
Abstract
Caliceal diverticulum management has been performed using various modalities, including ureteroscopy, percutaneous treatment, and laparoscopy. We present our experience with laparoscopic management of caliceal diverticulum in two patients with large caliceal diverticulum and a history of failed open surgery because of the incorrect diagnosis of a simple renal cyst. In laparoscopy, both patients had an uneventful intraoperative and postoperative course. On follow-up, both of them were symptom free without any evidence of diverticulum in imaging. We reviewed the literature and found that laparoscopic management of caliceal diverticulum has been reported in 37 adult patients other than our cases. We performed a pooling analysis and discussed different aspects of the approach.
Introduction
Indications for therapeutic intervention in involved patients include pain, recurrent urinary tract infection (UTI), hematuria, and pressure effect on the adjacent pyelocaliceal system. 4 Traditional invasive approaches, such as nephrectomy, heminephrectomy, and open marsupialization, are currently substituted by less invasive modalities, including extracorporeal shockwave lithotripsy (SWL), ureteroscopy, percutaneous treatment, and laparoscopy. 1,3 We describe our experience with laparoscopic management of caliceal diverticulum in two patients, review the literature on the subject, and present a pooling analysis of the previously reported patients.
Patients and Methods
Case presentation
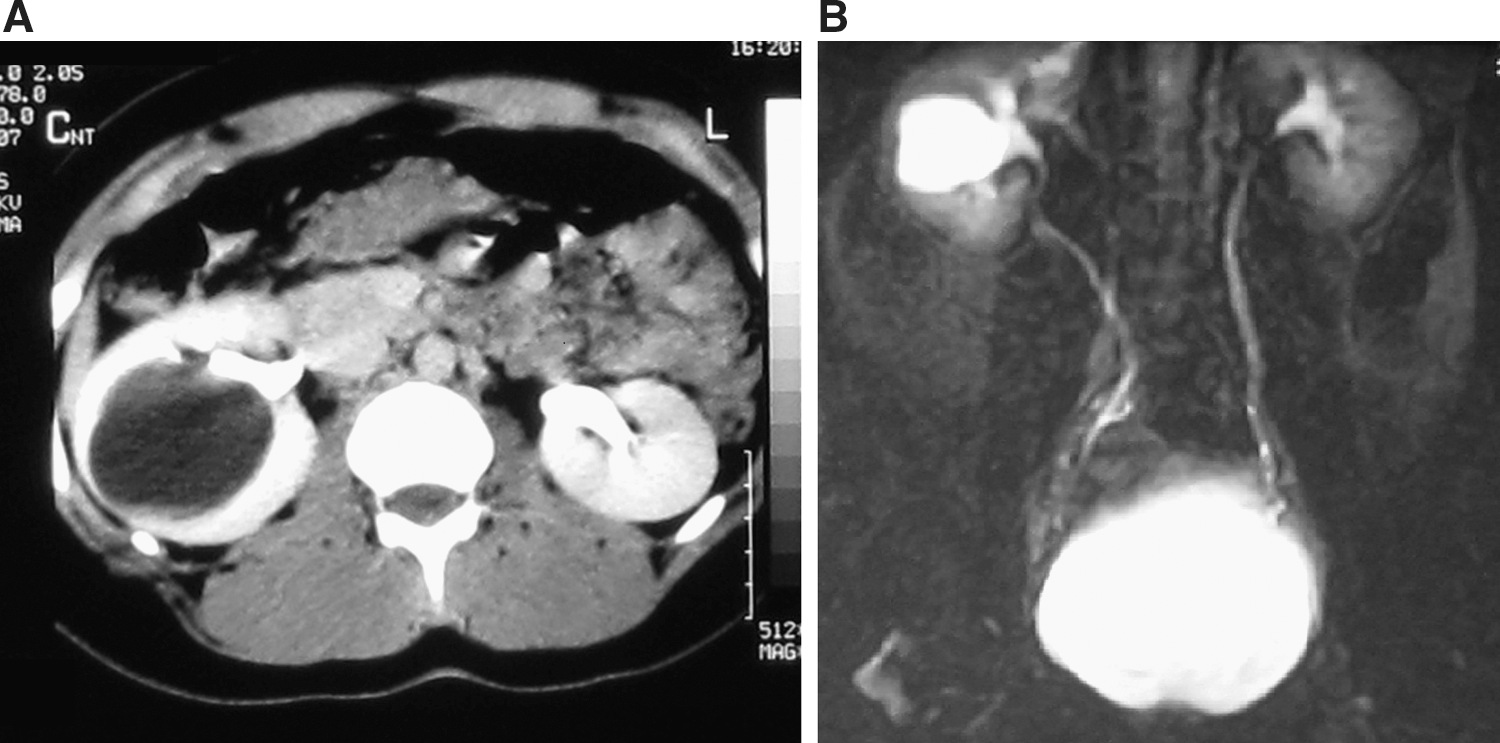
Preoperative imaging of case 1.
