
Abstract
After robot-assisted laparoscopic prostatectomy, total anatomic reconstruction (TR) with the additions of a circumapical urethral dissection, a dynamic detrusor cuff trigonoplasty, and placement of a suprapubic catheter was performed in 49 patients from June to July 2012. Continence at 6 weeks after catheter removal was assessed for an initial group of 23 patients, and also at 2 weeks in an additional 26 patients who most recently had undergone surgery. Follow-up appointments and telephone interviews were used to assess pad use and continence. Of the initial 23 patients receiving the modified TR, 60.9% had 0 pad use at 6 weeks. By 2 weeks, 65.4% of the most recent 26 patients operated on achieved continence with 0–1 pad use. Preservation and reconstruction of the pelvic floor and supporting bladder structures leads to an earlier return of continence. These key steps need to be validated and confirmed in larger and randomized trials.
Introduction
Methods
Indications and contraindications
Indications for RALP are identical to those for open prostatectomy. RALP can be performed in patients with prostate cancer having clinical stage ≤T2 without clinical or radiographic evidence of metastasis. Patients with severe cardiopulmonary disease unable to tolerate general anesthesia and those with immedicable bleeding diatheses are not candidates for RALP.
Preoperative workup
A complete history and physical examination including a digital rectal examination should be performed. Blood for a serum prostate-specific antigen determination is drawn. If necessary, a biopsy with transrectal ultrasonography is performed. Additional imaging with endorectal MRI may be ordered. The patient should receive medical clearance before surgery.
Preoperative preparation
Patients fast beginning at midnight on the day of surgery. Patients are counseled about the risks of bleeding, infection, general anesthesia, and adjacent organ injury and informed consent is obtained. The possibility of postoperative urinary incontinence and/or impotence should be emphasized. A broad-spectrum antibiotic is administered before incision.
Materials
Instrumentation for RALP includes a combination of conventional and specially designed robotic instruments listed below:
• Versaport Plus bladeless 5–12 mm (Covidien) • Versaport bladeless 5 mm (Covidien) • Endopath dilating tip trocar and housing 10/12 mm dilating tip (Cardinal Health)
• da Vinci robotic 0-degree and 30–degree scopes • Csrp robotic lapsky tray • New robotic fourth arm prostatectomy • New robotic fourth arm accessories • K. Storz robotic urology instrument tray robksuro 008
• Hydroline trumpet valve with pulsewave cassette (Cardinal Health) • Weck Hem-o-lok clips (Teleflex Medical) • Endoscopic needles – Polysorb (Covidien) • Biosyn sutures (Cardinal Health) • Endo Catch Gold (10 mm) (Covidien) • Endo Shears (5 mm) (Covidien) • V-Loc 26-mm sutures (Covidien) • Chromic Gut V-20 (26 mm) (Covidien) • Sofsilk cutting 26 mm (Covidien) • Maxon sutures 40 mm (Covidien)
Background
The numerous potential causes of post-RALP incontinence are related to disruption of normal anatomic contributors to continence (Table 1). These include shortening and thinning of the membranous urethra, devascularization or partial sphincter excision, bladder hypermobility and pelvic floor descent, posterior support disruption, and nervous tissue injury.
The TR after RALP has been developed to correct these possible causes of prolonged postoperative incontinence. The pillars of the technique are minimal periprostatic dissection and anatomic reconstruction. We have arrived at the present version of the technique only after trial and analysis of functional outcomes in several thousand patients. Tan and associates 4 described the early evolution of our technique to hasten early continence using vesicourethral conventional anastomosis to anterior reconstruction only to the TR.
In our modified TR, shortening and thinning of the membranous urethra and devascularization or partial excision of the sphincter is overcome by approaching the membranous urethral dissection circumapically. 5 Improved visualization of the junction between the prostate and membranous urethra permits the prostate to be swept and retracted superiorly. This maneuver allows for maximal preservation of membranous urethral length, providing added security during stress.
Normally, the puboperinealis muscle forms a dynamic cuff that pinches and angulates the urethra. This cuff is often disrupted during posterior apical dissection, which weakens this support. The second addition to our new technique involves performing a dynamic detrusor cuff trigonoplasty, which supports the proximal urethra and bladder neck with contractile detrusor tissue and constricts this outlet. 6 Reconstruction of this dynamic cuff is thought to be very important in the restoration of continence.
