
Abstract
Background and Purpose:
Laser technology presents a promising alternative to achieve tumor excision and renal hemostasis with or without hilar occlusion, yet its use in partial nephrectomy has not been significantly evaluated. We prospectively evaluated the thulium:yttrium-aluminum-garnet laser in laparoscopic partial nephrectomy (LPN) in our institution over a 1-year period.
Patients and Methods:
We used the thulium laser with a wavelength of 2013 nm in the infrared spectrum. Data were recorded prospectively. Tumor size, preoperative aspects and dimensions used for an anatomical classification (PADUA) score, operative time, warm ischemia time (WIT), and perioperative and postoperative morbidity were recorded. Blood loss, preoperative and postoperative creatinine level, and estimated glomerular filtration rate (eGFR) were also collected.
Results:
A total of 15 patients underwent consecutive LPN. The mean tumour diameter was 2.85 (1.5–4). The mean PADUA score was 6.8 (6–9). The mean total operative time was 168 minutes (128–306 min). Mean blood loss was 341 mL (0–800 mL). Date of discharge was 3.2 days postoperatively (2–8 days). The renal vessels were not clamped, resulting in a WIT of 0 minutes in all cases. There was no statistical significant increase in serum creatinine level or decrease in eGFR postoperatively. Histologically, the majority of lesions (13/15 patients) were renal-cell carcinoma stage pT1a. In all cases, base margins had negative results for tumor.
Conclusion:
The 2013-nm thulium laser system offers excellent hemostasis and precise resection capability of the renal cortex during LPN of small partially exophytic renal tumors. Our series showed excellent perioperative functional and pathologic outcomes, including minimal blood loss, zero ischemia, negative tumor margins, and preservation of renal function.
Introduction
The management of localized kidney tumors has changed, resulting in a shift away from radical nephrectomy toward more frequent use of partial nephrectomy (PN). For many patients with small clinical T1 renal tumors (<7 cm) who are candidates for nephron-sparing surgery, PN is now the reference standard treatment. 1
PN provides equivalent oncologic outcomes with superior functional outcomes compared with traditional radical approaches over the short and long term. Several reviews and one prospective randomized study on PNs have proven equivocal oncologic outcomes to those of radical nephrectomy with the advantage of preserving maximal renal function. 2 –4
Contemporary PN techniques, whether open, laparoscopic, or robotic, can necessitate hilar clamping to achieve a dry operative field to allow precise tumor excision and renal reconstruction. This, in turn, imposes an ischemic stress on the kidney, which may compromise functional outcomes. 5 Laparoscopic partial nephrectomy (LPN) is a technically demanding procedure because of difficulties in identifying tumor margins, maintaining adequate hemostasis, and minimizing warm ischemia time (WIT) in the kidney. Control of the renal pedicle is usually needed, and efforts to restrict WIT can be challenging.
Laser technology, such as diode laser and holmium laser, has been trialed in very select series for both open PN and LPN. 6 The newer thulium:yttrium-aluminum-garnet (Th:YAG) laser, which was first introduced into clinical practice in 2005, 7 has a wavelength of 2013 nm in continuous wave mode and offers complete absorption of laser energy in water, providing superior vaporization and hemostatic properties to those of other lasers. 8,9
We prospectively evaluated the feasibility of using the Th:YAG laser in LPN in patients with pT1 renal tumors in a tertiary referral center with a single dedicated laparoscopic surgeon.
Patients and Methods
Fifteen consecutive patients consented to laser LPN over a 1-year period. The 2013-μm Th:YAG laser (Revolix 120 W surgical laser, LISA Laser Products, Katlenburg, Germany) was used between 25 W to 30 W for renal tumor resection. Data were anonymized and collected prospectively. Preoperative workup included full medical history and physical examination and routine laboratory blood tests. Patient demographics, perioperative characteristics, preoperative and postoperative serum creatinine levels and estimated glomerular filtration rate (eGFR) using the Cockroft-Gault criteria were recorded prospectively.
All patients underwent a dedicated abdominal CT scan with 3-mm axial cuts to delineate characteristics of tumor location, depth, and proximity to the collecting system. Tumor complexity was defined as the exophytic extension (percent) of the tumor from the normal renal border seen radiologically in both (mean) coronal and axial planes of CT imaging. The preoperative aspects and dimensions used for anatomical classification (PADUA) score was calculated. 10
The functional outcomes observed by preoperative and postoperative serum creatinine and eGRF results were analyzed statistically using paired t tests, with P<0.05 considered to indicate statistical significance.
