
Abstract
Purpose:
We present our experience with the use of metallic stents (Wallstents®) in the management of malignant ureteral obstruction to maintain renal function, thereby permitting the use of chemotherapeutic agents to treat the underlying malignancy.
Patients and Methods:
We retrospectively reviewed the records of 24 patients with ureteral obstruction secondary to advanced cervical carcinoma, stage T3b (n=10) and T4 (n=14), that was relieved by Wallstents. Nineteen patients needed bilateral and 5 needed unilateral Wallstents to relieve the obstruction. Fifty-six additional endourologic interventions were necessary to assure continued patency. Holmium laser ablation was used 14 times to manage tumor proliferation and ingrowth at the distal end of the stent. Thirty-two endostents, 4 extension, and 6 replacement stents were used to maintain patency of the ureter.
Results:
Nineteen of our 24 patients received between one and five chemotherapeutic cycles over 18 to 140 months. In five patients, placement of Wallstents did not achieve adequate decrease of the creatinine levels to allow treatment with chemotherapy. Thirteen of 24 Wallstents remained patent over 18 months, yielding a primary patency rate of 54%. Technical success rate of Wallstent placement was 100%. The overall mean primary and secondary patency rates of the stent were 16.5 and 52 months, respectively. For T3b and T4 patients, the mean primary patency rates were 20.6 and 13.6 months, respectively. Secondary patency for T3b patients was 73.9 months vs 36.4 months for T4 patients. There were no serious complications associated with Wallstent placement.
Conclusion:
Wallstents offer a salutary solution to the problem of maintaining prolonged patency of ureters compromised by encasing neoplasms.
Introduction
Metallic stents were introduced some 25 years ago, lauded for a better rate of patency and fewer side effects. 6 –8 The recent literature indicates a resurgence of interest in this technique, emphasizing their advantage over polymeric stents with respect to relief of obstruction, increased interval between changes, reduced irritating symptoms, and lower maintenance cost. 2,9 –16 The utility of relieving ureteral obstruction in patients with advanced cervical cancer cannot be overstated: The literature suggests that patients who receive platinum-based chemotherapy may experience a 15% absolute increase in 5-year survival vs patients who did not receive chemotherapy. 17
We present results of 24 patients with cervical cancer, stages T3b and T4, who were followed over a 12-year period and treated with metallic Wallstents® (Boston Scientific) to relieve urinary obstruction and preserve renal function, thereby allowing repeated cycles of chemotherapy. Impact of the metallic Wallstents on survival and, in particular, renal function status (creatinine and clearance) was assessed. The importance of salvage procedures such as endostent placement and holmium laser ablation for secondary patency is also discussed.
Patients and Methods
Between March 1995 and February 2000, 24 patients, age 34 to 73 years (mean 51 years) with malignant ureteral obstruction secondary to cervical carcinoma, stages T3b (n=10) and T4 (n=14), underwent percutaneous placement of Wallstents with an experienced uroradiologist to relieve the obstruction and safeguard renal function. The cause of obstruction was established on contrast-enhanced triple phase CT in all patients. The length and morphology of the compromised ureter was defined on antegrade pyelograms. A histopathologic diagnosis of cervical cancer was established by biopsy in all patients. The indication for placing metallic Wallstents was deterioration of renal function, which was indicated by rising creatinine values and decreasing clearance, which ultimately prevented the use of chemotherapy to treat the underlying malignancy. The decision to use metallic Wallstents as opposed to polymeric Double-J stents was based on our poor results with 17 previously placed polymeric Double-J stents: Of those, 2 had migrated distally into the bladder, 1 obstructed during active bleeding, 1 obstructed with resulting pyelonephritis, and 13 occluded because of compression and/or encrustation within 2 months. All 17 polymeric stents needed replacement. Informed consent for the procedure was obtained from all patients.