Another possible cause of incontinence is the disruption of the anterior fixation of the bladder. This causes the bladder to collapse into the pelvis, resulting in a loss of the normal angulation of the vesicourethral junction. In addition, when the bladder is mobilized and incisions are made through the arcus tendineus and puboprostatic ligaments, the urethra becomes hypermobile and the pelvic floor descends. These mechanisms of incontinence can be avoided by placement of a suprapubic catheter and elevating the bladder, limiting urethral hypermobility and pelvic floor descent while restoring the normal angulation of the vesicoprostatic junction. 7
Before our modifications to TR, several techniques had been attempted to improve early continence. Kalisvaart and colleagues 8 reported achieving a rate of 90.9% of patients using under 1 pad and 48.2% were pad free at 3 months after RALP, using the posterior reconstruction and anterior suspension with a single anastomotic suture. Rocco and coworkers 9 published a method in which, before vesicourethral reanastomosis, the posterior rhabdosphincter is joined with remnants of Denonvilliers fascia, and then attached to the bladder wall. Not all studies agree that anatomic reconstruction improves continence after RALP. Menon and colleagues 10 compared a group whose members underwent periprostatic reconstruction with a group whose members did not. No difference in continence rates was found.
The purpose of our study was to determine if TR with three additional surgical techniques, including using a circumapical approach for urethral dissection, performing a dynamic detrusor cuff trigonoplasty, and the placement of a suprapubic catheter as described above could further improve continence rates after RALP. Our additions to the TR technique are aimed at the possibility of achieving an even earlier return to continence (<6 weeks) with the potential for immediate continence. These modifications synergistically work to address possible causes of incontinence not previously accounted for by other techniques.
Our technique is founded on a simple assumption: Anatomic normalcy correlates with functional normalcy. We attempt to reconstruct the pelvic anatomy after RALP with the goal of improved functional status postoperatively, specifically earlier continence.
Surgical Technique
Dropping the bladder
The peritoneum is incised widely. The inverted U-shaped incision begins lateral to the left medial umbilical ligament and is extended high across the midline to the right umbilical ligament. The ends are extended to the level of the vas deferens. The medial umbilical ligaments and the urachus are cut using a monopolar electrocautery shears. We next develop the space of Retzius and expose the bladder, prostate, and puboprostatic ligaments.
We identify the endopelvic fascia and dissect the periprostatic space athermally, keeping the plane of dissection between the endopelvic fascia and lateral prostatic fascia. During development of the retropubic space and incision of the endopelvic fascia, we proceed distally and medially. Meticulous dissection is performed to minimize disruption of the puboprostatic ligaments and arcus tendineus until the urethra is exposed and there is a clear space for the placement of the dorsal venous stitch. The arcus tendineus and puboprostatic ligaments are used later in the anterior reconstruction.
Dissection of the bladder neck
Identification of the bladder neck is facilitated by defatting the prostate anteriorly and using a technique termed the “bimanual bladder neck pinch” as we have previously described. 11 Using blunt robotic instruments, the prostate is trapped, and instruments are pulled proximally until there is a sudden feeling of “giving way” at its junction with the collapsed bladder.
The surface is scored to precisely mark the prostatovesical junction anteriorly. The bladder neck is incised in the midline using Maryland bipolar forceps and hot shears with 1:1 scaling for adequate coagulation of any bleeders. Dissection proceeds until we identify the Foley catheter tip, lifting it upward using the free robotic arm, providing a source of countertraction. The dissection proceeds laterally. Care is taken to maintain the appropriate plane of dissection.
We define the posterior junction intravesically, scoring the bladder mucosa. After dissection through the mucosa, we identify the retrotrigonal fibromuscular layer as we have previously described. 12 This is the fascial plane beyond which electrocautery is no longer used to avoid damaging the neurovascular bundles and pelvic plexus, which are in close proximity to the bladder. Dissection proceeds in an athermal, traction-free manner, preserving the neural hammock surrounding the prostate and the trigonal nerves until the shiny surface of the vas deferens is seen.