On the recent presentation, CT scan revealed a cystic lesion with a smooth wall and a diameter of 10 cm located in the anterior aspect of the upper and midpolar region of the right kidney (Fig. 2). After inserting a percutaneous nephrostomy tube in the cystic lesion, biochemistry of the contained fluid was compatible with urine. An antegrade contrast study revealed the cavity, but the connection between the pyelocaliceal system and the cavity was not seen. Intraoperative retrograde pyelography confirmed the diagnosis of caliceal diverticulum.
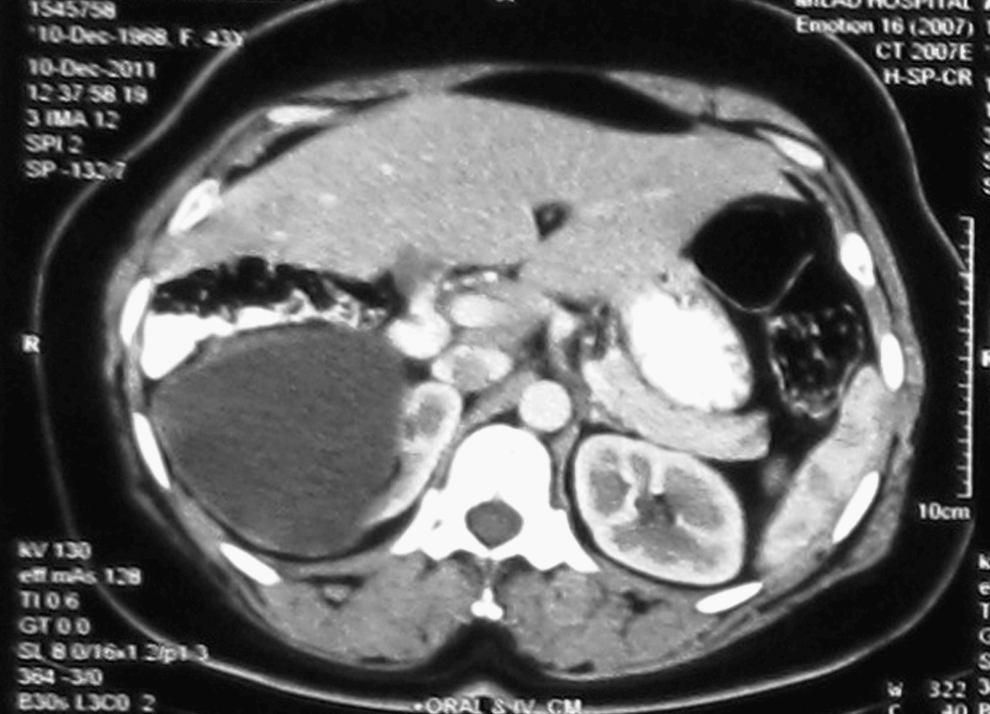
Contrast-enhanced CT in case 2 shows a large cystic cavity in the upper pole of the right kidney causing compression of the renal parenchyma.
Surgical technique
With the patients under general anesthesia, cystoscopy was performed with the patient in the lithotomy position and a 5F ureteral catheter was inserted. Then patients were placed in a 60-degree modified lateral decubitus position, supported by adequate padding. A four-port transperitoneal approach consisting of a 12-mm camera port inserted through an open access approach at the supraumbilical position and one 10-mm and two 5-mm working trocars was used. After medial mobilization of the colon and incising of the Gerota fascia, perinephric fat was removed from the kidney surface.
In the second case, diverticulum location was easily found because of the thinness of the renal parenchyma at the diverticulum location. In the first case, because the diverticulum was endophytic and normal parenchyma had covered it, its location could not be visualized. We used a laparoscopic ultrasound probe intraoperatively, which revealed the sonolucent cavity. The cavity was unroofed and its base was exposed. Then diluted methylene blue was instilled through the ureteral catheter localizing the diverticulum orifice. The orifice was fulgurated by electrocautery, then closed by a figure of eight using 2-0 polyglactin suture.
After confirming closure of the orifice through instillation of methylene blue into the ureteral catheter, the internal wall epithelium of the cavity was fulgurated. The cavity was occluded with a flap of perirenal fat. Finally, the ureteral catheter was removed and a Double-J stent was inserted with the patient in the lithotomy position.
