
Abstract
Purpose:
To determine the stage-specific operative, postoperative and oncologic outcomes, for patients undergoing a laparoscopic radical nephrectomy (LRN) for renal cell carcinoma (RCC) in a single center and assess changes over a generation of practice.
Patients and Methods:
From December 1992 to July 2011, data were collected prospectively for 854 consecutive simple laparoscopic necphrectomies (LNs) and LRNs, 397 of which were LRNs for RCC. The first LRN was performed in December 1997. Stage-specific surgical and oncologic outcomes were assessed across the study period. Patients were then grouped into three equal consecutive cohorts. Case mix and surgical outcomes were compared to assess changes with departmental experience.
Results:
There were 206, 71, 118, and 2 patients across stages pT1, pT2, pT3, and pT4, respectively. Median operative time was significantly shorter for pT1 tumors (125, 150 and 150 min for pT1–3, P<0.021), while median estimated blood loss (EBL) was greater for pT3 tumors (50, 50, 100 mL, for pT1–3, P<0.001). Median follow-up time was 31, 30, and 18 months, respectively, across pT1–pT3. There was a significant difference in 5-year overall survival (82.4%, 68.4%, 58.9%), cancer-specific survival (99.5%, 83.6%, 66.5%) and progression free survival (86.5%, 66.3%, 47.5%) across these stage-specific subgroups. Over the three cohorts, there was an increase in LRN performed for locally advanced disease and cytoreduction. With greater surgical experience, there was improvement in median operative time and median EBL in localized disease over the three periods, but no significant changes for locally advanced disease.
Conclusion:
This is the largest reported series of LRN in the United Kingdom. Departmental experience has resulted in improved surgical outcomes for localized RCC, with expansion of practice in more complex advanced disease. Laparoscopic nephrectomy is both operatively and oncologically safe in T1 and T2 disease, and although technically more demanding, it is also safe in selected T3 disease.
Introduction
Radical nephrectomy for RCC was first described in 1969 3 with laparoscopic nephrectomy subsequently reported first by Clayman and colleagues 4 in 1991. Since then, laparoscopic radical nephrectomy (LRN) has become the first-line treatment for localized RCC, when it is not amenable to partial nephrectomy. We aimed to determine the stage-specific operative, postoperative, and oncologic outcomes for patients undergoing a LRN for RCC in a single center and to assess any change over a generation of laparoscopic nephrectomy practice.
Patients and Methods
From September 1992 to July 2011, data were collected prospectively for 854 consecutive simple laparoscopic nephrectomies (LNs) and LRNs performed by one of three surgeons (DAT, SAM, ACPR) using a transperitoneal approach. Adrenalectomy was performed as part of a LRN, when there was a large upper pole tumor and the adrenal was believed to be abnormal or involved on preoperative imaging. The first LRN for RCC was performed in December 1997. Data for the LRNs performed for RCC between December 1997 and July 2011 are presented and analyzed. Information recorded included patient demographics, operative details, postoperative course, and pathology results. Postoperative complications were recorded using the Clavien-Dindo classification. 5 Follow-up data and any omissions from the prospectively collected data were completed retrospectively by review of hospital case notes. Length of follow-up was determined by the time between nephrectomy and last clinical contact. In those patients who died, cause of death was taken from the case notes or from the death certificates obtained from the General Registry Office of Scotland when not available in the notes.
Cancer-specific survival (CSS) was determined if the cause was directly attributable to RCC. Progression-free survival (PFS) was calculated based on the time from surgery to disease recurrence when present. All patients were staged based on the AJCC Cancer Staging Manual, 6th edition (Table 1). 6 Comparisons were first made based on pathologic tumor stage. Secondly, patients were grouped consecutively into three equally sized patient cohorts and compared to assess change in surgical outcomes with increased departmental experience. Finally, outcomes for cytoreductive nephrectomy were detailed and compared with that for nephrectomy with a curative intent.
Unpaired t test and one-way analysis of variance were used to compare continuous variables and the chi-square test for categorical data. The Kaplan-Meier method was used for survival predictions. Statistical analysis was performed using PASW version 18.0 (SPSS Inc., Chicago, IL); P<0.05 was taken to indicate significance.