Athermal dissection of the vas deferens and seminal vesicles
The vas deferens are picked up one at a time and dissected out using athermal technique, clipping the ends and cutting them. The cut ends are then lifted up by the fourth arm of the robot.
We develop a plane between the seminal vesicles and the surrounding fascia and identify the arteries entering into the seminal vesicles. These are cut using clips and sharp dissection. Lateral to the seminal vesicles, it is important to be aware of the proximity to the neurovascular bundles. Every attempt is made to preserve them. Both the seminal vesicles and vas deferens are then pulled upward. In patients who are appropriate candidates for nerve sparing, an intracompartmental seminal vesicle dissection is performed as in our traction free article. 13
Nerve sparing
The optimal approach to prostatic dissection is based on the appropriateness of the cancer control and grade of nerve sparing. Our dissection proceeds in a plane according to the risk grade as determined by our previously published protocol. 14 We develop this plane athermally by sharp and blunt dissection, proceeding distally toward the apex and laterally on both sides.
At the lateral attachments, the perforating arteries are entering into the prostatic capsule. We sharply cut them and develop a plane between the capsule and the medial aspect of the pedicular vessels. They are sharply cut after being secured by clips.
Circumapical urethral dissection
Once the prostate is reasonably mobilized, we lift it upward and develop a plane along its posterior surface (Fig. 1). The remaining pedicular vessels are then identified, clipped, and cut. The plane then separates easily, and dissection is continued distally around the prostate, specifically near the apex at the posterolateral aspect. The prostate is retracted to one side and anterolateral dissection is performed with the goal of preserving the urethral sphincter. This is repeated on the contralateral side. Finally, the prostate is released posteriorly and laterally.
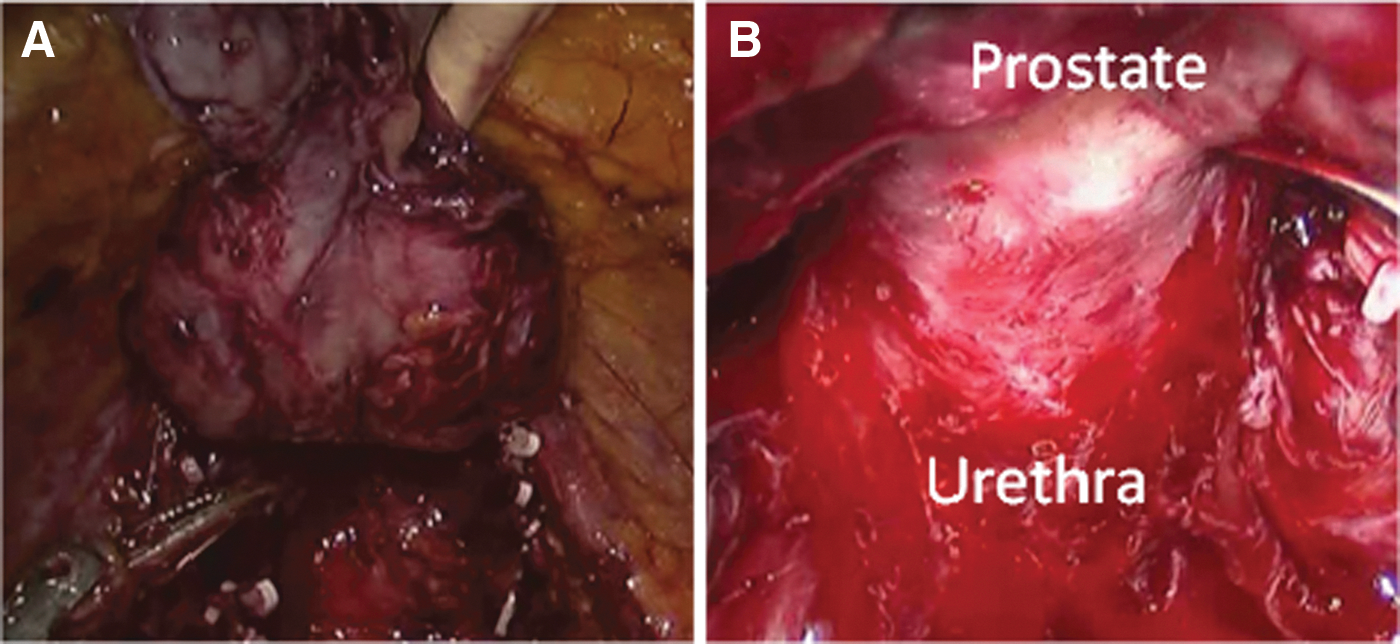
Circumapical dissection.