Laser LPN technique
As is standard, three ports were inserted transperitoneally around the region of the kidney. A fourth port was occasionally used if retraction of the liver was needed in right upper pole tumors. After adequate mobilization of the colon medially, the proximal ureter was identified and retracted laterally. Cephalad dissection along this plane invariably led to the renal hilum. In the initial cases, the renal vein and artery were dissected and individually isolated and controlled using vessel loops (in case cross clamping was needed during tumor resection) (Fig. 1), whereas later in our series, only the artery was mobilized and controlled. The Gerota fascia was opened and defatted to mobilize the kidney and to expose the exophytic portion of the tumor (Fig. 2). The laser fiber was introduced via one of the laparoscopic ports using a laparoscopic applicator, and the proposed margins of resection were superficially scored with the laser.

Dissection of the renal artery, vein, and ureter.

Laser resection of the renal tumor.
In all cases, a frontal laser fiber was used for vaporesection between 20 W and 25 W. The laser allows both coagulation and vaporization/cutting capabilities, depending on the distance the fiber tip is held from the tissue being resected (5 mm vs 1–2 mm, respectively). After complete resection, the tumor was extracted via the 12-to 15-mm laparoscopic port via an endoscopic specimen bag.
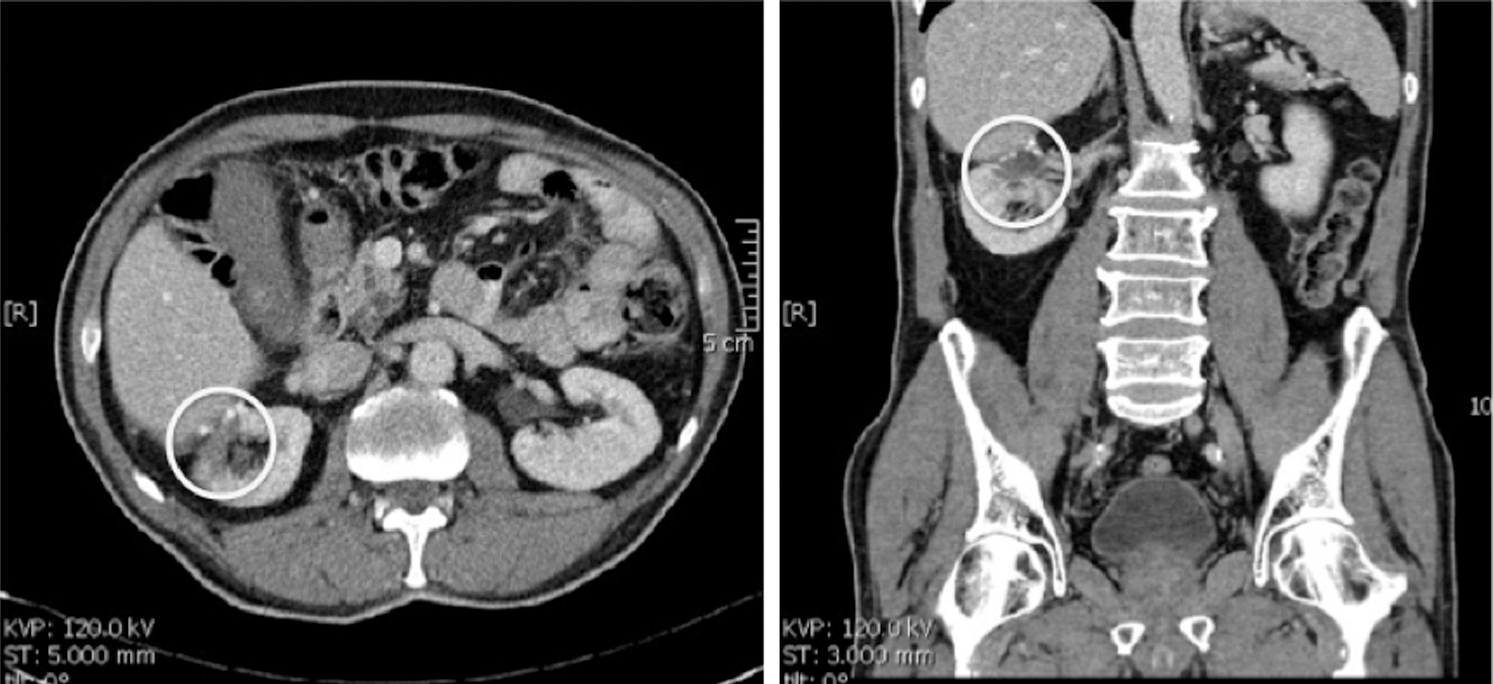
The laser has the ability to seal small vessels between 1.5 and 2.0 mm, providing excellent hemostasis. 7,8 Larger transected vessels from the resection bed were suture repaired. Entry into the collecting system necessitated separate closure using 2-0 polyglactin sutures to ensure a watertight seal. Intraoperative methylene blue was not routinely administered after tumor resection, because most tumors in our series were superficial and only four (26%) cases necessitated collecting system closure. Hemostatic renorrhaphy was performed in using 1-0 polyglactin sutures over prefashioned cellulose bolsters held in place with Hem-o-lok clips. A Robinson drain was placed in all patients. Figures 3 and 4 illustrate representative CT images before and after laser LPN.