Results
Of the 854 LNs performed, 397 were for pathologically confirmed RCC, 30 were for oncocytoma, 285 were for nonfunctioning kidneys with stone disease or chronic infection, three were for rare non-RCC tumors, and 139 were laparoscopic nephroureterectomies for upper urinary tract transitional cell carcinomas. These were performed sequentially by the three surgeons DAT (1992–2009, LN=317, LRN=42); SAM (2002–2010, LN=291, LRN=195); and ACPR (2006–2011, LN=246, LRN=160). Only LRN for RCC were assessed further during this study.
Patients undergoing LRN for RCC were grouped by pathologic tumor stage with 206, 71, 118, and 2 patients staged as pT1, pT2, pT3, and pT4, respectively. There was no difference in sex across the tumor stages; however, those undergoing LRN for T3 disease were significantly older (P=0.026). There were significant differences in distributions of tumor grade (P<0.001) and histologic subtype (P=0.021) across tumor stages (Table 2).
Preoperative staging results are not available for all patients. Of note, however, there were two cases of pT4 disease for which staging was available. Both were clinically staged as T2 disease; the first case had to be converted to open nephrectomy because of failure to progress while in the second case, in which the tumor was reported as abutting the liver, the tumor was excised laparoscopically. Both patients had early recurrence and died from their disease.