We lift the prostate and find the distinct plane between the prostatic apex and the urethra using blunt dissection. Sweeping the apex away from the urethra, we gain 1 to 2 mm of ventral membranous urethral length before transection. 5 Once transection is complete, we move onto the anterior surface of the prostate. At this time, the prostate is only loosely attached by some veins, ligaments, and fibrofatty tissue because the urethra has been cut posteriorly.
After securing the prostate with suture, we then use both blunt and sharp dissection to find the distinct plane between the anterior prostatic apex and the membranous urethra. Again, with blunt dissection, we save an additional 1 to 2 mm of urethral length anteriorly.
Effort is made to avoid skeletonizing the urethra distally. To this end, the least amount of dissection possible is performed. Under direct vision, the anterior urethra is cut sharply and the prostate is now free. It is then bagged along with the ymph nodes, and we prepare for the reconstructive aspect of the surgery.
Dynamic detrusor cuff trigonoplasty
The anterior bladder is held using the fourth arm of the robot, and we identify the bladder opening, mucosa, and ureteral orifices (Fig. 2). The posterior extent of this bladder opening is closed with a “tennis racquet” stitch using mucosa and detrusor fibers and 4-0 Biosin suture. The opening is now just large enough to accommodate a 20F Foley catheter. The mucosa is then everted using the same suture.
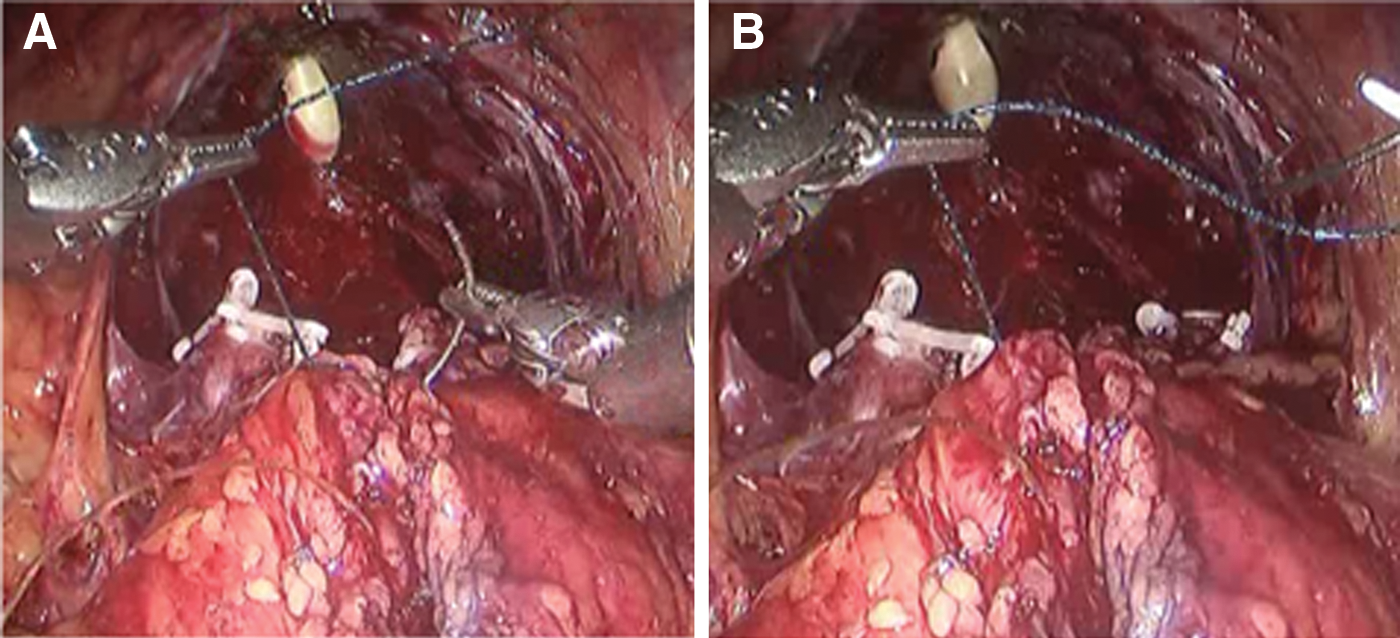
Dynamic detrusor cuff trigonoplasty.