Preoperative CT images of renal tumor.
Postoperative CT images after laparoscopic laser resection of renal tumor.
Limitations of the laser
During resection, laser coagulation and vaporization creates a problematic smoke plume that can obscure direct operative vision. This plume increases when the laser is used primarily for coagulation held away from tissue at approximately 5 mm and is less prominent when held 1 to 2 mm away from tissue being vaporesected. The smoke plume is minimized by trickling water down the laparoscopic applicator during laser resection as well as attaching an automatic smoke extractor to one of the port sites.
The laser does not have the ability to seal larger arterial vessels greater than 2.0 mm. Therefore, the potential for bleeding increases with deeper endophytic tumors. One case in our series included a tumor that was 85% endophytic, resulting in a slightly higher blood loss of 800 mL (Table1). Bleeding encountered because of transection of larger vessels necessitates conventional laparoscopic suture repair in the transection bed. Similarly, entry into the collecting system also necessitates separate closure, because such defects are not sealed with laser vaporesection.
Preoperative and Intraoperative Characteristics and Postoperative Renal Functional Outcomes
PADUA=preoperative aspects and dimensions used for an anatomical classification; GFR=glomerular filtration rate.
As with all new technology, there also comes a financial cost that is often significantly higher than the current standards of technique in open PN or LPN, such as resection with cold or monopolar scissors. A standard thulium laser machine by Revolix starts at approximately 45,000 Euros (about $60,056), with each single-use laser fiber costing approximately 450 Euros (about $600).
Results
A total of 15 patients underwent successful LPN using the thulium laser system. Ischemia time was zero in all cases. No patients needed cross-clamping at any time during tumor resection or renal reconstruction. Median tumor size was 2.85 cm (range 1.5–4 cm), Tumor complexity/exophytic percentage of the tumor was 42% (range 15%–70%), the mean PADUA score was 6.8 (6–9), the mean operative time was 168 minutes (range 128–306 min), mean blood loss was 341 mL (range 15–800 mL). Pelvicaliceal entry/repair was performed in four (26.6%) cases. Hemostatic renorrhaphy was performed in 11 (73%) cases. Mean hospital stay was 3.2 days (range 2–8 days). Preoperative and intraoperative characteristics and postoperative renal functional outcomes are summarized in Table 1.
No patients demonstrated any urine leaks postoperatively through the Robinson drainage system. One patient needed a blood transfusion of 2 units of red cells on postoperative day 2 for symptomatic anemia, with a hemoglobin level of 7.8 g/dL. There were no other significant intraoperative or postoperative complications.
All the renal tumors excised were partially exophytic lesions ≤4 cm (pT1a). The final pathologic outcomes are summarized in Table 2. All resections margins had negative results for tumor. The mean preoperative and postoperative serum creatinine levels were 81 mmol/L and 83 mmol/L, respectively. The mean preoperative and postoperative eGFR (mL/min/1.73m2) was 80 and 77.5, respectively. Both properative and postoperative serum creatinine levels (P=0.3485) and eGFR (P=0.3192) were comparable and showed no statistical change.
Pathologic Outcomes
PEC=perivascular epithelioid cell tumor.