Comparing surgical outcomes in stages pT1–T3, median operative time was significantly shorter in those with pT1 tumors (125 min [range 70–240], 150 min [range 80–270] and 150 min [range 80–320], respectively; P=0.021), while median estimated blood loss (EBL) was greater in those with pT3 tumors (50 mL [range 0–1500], 50 mL [range 5–1200], and 100 mL [range 0–3000]; P<0.001). This stage related difference in blood loss reflected the transfusion rates of 2.8%, 6.3%, and 10.8%, respectively, although this was not statistically significant (P=0.054). There was no significant difference in all cause postoperative morbidity (32%, 20%, 41%, respectively; P=0.052) and median postoperative stay (4.0, 4.0, 5.0 days respectively; P=0.267).
Median follow-up time was 26 months overall (range 0–147 mos; quartiles 11.5 and 49 mos) and 31, 30, and 18 months respectively across pT1–pT3. As expected, there was a significant difference in 5-year overall survival (OS; 82.4%, 68.4%, 58.9%), CSS (99.5%, 83.6%, 66.5%) and PFS (86.5%, 66.3%, 47.5%) across pT1, pT2, and pT3 tumors, respectively (Table 3 and Figs. 1 –3, P<0.001).

Kaplan-Meier: Stage-related overall survival.
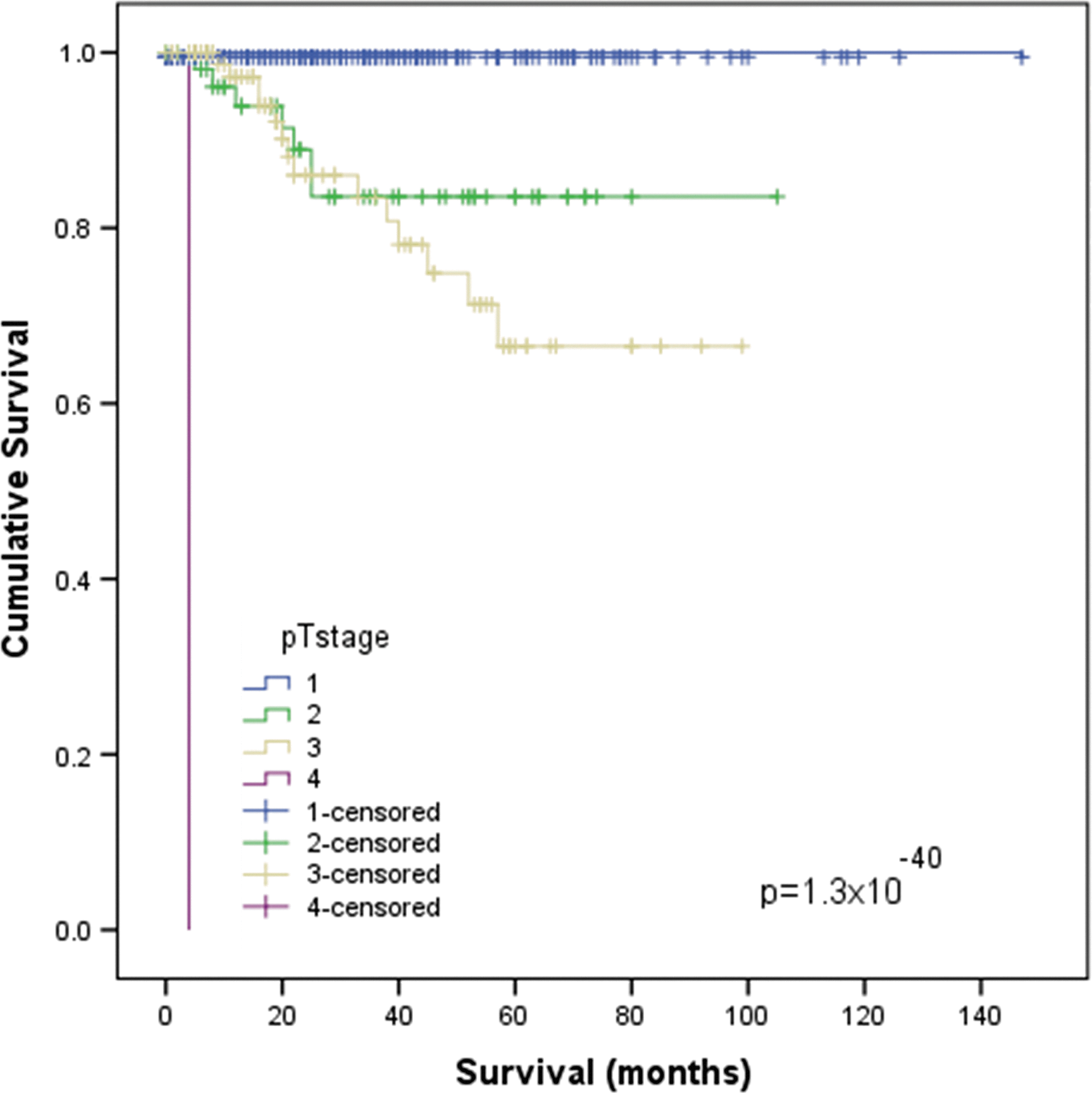
Kaplan-Meier: Stage-related cancer-specific survival.
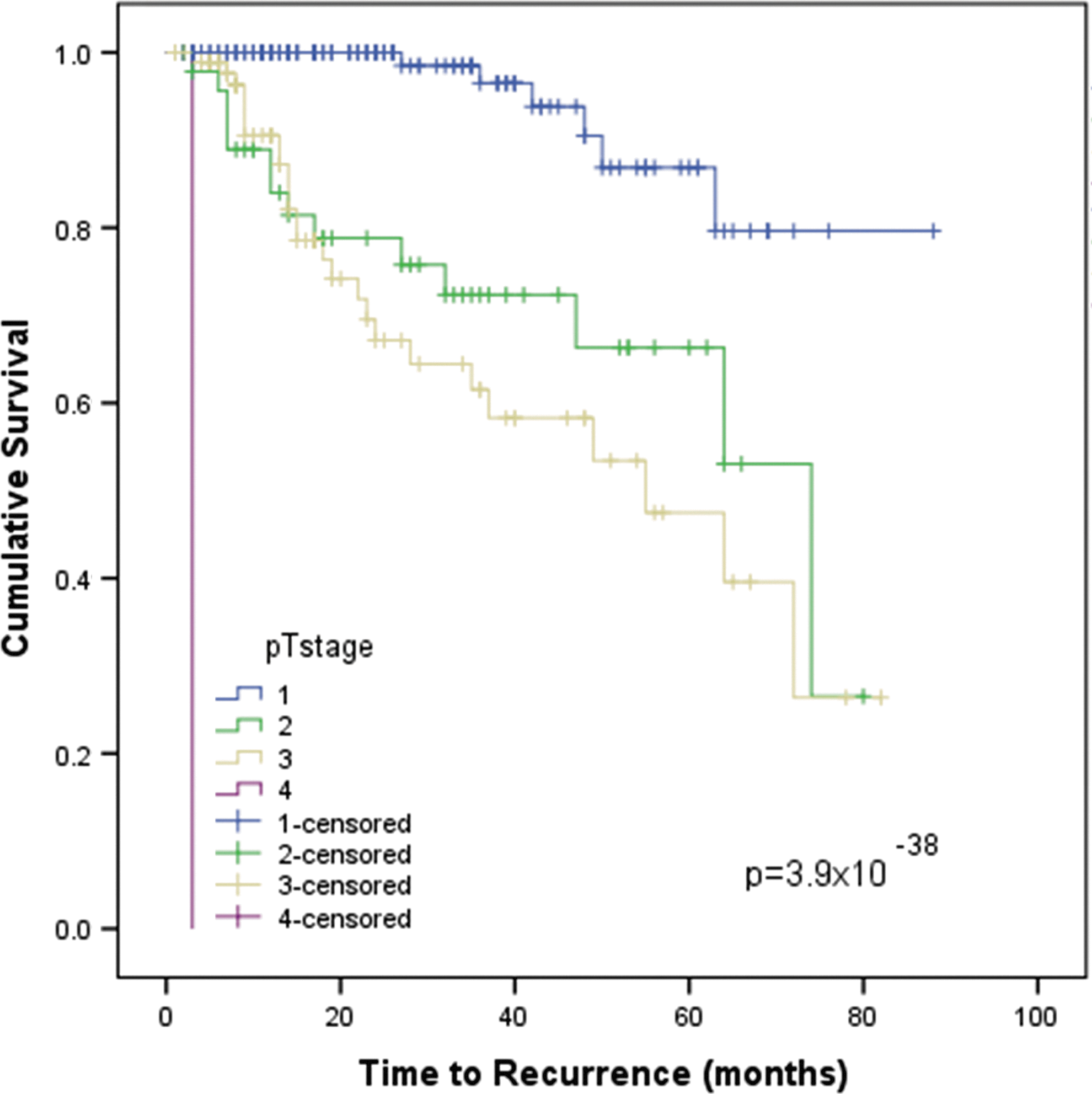
Kaplan-Meier: Stage-related progression-free survival.
OS=overall survival; CSS=cancer-specific survival; PFS=progression-free survival.