The posterior gap behind the newly constructed bladder neck is covered using a flap of detrusor muscles and approximated in the midline using a 3-0 V-Loc suture completing the dynamic detrusor cuff trigonoplasty, supporting the bladder neck. 4 This posterior reinforcement is based on the principles of Pagano and colleagues. 15
Posterior reconstruction
During circumapical dissection, suture was passed into the posterior aspect of Denonviliers fascia. Shallow, superficial bites are emphasized so that the underlying nervous tissue remains intact. The same suture is passed through the retrotrigonal layer and cinched down.
Anastomosis and anterior repair
We then use a V-loc suture described in our previous article as a self-cinching technique; we complete the anastomosis in two layers. 16 The two-layer anastomosis is finished, and mucosa to mucosa approximation is achieved. Key elements of a secure, watertight anastomosis are: Proper mucosal apposition, tension-free approximation, and avoidance of the neurovascular bundles.
Using a single-knotted suture, small bites of the previously preserved arcus tendineus are sutured to partial thickness bites of the detrusor muscle. This is termed anterior reconstruction 17 and aids to position and stabilize the vesicourethral junction.
Suprapubic catheter placement
The bladder is filled with 180 mL of water, and the suprapubic catheter is introduced into the bladder (Fig. 3). 7 This aids in elevating the bladder to its normal preoperative position in which it was attached to the anterior abdominal wall.
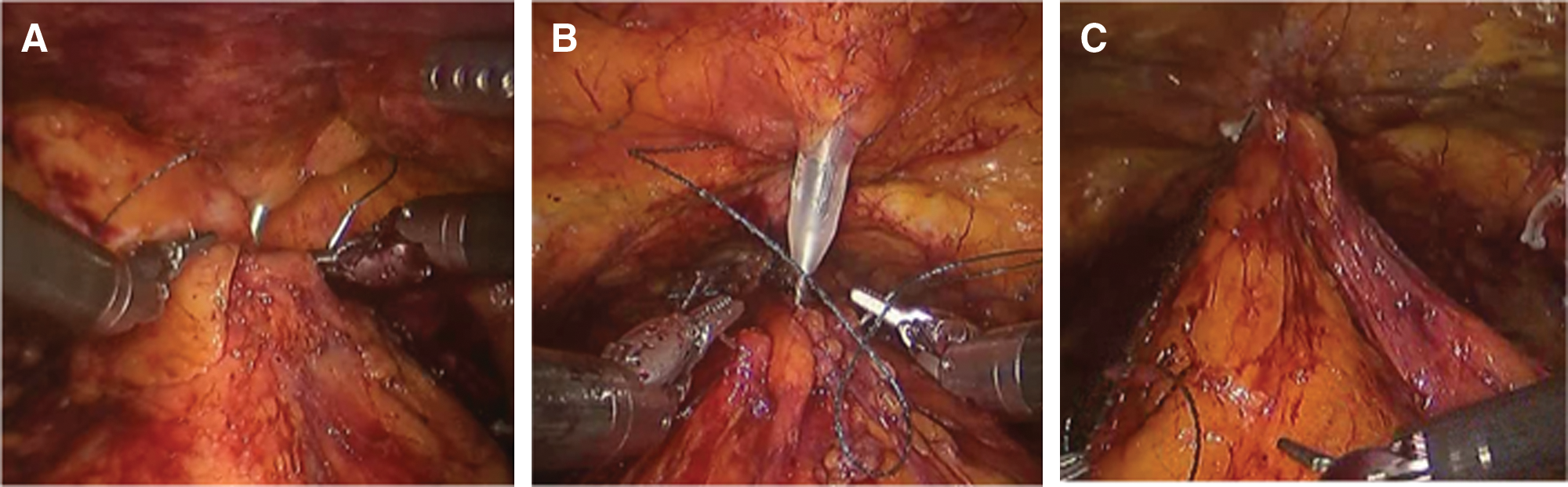
It also serves as a route for urinary diversion in cases in which we do not use a catheter and instead are using a splint. Finally, we reperitonize the flap of the peritoneum so that the anatomy is restored to its preoperative state.