Discussion
Duration of warm ischemia is the largest modifiable risk factor during PN in either solitary or two kidney settings. 11 Historically, renal function after laparoscopic or open procedures are equivalent from high-volume laparoscopic centers, with an average WIT of about 30 minutes. Over the last 5 years, however, this figure has been challenged. Recent studies investigating the role of nephron-sparing surgery in tumors within solitary kidneys have highlighted the risk of postoperative acute renal failure and new onset stage IV chronic kidney disease as a result of prolonged warm ischemia and have therefore recommend limiting WIT to 20 minutes or less. 12,13
A variety of methods to reduce this ischemic insult have been described, including surface cooling (ice slush), intra-arterial cooling perfusion techniques, manual compression, early unclamping, and hypotensive anesthesia. 5,14,15 These techniques can be logistically difficult to implement and are often limited to centers with high-volume patient recruitment.
The term “zero ischemia” in PN implies that tumor resection and renorraphy were successfully completed without hilar clamping and not subjecting the resected kidney to ischemic stress. Gill and colleages 5 first described this novel technique in 15 patients undergoing laparoscopic or robot-assisted PN. In their initial published series, they pharmacologically induced hypotensive anesthesia during the excision of the deep part of the tumor. In cases with medially located hilar or polar tumors that were specifically supplied by a dedicated tertiary or quaternary renal artery branch, microdissection and clip ligation of this specific vascular branch was performed. 5
In our series, we did not induce hypotensive anesthesia as described by Gill and associates. 5 Also in our series, only the main hilar vessels were dissected preemptively in the event that en bloc or individual primary renal artery clamping was needed. The vast majority of tumors in our patient cohort, however, were predominately exophytic with likely lower PADUA scores.
Laser technology has recently emerged as a promising alternative to achieve tumor excision and renal hemostasis in a time-sensitive manner without hilar clamping in PN. The use of laser-assisted PN, particularly in minimally invasive approaches, is very limited, however. Early experience with laser technology in renal surgery can be traced back to 1982. 16 As a result of these early pioneering cases, several experimental studies have demonstrated the efficiency of laser-assisted PN in various experimental conditions. To date, however, only small series concerning clinically tested laser-assisted PN have been published, of which only two series were performed laparoscopically (two conventional and one robotic). 6,16,17
The thulium laser emits energy at a wavelength of 2013 nm in a continuous wave fashion. Although it has the same absorption characteristics as a holmium laser in water and tissue, it has superior properties in soft tissue surgery because of the continuous-wave output, resulting in smooth incision and vaporization of tissue with excellent hemostasis. 7 –9
Because of the slightly shorter wavelength compared with the holmium laser, the depth of penetration is decreased to 250 μm. With the thulium laser, the primary chromophore is water; therefore, its mechanism of action is the hot vaporizing quasicontinuous bubbles produced by the laser on contact to near contact. This results in a high-energy density leading to rapid vaporization of water and tissue. 18 Water retains its absorption properties when heated by the laser beam up to the boiling point, which marks the onset of tissue vaporization. Instead of the tearing action on tissue caused by the pulsed emission of the holmium-yttrim-aluminum-garnet laser, the continuous-wave output of the thulium laser allows smooth incision and vaporization of tissue with excellent hemostasis. 19
Thus far, studies evaluating the use of thulium laser in nephron-sparing surgery are sparse. Our study is the largest study to date to use the Th:YAG laser for renal tumor resection in a series of consecutive LPN. Our series of 15 patients shows excellent perioperative functional and pathologic outcomes, including minimal blood loss, zero ischemia, negative results for tumor margins, and preservation of renal function (Tables 1 and 2).
This study has significant limitations. It is a pilot study with small patient numbers (n=15) and no control group. Because laser technology is particularly novel in PN technique, we prospectively trialed thulium laser resection in LPN for small exophytic renal tumors over a 1-year period. The benefits, if any, from using laser vs conventional energy techniques (monopolar cautery or argon beam coagulation) for renal tumor resection have yet to be conclusively determined and need further study. Initial results from our pilot study can be used to design future randomized controlled studies using laser technology, ideally with larger number of patients.
Furthermore, this pilot study was performed in a tertiary referral urologic center by a single experienced laparoscopic urologic surgeon performing more than 50 to 60 upper tract laparoscopic procedures per year. We recognize that laparoscopic PN is technically challenging, and with the introduction of new technology or resection techniques, our results may not be reproducible in institutions that are not high-volume laparoscopic centers.
Conclusions
In this pilot series, the 2013-nm thulium laser system offers excellent hemostasis and precise resection capability of the renal cortex during LPN of small partially exophytic renal tumors. We report zero ischemia and negative results for tumor margins associated with excellent renal functional outcomes in all cases.
Footnotes
Disclosure Statement
No competing financial interests exist.