The data were grouped into three cohorts to reflect the increasing experience of the department for comparison of caseload and operative outcomes. The three groups (A, B, C) contained 132, 133, and 132 consecutive cases reflecting early, intermediate, and recent experience in periods: 01/12/1997 to 23/02/2006, 28/02/2006 to 16/06/2008, and 17/07/2008 to 02/07/2011, respectively. There were no differences in patient sex or age over these periods (P=0.225 and P=0.827, respectively). Operative outcomes were assessed over the three cohorts, with subgroup analysis for localized disease (T1/2) and locally advanced disease (T3/4).
Over these three periods, there was a significant increase in LRN utility for locally advanced RCC (T3/4) (P=0.001, Fig. 4). Furthermore, there were an increased number of nephrectomies for cytoreduction in the context of metastatic disease over the three cohorts (1, 9, and 33, respectively; P<0.001).

Caseload of laparoscopic radical nephrectomy over three cohorts of operative experience, based on disease stage.
There was a significant reduction in median operative time of LRN for localized RCC over the three cohorts with accrued experience (145, 130, and 120 min; Fig. 5; P<0.001). While median operating time for locally advanced tumors is significantly higher than that of the localized tumors, there has been no significant reduction in operative time with accrued experience over the three cohorts (153, 160, and 150 min; Fig. 5; P=0.814).