Results
Both patients had an uneventful intraoperative and postoperative course. Operating time was 210 minutes in the first patient and 155 minutes in the second one. There was no significant bleeding. The first patient was followed for 17 months and the second patient for 9 months. Both of them were asymptomatic on follow-up. CT scan showed no evidence of diverticulum 4 months after the operation in the first patient (Fig. 3). In the second patient, postoperative CT obtained 3 months postoperatively showed a cavity measuring 3×4 cm in diameter. Five months after the surgery, ultrasonography (US) revealed a 2×1.5 cm cavity in the upper pole of the right kidney. Finally, US showed no diverticulum and the area was normal 7 months after the surgery.

Postoperative CT in case 1 shows no evidence of diverticulum. The depression in the right renal cortex is the location of the ablated diverticulum.
Discussion
The ideal end result of caliceal diverticulum management is complete obliteration of the diverticulum. Although stone removal and symptom relief are considered in assessment of a therapeutic approach, the remaining cavity may cause stone and symptom recurrence. 5
Because of incomplete stone passage and remained underlying pathology, the SWL success rate in management of diverticulum stone is generally low. 3,6 Best results of SWL are reported for stones less than 15 mm in diameter and diverticula with open neck on imaging studies. A stone-free rate of 58% and symptom-free rate of 86% have been reported in such instances. 7
Ureteroscopic treatment consists of diverticulum neck incision and breaking the stone, and is associated with a 19% to 73% stone-free rate, 35% to 69% symptom-free rate, and 20% obliteration rate. This approach is usually indicated for small stones in upper or midpolar diverticula. 1 Auge and associates 8 reported that the success rate of ureteroscopy is low in lower pole diverticula because of insufficient ureteroscope deflection and failure in localizing the diverticulum orifice.
Percutaneous management of caliceal diverticulum is associated with a high success rate in stone removal, 1 but the diverticulum cavity remains in place in 20% to 40% of patients. Furthermore, need for passing through the whole renal parenchymal thickness in anterior diverticula, tract loss during treatment of small diverticula, and difficulty in obliterating large diverticula are some of the limitations of this technique. 5,9
Laparoscopic management of caliceal diverticulum was first reported by Gluckman and colleagues 2 in 1993. In the past 20 years, 37 adult patients who underwent laparoscopic management of caliceal diverticulum have been reported in English language literature. We discuss the outcome of laparoscopy in previously reported patients along with ours.
There is a general consensus on using laparoscopy for management of anterior thin-walled diverticula. 1,3,4,9 Also, posterior thin-walled diverticula, large diverticula containing large stones, and diverticula with a narrow neck unsuitable for retrograde access are reported to be suitable for laparoscopy. 1,4,10 Some authors believe that deeply located diverticula with a thick overlying parenchyma and a patient history of failed percutaneous treatment are relative contraindications for laparoscopy. 1,3 Thick overlying parenchyma could result in difficulties in intraoperative localization of the lesion, need for limited anatrophic nephrolithotomy, and occasionally pedicle control. It is also associated with higher incidence of bleeding. Hence, endourologic management is preferred in such instances.
In addition to both of our patients who had history of failed open surgery, two previously reported patients had a history of failed percutaneous management. 5,9 Considering the uncomplicated laparoscopic management of these patients, a history of failed percutaneous or open surgery does not seem to be a contraindication for laparoscopy.
Major differential diagnoses of caliceal diverticula are renal cyst and hydrocalix. Misdiagnosis and mismanagement of a diverticulum as a renal cyst may lead to urinary fistula, urinoma, and recurrence of diverticulum. Retrograde pyelography, and delayed intravenous urography (IVU) and CT may be helpful in patients with equivocal findings.
Retroperitoneal and transperitoneal laparoscopy have been applied in 20 and 19 patients, respectively. Retroperitoneal approach advantages include lower incidence of bowel injury, decreased intraperitoneal adhesion, and easier access to posterior diverticula. Easier access to anterior diverticula and having more anatomic landmarks are advantages of the transperitoneal approach. 11
After exposing the kidney in either approach, the diverticulum or its stone should be localized. The first and easiest technique for intraoperative localization of a diverticulum is direct inspection of the kidney surface seeking an elevated, depressed, or lobular area. Retrograde instillation of methylene blue through the ureteral catheter could cause a discoloration visible through the thin overlying parenchyma of the diverticulum. A Chiba or gallbladder needle can be used for percutaneous aspiration of diverticulum content and touching the stone with the needle tip. While Gonzalez and coworkers 9 reported that direct inspection localized the diverticulum in 5 of 7 patients; diverticulum and stone were localized visually in none of the five patients in a report by Miller and colleagues. 3
Fluoroscopy has been used for stone localization in eight patients. Because applying fluoroscopy is difficult with the patient in the flank position, 9 intraoperative laparoscopic US is a better option for localization of the lesion when the overlying parenchyma of the diverticulum is thick and/or the precise location of the diverticulum is not known. US has been used in 10 patients and was successful in all of them. Most of the patients underwent diverticulum marsupialization and fulguration of the diverticulum neck and its internal surface epithelium using argon beam or electrocautery. Retrograde instillation of methylene blue at this step could be helpful in localization of the diverticulum orifice.