Technique
Antibiotic prophylaxis was administered 24 hours before the procedure, which was performed under conscious sedation. Antegrade placement of the metallic Wallstents was preferred for convenience and cost reasons. Primarily, antegrade access had already been established to assess the length and configuration of the diseased areas of the ureter; the retrograde approach, in our experience, was specifically insufficient in visualizing the proximal end of the stricture. Retrograde placement of an ureteral Double-J stent placement had also failed in the patients.
The patient was placed in an oblique supine position. Under local anesthesia, a 22-gauge Chiba needle was advanced using fluoroscopic and/or ultrasonographic guidance along the Brodell avascular zone into the posterior mid or superior calix. An 0.017-inch hydrophilic guide wire (Cook, Bloomington, IN) was then advanced into the pelvis and upper ureter. The tract was then dilated with a 4F catheter, and antegrade ureterography was performed to define the length and morphology of the ureteral stricture. Finally, an 0.035 Amplatz wire (Cook, Bloomington, IN) was advanced across the stricture into the bladder. Two 4, 6, and 8 mm high pressure balloon catheters of appropriate length (Olbert Bard Urologic) were sequentially advanced through the stricture, which was dilated with pressures ranging from 6 to 14 atm. Once the stricture had yielded, a Wallstent of 8 to 10 cm in length and 6 to 10 mm in diameter was placed, extending 0.5 cm beyond the ureteral orifice into the bladder and 3 cm proximal to the stricture at its rostral end. If this could not be achieved with one Wallstent, overlapping stents were deployed. To secure the stent in position, its vesical and rostral ends were flared by overdistending the balloon to 12 to 14 mm under pressures up to 25 atm. This technique was an off-label use of the Wallstent, yet resulted in a solid stent seating and prevented migration.
In 19 patients, both ureters had stent placement; in 5 patients, only one ureter received a stent, because there was no function in the other kidney on a radionuclide study. Four Wallstents were deployed via a retrograde cystoscopic approach by urologists, and the remaining 20 Wallstents via an antegrade percutaneous approach by an experienced interventional radiologist. As mentioned earlier, the antegrade approach was favored because access had already been established to assess length and configuration of the stricture. Furthermore, previous cystoscopic placement of Double-J stents had failed in a number of these patients.
A percutaneous nephrostomy was kept in place for 48 hours, but capped. Once satisfactory urine flow was established and a normal urinalysis was confirmed, the percutaneous nephrostomy was discontinued. If there was evidence of a urinary tract infection, the nephrostomy tube was left in place for an additional 1 to 2 weeks until antibiotic therapy cleared the infection.
Adequate urine output, decrease of hydronephrosis, if present, and improvement or normalization of creatinine values and clearance were indicators of clinical success. Follow-up relied primarily on serum creatinine levels, which were obtained every other week for 3 months and thereafter in monthly intervals. Elevation of creatinine prompted reexamination by ureterography and cystoscopy to identify and define any cause of recurrent obstruction.
Primary patency was defined as successful restitution of urine flow after placement of the Wallstent. Secondary patency was defined as successful restitution of urinary flow after supplementary treatment with endostents, extension stents, or ablative procedures to remove obstructive tumor-elements.
Results
The principal aim of metallic stents, preservation of renal function to permit continued treatment with chemotherapeutic agents, was met. Nineteen of our 24 patients received between 1 and 5 chemotherapeutic cycles over 18 to 140 months. In five patients, placement of Wallstents did not achieve adequate decrease of the creatinine levels to allow treatment with chemotherapy. Thirteen of 24 Wallstents remained patent over 18 months, yielding a primary patency rate of 54%.
