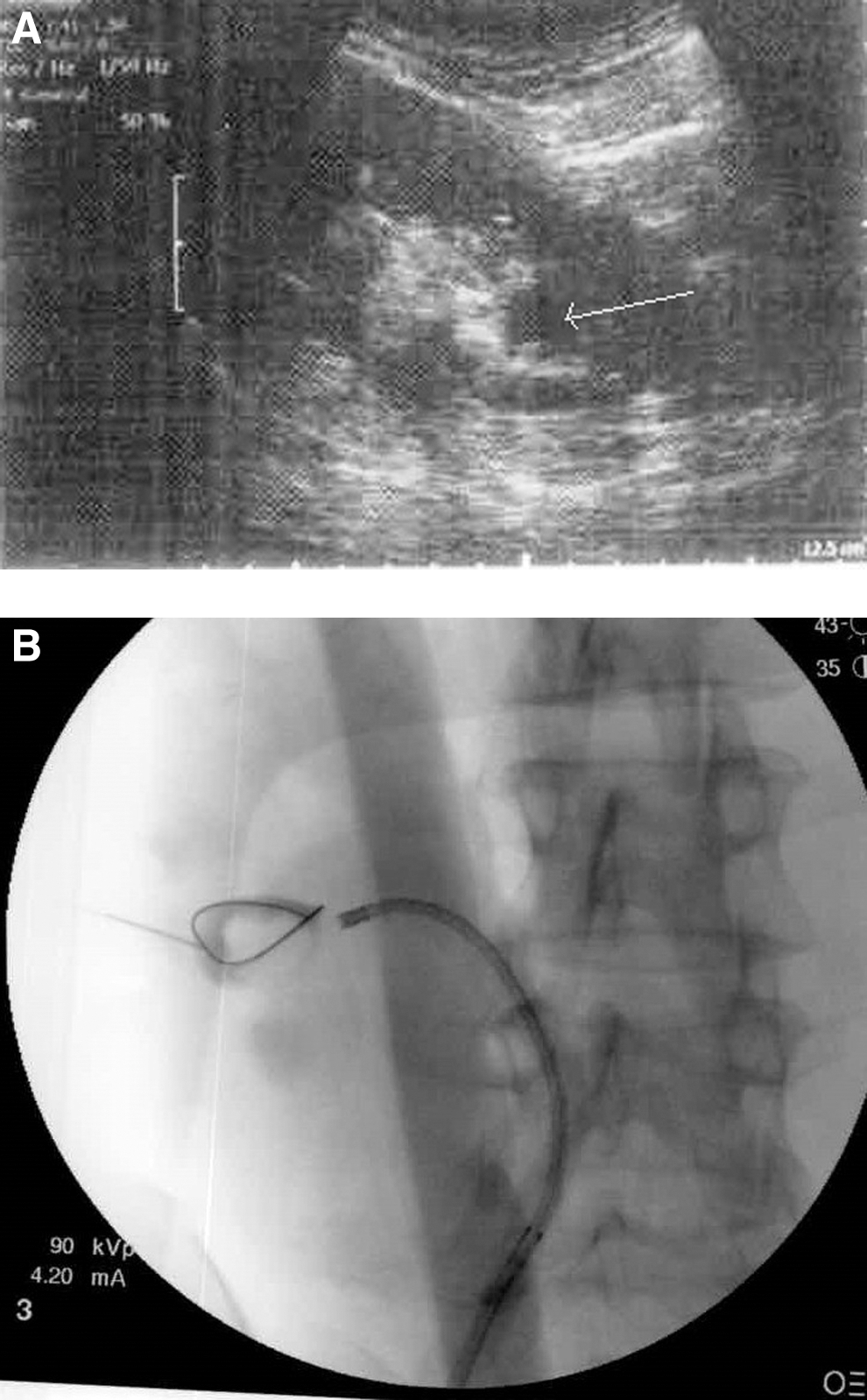
The patient continued to reject nephroureretectomy. She was again brought to the operating room for a repeated percutaneous resection. Here, prone ureteroscopy revealed no obvious urothelial tumors but an excluded calix was noted. With the use of intraoperative ultrasonography, the dilated lower pole calix containing a soft tissue mass within it was identified and punctured percutaneously (Figs. 4A, 4B) The percutaneous tract was then dilated to 30F under fluoroscopy, and using a 25F resectoscope, the papillary tumor was again resected.
Once complete and the base fulgurated, the retrogradely passed ureteroscope was oriented toward the thinnest area of tissue leading to the percutaneous tract. The nephroscope was then used with a forceps to form a new connection to the collecting system using the light from the ureteroscope as a guide. A glidewire was then passed through the ureteroscope through the new opening and into the obstructed calix. Postoperatively, both an internal Double-J stent and a 22F nephrostomy were used, with the nephrostomy placed across the infundibulotomy. Pathologic evaluation of the obtained tissue from the calix revealed fragmented papillary urothelial carcinoma, high-grade, with rare foci of superficial lamina propria invasion.
At both the initial and subsequent resection, consideration was given to the use of topical agents such as bacille Calmette-Guérin (BCG) or mitomycin C. In the absence of carcinoma in situ, however, BCG was thought to be of limited value, and the association of topical mitomycin C with ureteral stricture for a solitary kidney was of enough concern to avoid its use.
Multidisciplinary discussion based on the pathologic findings was held, and the decision was made to avoid additional adjuvant chemotherapy at this time.