In four patients (our two patients and two patients from another report), the diverticulum neck was closed using figure of eight sutures, which resulted in successful obliteration of the diverticulum. 3 Some authors believe that suturing the orifice is difficult and time-consuming 6 ; on the other hand, some believe that fulguration might be sufficient only when the diverticulum has a pinhole orifice, and suturing is generally preferable. 3 Considering successful results of fulguration without suturing, we think that this technique is sufficient in most of the diverticula with a narrow orifice. When a broad neck exists, combining fulguration with suturing might be helpful in complete obliteration of the cavity.
Because the epithelium of a diverticulum is nonsecretory, it is not always necessary to fulgurate the internal surface of the diverticulum, unless the diverticulum orifice is not well localized or hydrocalix is strongly suggested as a differential diagnosis. Wyler and associates 10 described laparoscopic excision of a diverticulum and closing its orifice using Endoloop. They mentioned that total excision of the lesion may prevent recurrence and dissemination of bacterial infection of the diverticulum. Excision is not a good option, however, for deep diverticula and large and inflammatory ones. Furthermore, regarding the high success rate of the marsupialization-fulguration technique, the excision technique has not been vastly used.
Different materials have been used to fill the diverticulum cavity as an adjuvant to the marsupialization-fulguration technique in 23 patients. Surgicel and Floseal have been applied in 7 patients, 9 perirenal fat and the Gerota fascia flap in 12, 3,5,12,13 mesh impregnated with gelatin resorcinol formaldehyde glue in 3, 6 and omentum fixation with stapler in 1 patient. 2 Harrewood and coworkers 5 reported that filling the cavity at the end of procedure seems to be effective, if possible. 5
Wong and associates 14 reported on laparoscopic-assisted transperitoneal percutaneous nephrolithotomy (PCNL) in a patient with an anterior diverticulum containing a stone that also occupied a part of pyelocaliceal system. 14 Clinical application of this technique is limited to patients in whom complex anatomy and stone location do not allow laparoscopy to be used solely.
The average age of 39 reported patients was 45.5 years. Although caliceal diverticulum prevalence in IVU is not different between sexes or sides, 82% of patients managed with laparoscopy were female, and 70% were involved on the right side. Average operative time was 184 minutes (range 80–485 min). Intraoperative and postoperative complications occurred in four (10%) patients, including one patient with bleeding during dissection for finding the diverticulum, leading to transfusion of three packed cell units, 5 prolonged urinary leakage and Double-J stent placement in one patient, 15 prolonged discharge from the trocar site in one case, 5 and subcutaneous emphysema in one. 2 The procedure was completed uneventfully in 90% of patients. Bleeding has been negligible in most of the patients 16,17 ; blood transfusion was needed in only one (2.5%) patient. 5 If the diverticulum is located in a deep position and/or has a thick wall, the incidence of bleeding and transfusion might be increased. Hence, appropriate case selection is crucial in decreasing the incidence of complications.
Laparoscopy has been successful in 87% of patients in relieving symptoms, 92.3% in ablating the cavity, and 100% in stone removal. Laparoscopy has the highest success rate in diverticulum cavity ablation compared with other modalities, such as PCNL, ureteroscopy, and SWL. Some authors consider “the patient's request for the most successful management modality” as an indication for laparoscopy. 9
Another advantage of laparoscopy is the feasibility of simultaneous management of other coincidental renal diseases. In one reported patient, laparoscopic management of diverticulum and its stone and partial nephrectomy for a small renal-cell carcinoma was performed simultaneously. 9
Conclusion
Laparoscopy is the most invasive minimally invasive modality in the management of caliceal diverticulum and its stone. Although some authors believe that laparoscopy should be considered when other approaches have failed, because of its high success and low complication rates, it could be considered as the first option provided the patient is selected carefully. Anterior thin-walled diverticulum is the best candidate for laparoscopy. Large size of the diverticulum and stone and narrowing inaccessibility of the diverticulum neck in retrograde approaches encourage laparoscopy. Small diverticula with a thick overlying parenchyma are not suitable for laparoscopy. A history of failed open or percutaneous management of diverticulum does not seem to be a contraindication for laparoscopy.
Footnotes
Disclosure Statement
No competing financial interests exist.