To preserve patency and thus renal function, 56 additional endourologic interventions became necessary. These salvage procedures were undertaken whenever creatinine rose to a level making chemotherapy hazardous. Careful monitoring of renal function parameters allowed for timely corrective interventions, precluding significant loss of renal function. Fourteen Holmium laser ablations were performed to clear the intravesical end of the stent of hyperplastic reaction or tumor proliferation (n=10) and of tumor ingrowth through uncovered stents (n=4). In addition, 32 endostents, 4 extension stents and 6 replacement stents had to be placed to maintain acceptable urine flow. The Double-J polymeric endostents were primarily deployed to counter compression of the Wallstent (n=28) and to correct occlusion at the intravesical end by tumor ingrowth (Fig. 1). In four patients, cephalad tumor extension and compromise of the ureter was alleviated by an extension Wallstent overlapping the original stent, which was introduced via an antegrade approach (Fig. 2). In three patients, new Wallstents were introduced cystoscopically in a retrograde fashion to replace Wallstents that had migrated into the bladder, which was thought to be from secondary radiation emanating from the stent when irradiated by high voltage external beam therapy, thereby loosening the stents. Kinking of the stent secondary to encrustation called for replacement of the Wallstents in three other patients, whereas 22 Double-J polymeric stents showed evidence of encrustation on removal.
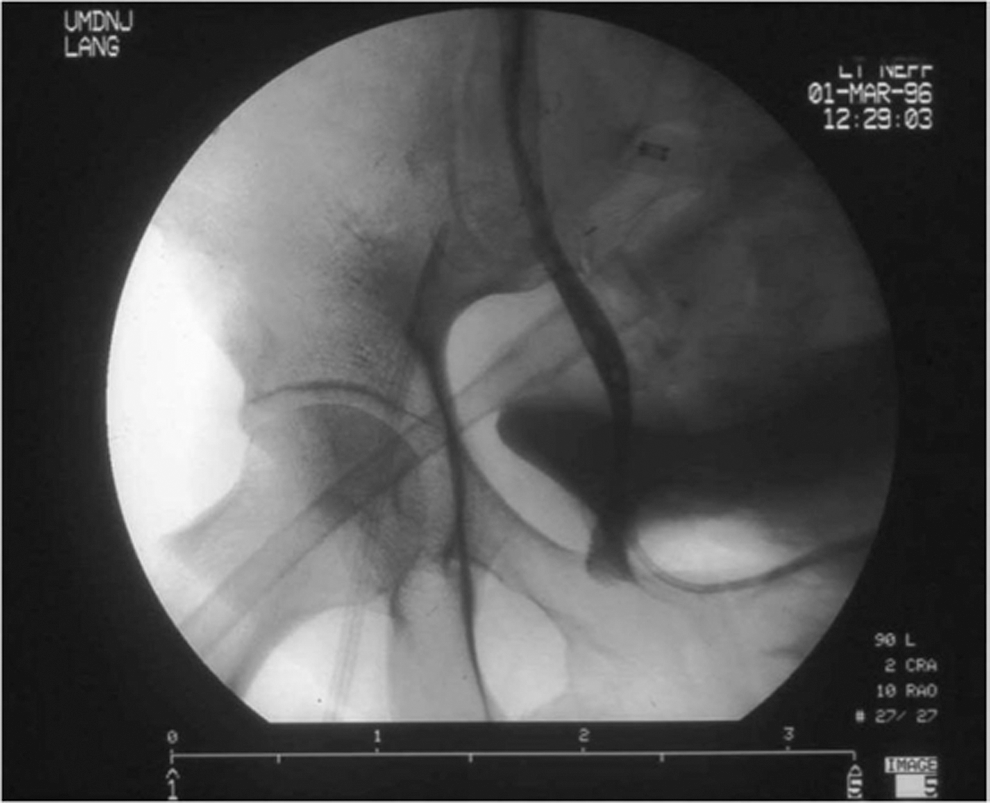
Deployment of Double-J endostent to counter secondary occlusion by either extrinsic compression or tumor ingrowth.

Extension Wallstent overlapping the original stent to alleviate cephalad tumor extension.
Intercurrent urinary tract infections occurred in only five patients and were controlled by appropriate antibiotic management.