Postoperative care
The patient is left with a suprapubic catheter, bulb drain, and occasionally a Foley catheter. On postoperative day #1, pain is managed with parenteral narcotics. Sequential compression devices and early ambulation are used to prevent deep venous thrombosis (DVT). The patient is started on a clear liquid diet, which is advanced as tolerated. Once the patient has been taught catheter care, is ambulatory, and tolerating oral pain medication, he is discharged. One week after surgery, the patient returns for catheter removal and discussion of the pathology report. Patients then begin Kegel exercises.
Possible complications
Argawal and associates reported an overall complication rate of 9.8% in 3317 patients undergoing RALP with 81.3% of these occurring within 30 days. 18 During the operative and immediate postoperative period, anemia necessitating transfusion, xerophthalmia, anastomotic urine leak, and ileus were the most often observed, together occurring in 3.6% of all patients. The most common delayed complications were lymphocele and bladder neck contracture, 0.8% and 0.7% of all patients, respectively. Postoperative bleeding necessitating reoperation during the initial hospitalization was seen in 0.3% of patients. Bowel injury and port site hernia have been reported to have an incidence of <1%. DVT/pulmonary embolism occurred in seven (0.2%) patients, and one patient experienced myocardial infarction.
Results
Recently, Srivastava and coworkers 19 evaluated the effect of a risk-stratified grade of nerve-sparing technique on the early return of urinary continence. In that series of 1417 men, 55.8% achieved early continence defined as the use of 0 pads in 24 hours at 12 weeks postoperatively. They also found a correlation between the risk-stratified grade of the nerve-sparing technique and early return of urinary continence.
Our preliminary results show that the continence rate at 6 weeks is improved TR with the three additional techniques described. In our series, among the initial 23 patients, 60.9% of patients achieved continence defined as the use of 0 pads at 6 weeks (Table 2, Fig. 4). This technique was performed in another cohort of 26 patients more recently operated on, of whom 65.4% were continent with 0 to 1 pad use at 2 weeks.