After 6 months further evaluation, repeated imaging and interval cystoscopy have produced negative results,and repeated URS is pending.
Discussion
While nephroureterectomy remains the accepted standard of care for patients with TCC of the upper tract, a large experience has been developed for patients in whom renal preservation is desired. Classic indications for such treatment generally prefer low-risk lesions such as small tumor size, low tumor grade, and solitary tumors in patients who understand that a program of aggressive surveillance is needed, and who accept the dual risks of cancer recurrence and progression. 4 We present the challenging case of a patient with an extremely large and high-grade tumor in a solitary kidney, in whom the combination of neoadjuvant chemotherapy and percutaneous resection has resulted in excellent short-term oncologic and functional outcomes.
The treatment of high-grade UTUC in patients with a functionally or anatomically solitary kidney represents a therapeutic dilemma, and complex cases may stretch the limits of endourologic management. Because accurate tumor staging of UTUC is limited by the inability to obtain muscle on specimens, it is generally accepted that tumor grade approximates tumor stage in terms of disease outcomes, and higher grade cancers present a greater likelihood of advanced disease. 5 Ultimate cancer-free survival has been shown to be associated with cancer grade of UTUC by Jarrett and associates, 6 who published a series of percutaneous tumor resection in 30 patients who had mean follow-up of 55 months. They reported a 33% recurrence rate, with dramatic differences seen between grade 1 lesions (18%) and grade 3 cancers (50%). In addition, cancer-related deaths were only observed in patients with high-grade (grade 3) TCC.
Smith and colleagues 7 were the first to present a large series of percutaneous resection of renal pelvis UTUC. Subsequently, other authors have described their experience, 8 but there remain no studies that have compared endoscopic resection with RNU in a prospective, randomized fashion. To date, all published reports are either small series or nonrandomized comparative studies.
Renal preservation in UTUC has been proven to be feasible, but there remain many questions about optimal technique and adjuvant/neoadjuvant treatments (topical and systemic) to be defined. The risk of cancer progression and death of the UTUC patient must be balanced against the morbidities of nephrectomy in a more clearly defined fashion, and, ideally, in prospective fashion. In addition, although nephron-sparing surgery appears to benefit patients in a lower rate of progression of chronic kidney disease than seen with RNU, careful and methodical study needs to be performed. 9
Recurrence of UTUC developed in our patient approximately 8 months after initial resection, and within an excluded calix, likely the result of infundibular stenosis. As our case underscores, excluded calices may be diagnosed when dilation is present and the obstructed calices are absent on retrograde pyelography. 10 Identification and management of such complications must be a part of any treatment plan to assure the potential for complete and accurate future endoscopic surveillance.
A multimodal approach to the management of UTUC with the use of neoadjuvant chemotherapy has been advocated by some as a possible approach to patients with higher risk UTUC. 11 There is, however, relatively little prospective data using this approach in UTUC, although recent data have suggested the efficacy of this multimodality approach in the management of urothelial tumors of the bladder, which may be considered a reasonable surrogate for UTUC. 12 Matin and coworkers 13 recently studied 43 patients who were treated with neoadjuvant chemotherapy for high-grade UTUC and who then proceeded to surgery. The authors reported a statistically significantly lower incidence of invasion on pathologic evaluation in patients receiving neoadjuvant chemotherapy, including a 25.4% lower incidence of pT2 cancers and a 41.5% decrease in pT3 or pT4 cancers. In addition, they reported a 14% incidence of T0 disease in those undergoing neoadjuvant chemotherapy.
In a separate report, Igawa and colleagues 14 described a series of 15 patients with locally advanced UTUC who also underwent neoadjuvant chemotherapy, and they observed similar findings (13% complete response and 53% overall decreased stage) to those seen in the Matin study. The patients in the Igawa series who responded well to neoadjuvant therapy on final pathology results also appeared to have benefits to overall survival. Although prospective and large-scale studies are lacking to suggest such a multimodal approach as the new gold standard, these early series suggest the potential for significant benefits using a neoadjuvant chemotherapy before extirpative surgery for high-risk UTUC.
Extrapolating these pathologic and survival benefits from these series to endoscopic/percutaneous management in the most appropriate patients is certainly not a large leap, although much more study is needed before we are able to derive optimal management in the average situation. Despite this, there seems to be enough encouraging data to suggest a significant disease-specific and survival benefit to warrant exploring this in the appropriately, and carefully, selected patient. To be certain, in our case of a patient with a large, high-grade UTUC in her solitary kidney, who is extremely motivated to avoid RNU and resulting dialysis, we appear to have achieved an initial successful management that has resulted in preservation of the kidney to this point without disease progression.
Conclusion
While percutaneous resection of UTUC is not generally considered the standard of care in the management of UTUC, it appears to a viable strategy even in patients with extremely complex lesions and comorbidities. As this case of “extreme” renal preservation in a highly motivated patient with previous contralateral nephroureterectomy illustrates, neoadjuvant chemotherapy appears to be useful in downsizing an initial tumor, thereby facilitating endoscopic management, just as in neoadjuvant series with RNU.
We believe that such a multimodal approach, using neoadjuvant chemotherapy coupled with nephron-sparing endoscopic management, could represent a reasonable strategy for patients in whom such a therapy is desired. Certainly, further aggressive follow-up in this patient, as well as future studies, will be needed to determine if this is a viable treatment modality.
Footnotes
Disclosure Statement
David M. Hoenig is a consultant, researcher for Boston Scientific. For the remaining authors, no competing financial interests exist.