The mean survival of our patients who had both Wallstents and supplementary endourologic procedures to maintain urinary function was 54 months. If one excluded the patients who failed to attain a creatinine level acceptable for chemotherapeutic treatment (n=6), however, the mean survival for the remainder in this group is 69 months. The mean survival for all patients treated for stage T3b cervical cancer after attempted stabilization of renal function by Wallstent and endourologic intervention was 75 months; excluding patients who did not receive chemotherapy (n=2), mean survival was 92 months. For patients with T4 cervical cancer, the overall survival was 38 months; when excluding the group not amenable to chemotherapy (n=4), the mean survival was 51 months. No patients were cancer free during the study period. Of note, however, the 5-year survival of our patients treated for stage IIIb cervical carcinoma was 60%. In comparison, the literature supports a 5-year survival rate for patients with stage IIIB cervical carcinoma of 32.4%, whereas the 5-year survival rate for patients with stage IVa cervical carcinoma is 16.1%, and that of stage IVb cervical carcinoma is 14.8%.
Four of 10 patients with T3b cervical cancer were alive between 108 and 140 months after stent placement. Two patients were followed for 46 and 82 months but were lost to follow-up. At their last appointment, however, both patients' creatinine levels were acceptable. Two patients died of intercurrent disease at 40 and 70 months, also with acceptable creatinine levels. Two died of cervical cancer at 4 and 12 months with high creatinine levels at their last clinic visit.
The low survival of patients with T4 cervical cancer reflects the advanced stage of the neoplasm. Four patients died of cervical cancer without commencing chemotherapy because they were unable to attain acceptable creatinine levels. Two patients were only able to undergo one chemotherapy session because they, too, were unable to attain acceptable creatinine levels (Fig. 3). Conversely, Wallstents and endourologic adjunct management kept creatinine levels at an acceptable level, allowing chemotherapy in three patients, who later succumbed to intercurrent disease (Table 1). Two patients lived for 108 and 112 months, respectively, also with acceptable creatinine levels. One patient completed three cycles of chemotherapy before succumbing to cervical cancer. Two patients were lost to follow-up after 28 and 44 months, but their creatinine levels were at an acceptable range at their last appointment.