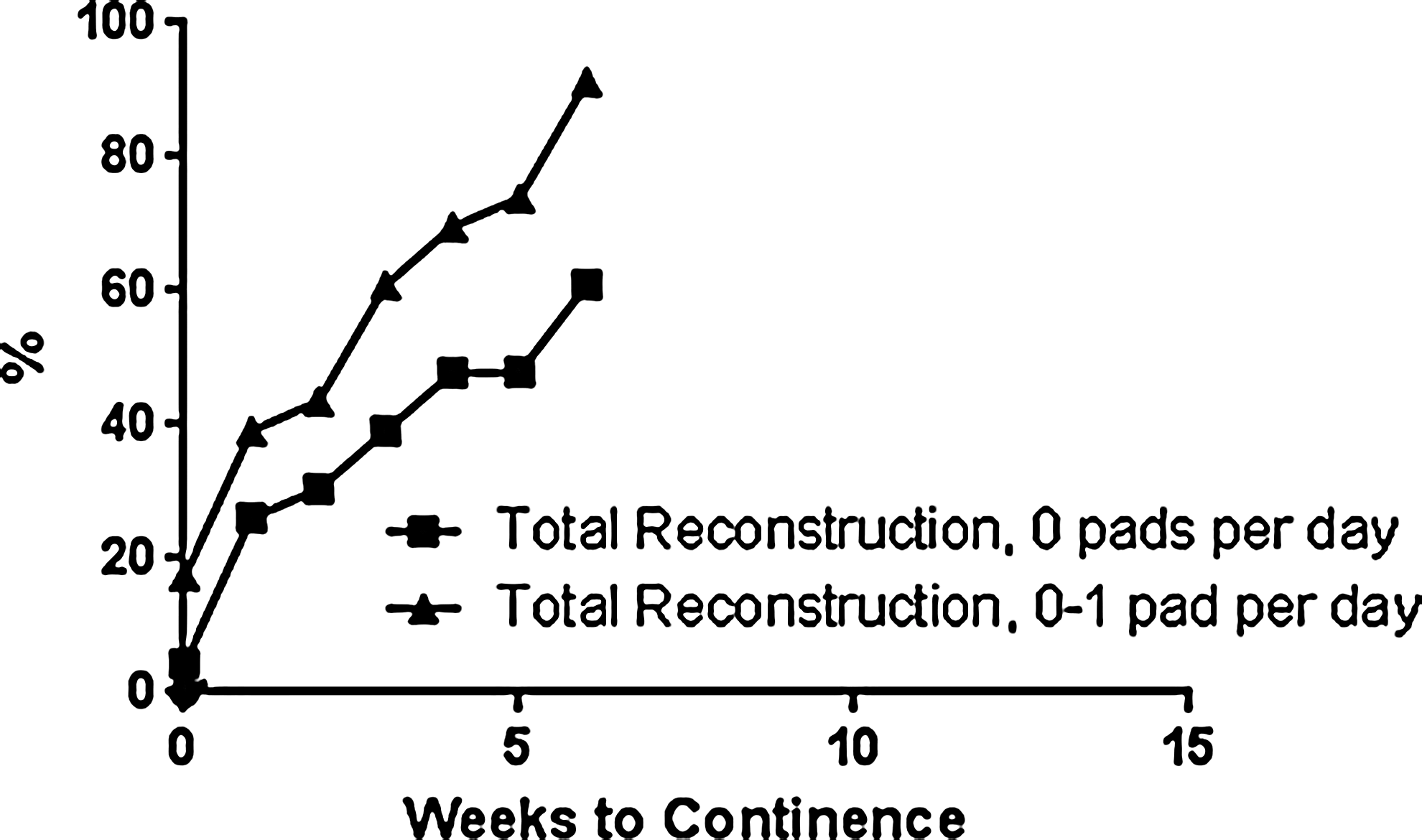
Percentage of patients achieving continence at 6 weeks using the modified total anatomical reconstruction technique after RALP. Percentage continent with 0 pad use shown, as well as 0-1 pad use.
Discussion
Much progress has been achieved in clarifying the anatomic, physiologic, and neural basis of the male continence mechanism, resulting in novel adaptations of conventional radical prostatectomy with the aim of preserving continence and accelerating its return.
To this end, we make painstaking efforts to reconstruct even small pelvic structures and reposition the urinary bladder to its normal position. With our approach, we are finding that the degree and duration of incontinence is reducing even after performing close to 5000 RALPs. We have also noted that apical dissection is of the utmost importance and the degree of nerve sparing intraoperatively may impact continence.
Our modified technique is not predicated on one magical step or suture that alleviates the problem of incontinence. Rather, we have found that multiple small, intraoperative steps in sequence are needed to maintain the delicate balance of voiding and continence that exists before removal of the prostate. As has been shown by our experience over the years, RALP is an ever-progressing and dynamic surgery on which improved outcomes beget improved outcomes.
Conclusion
Our initial results suggest that our modified TR technique not only hastens continence, but also that a significant level can be achieved within 2 weeks. These results are preliminary, and the effectiveness of these key steps we have discussed need to be validated in larger studies.
Footnotes
Disclosure Statement
Dr. Ashutosh K. Tewari discloses that he is the principal investigator on research grants from Intuitive Surgical, Inc. (Sunnyvale, California, USA) and Boston Scientific Corporation; he is a non-compensated director of Prostate Cancer Institue (Pune, India) and Global Prostate Cancer Research Foundation; he has received research funding from The LeFrak Family Foundation, Mr. and Mrs. Paul Kanavos, Craig Effron & Company, Charles Evans Foundation and Christian and Heidi Lange Family Foundation. No competing financial interests exist for the remaining authors.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.