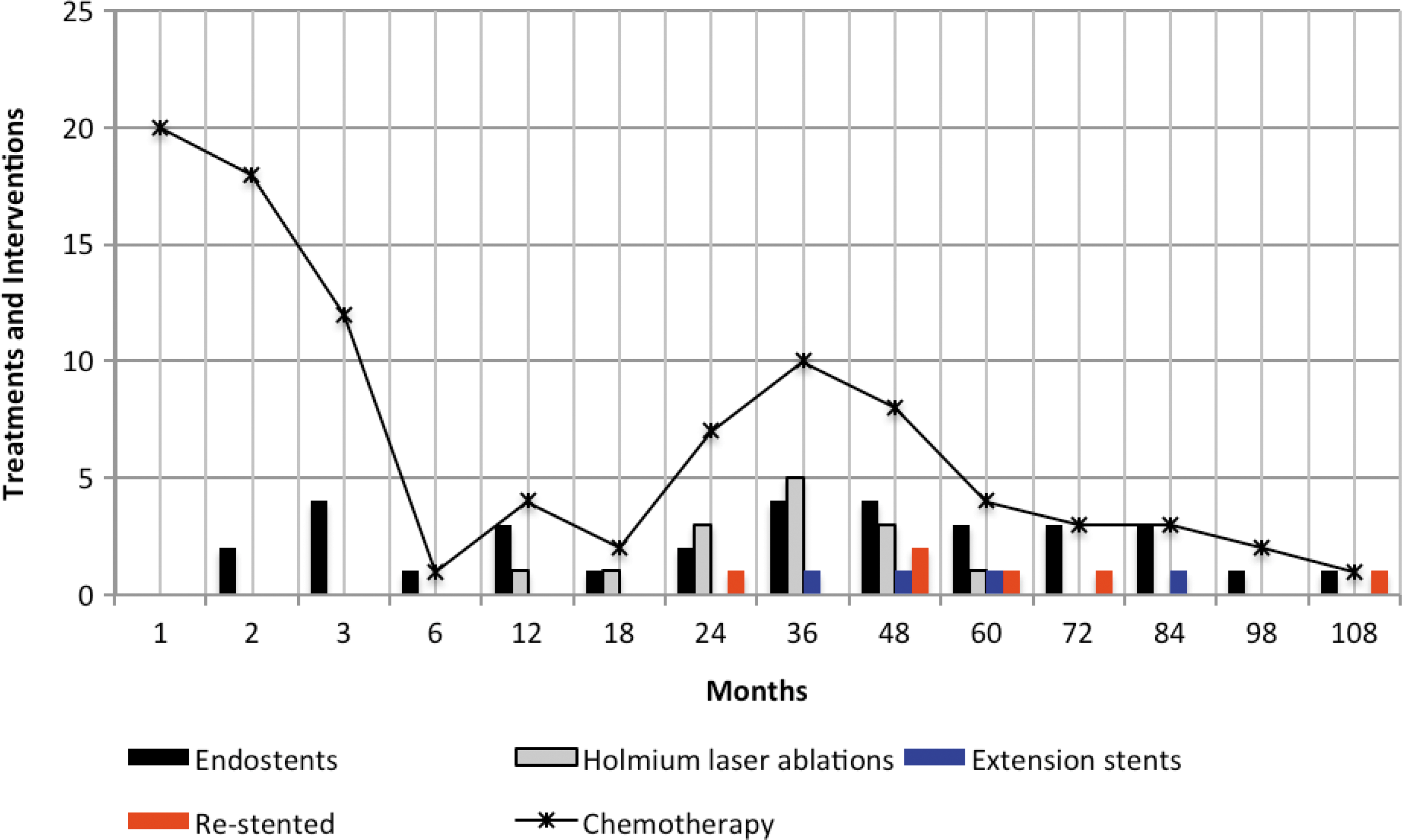
Number of interventions and cycles of chemotherapy over time.
LTF=lost to follow-up.
The technical success rate of Wallstent placement was 100%. The mean primary patency of the stent was 16.5 months. The mean secondary patency was 52 months (Table 2). For T3b patients, the mean primary patency was 20.6 months and for T4, as one might expect, only 13.6 months. Secondary patency for T3b patients was 73.9 months vs 36.4 months for T4 patients.
There were no serious complications associated with Wallstent placement. Minor complications included self-limited hematuria, minor irritating bladder symptoms, and urinary tract infections secondary to reflux through the stent.
Discussion
The efficacy of metallic stents to correct refractory ureteral strictures and obstructions is well established. Such stents have been successfully used in management of benign ureteral strictures 10 –12,18 and strictures of ureteroileal anastomosis, 19 transplant ureters, 20,21 and ureterocalicostomy anastomosis. 14
Metallic stents and particularly thermoexpandable metallic stents offer a significant advantage over polymeric Double-J stents. 15 Notably, because of the established low rate of encrustation and ingrowth, we now use resonance and thermoexpandable stents. Double-J stents have a high incidence of encrustation, dislocation, and migration, discomfort from bladder irritation, and failure in treatment of urogenic malignancies. Conversely, metallic stents are more resistant to extrinsic compression, encrustation, and offer a better primary and secondary patency rate, reported as 51.2% and 92.3%. 9,10 Moreover, they are more cost-effective than polymeric stents, $11.183 vs $23.999, 12 and also have a high potential for retrieval at 83.3%. 22 One must also consider the hospital stay and use of operative time for polymeric Double-J stents as opposed to metallic Wallstents. Patients who underwent polymeric Double-J stents needed an operating room, which generally costs more than an interventional radiology suite, as well as overnight observation secondary to a tendency for bleeding. Metallic Wallstent placement, however, was an ambulatory procedure performed in the interventional radiology suite.
Polymeric Double-J stents also necessitated more frequent exchanges: Over a 120-month period, given their tendency to migrate and encrust, patients needed an average of 60 exchanges. Thus, the mean patency rate for Double-J stents was 2 months, compared with a mean patency rate of 4 months for metallic stents. Moreover, in long-term survivors, the mean patency rate for metallic stents was 6.5 months. Thermoexpandable and Resonance® (Cook, Bloomington, IN) metallic stents became available during our study period and are now used instead of Wallstents secondary to their benefits of reduced ingrowth and hyperplastic reaction.
Quality of life appears to be significantly improved with metallic stents over polymeric stents as well. 16 Reported survival rates of patients treated with metallic stents for urinary obstruction caused by pelvic malignancies are highly variable, however, and are likely influenced by the underlying malignancy. 2,9,14 –16,23
Effective chemotherapy for advanced cervical cancer is dependent on acceptable renal function (a creatinine level below 1.8), which can be maintained when using metallic stents. 13
The goal of metallic stents to stabilize renal function (serum creatinine) and thus permit chemotherapy for the underlying cervical carcinoma was largely met in 19 of our 24 patients (79%). Six of our 24 patients survived for 108 to 140 weeks, maintaining creatinine levels of 1.6 to 3.6 over the entire treatment period. Three to eight chemotherapy cycles were possible in 18 patients, in whom creatinine had been lowered to acceptable levels.
Our mean primary patency rate of Wallstents was 54% over 18 months, similar to the rates of 51.2% reported in the literature. 9 To maintain the patency of the Wallstent and adequate urinary flow, 56 endourologic interventions had to be performed. Holmium laser ablation was used to remove ingrowth of neoplasms at the vesical end that compromised Wallstent patency 12 to 60 months after it had been seated. Double-J stents, extension stents, and replacement stents were deployed to counter effects of compression, angulation, and encrustation occurring 2 to 104 months after seating of the Wallstents. Migration of the stent in three of our patients was readily remedied by insertion of a new Wallstent (Fig. 3). The aforementioned additional interventions achieved a secondary patency rate of 100%, which is better than that reported in the current literature 9 (Table 2). Despite innumerable instrumentations and retention of endoprosthesis for up to 12 years, we encountered no incidence of pyonephrosis. Intermittently occurring urinary tract infections were managed successfully by antibiotic therapy. 2,9,15
As might be expected, death from the primary disease was higher in the advanced stage T4 cervical cancer than in T3b cervical cancer.
We acknowledge our limitations. Primarily, we used metallic Wallstents despite the availability of newer materials, such as Memokath (Pnn Medical) and Resonance (Cook Medical), during the study period. We also acknowledge that the metallic Wallstents tend to encrust more easily secondary to an absence of coating. In fact, holmium laser was needed in 14 patients to combat hyperplastic tissue ingrowth at the distal end of the stent. Even in patients who died of intercurrent disease (n=5) and those lost to follow-up (n=4), however, the goal of temporary stabilization of renal function, which is to allow chemotherapy treatment, was achieved. Overall, only five patients did not benefit from Wallstent placement and succumbed to cervical cancer in less than 1 year. We also realize that very few functional studies were performed. Radionuclide scans were used only to establish lack of function of a renal moiety.
Conclusion
Overall, Wallstents, complemented when needed by other endourologic interventions, met the goal to maintain urine flow and renal function, thereby allowing the extended chemotherapy treatment of cervical cancer with only minimal complications. The lifespan of patients, particularly with T3b carcinoma of the cervix, appears to be prolonged. Both lifespan and quality of life are positively impacted by Wallstents stabilizing urine drainage.
Footnotes
Disclosure Statement
No competing financial interests exist.