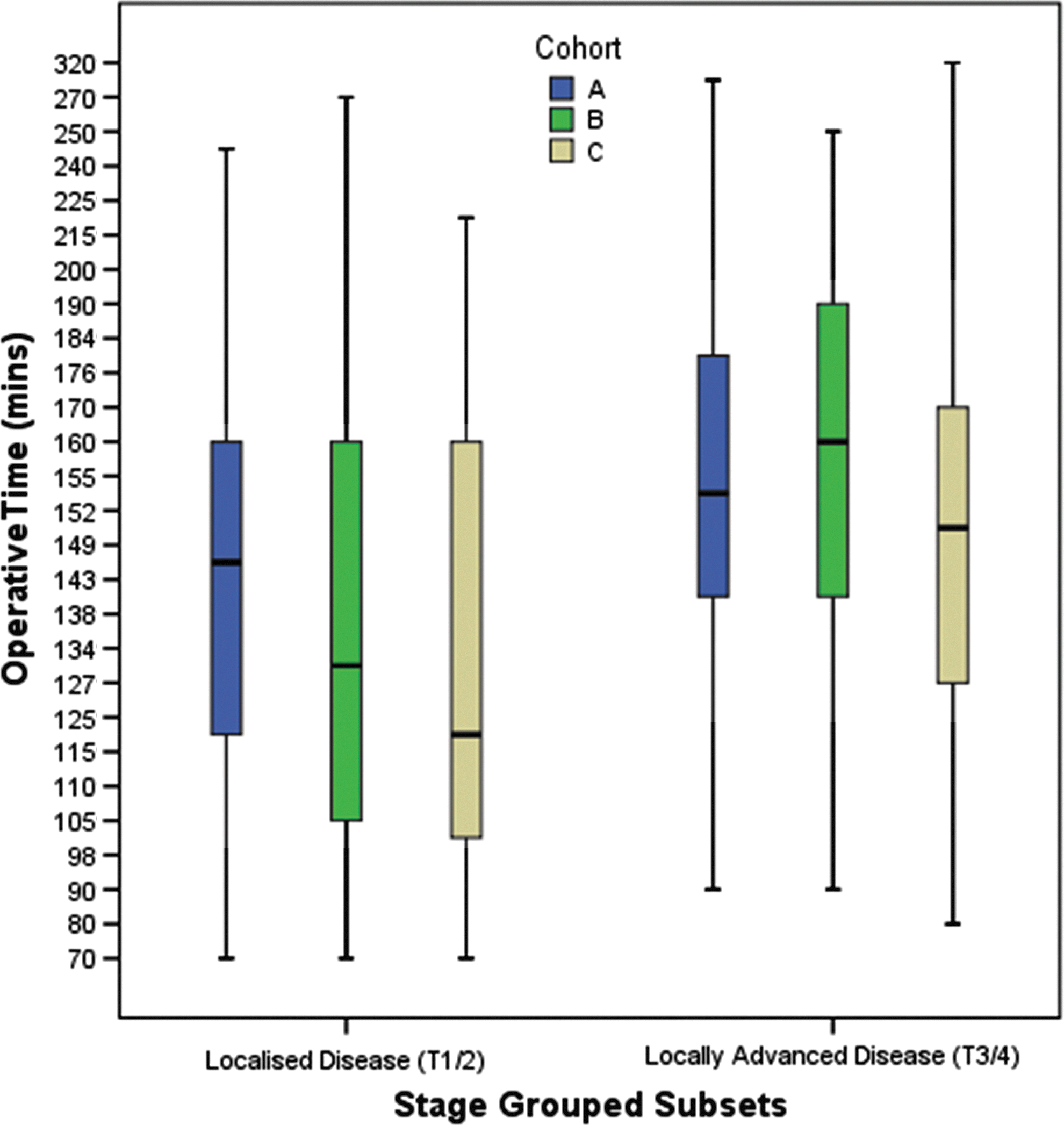
Operative time for laparoscopic radical nephrectomy for each cohort based on pathology (localized and locally advanced). There was a progressive reduction in median operative time with accrued experience for localized disease, but not for locally advanced disease.
Similar findings have been shown with EBL. There has been a significant reduction in median EBL over the three cohorts with localized disease (150, 104, and 40 mL; Fig. 6; P=0.02). While median EBL in the advanced disease groups has shown no significant change, it remains within accepted limits (100, 225, and 100 mL; Fig. 6; P=0.926). There was no significant change in the transfusion rate for localized or locally advanced disease over the three cohorts (P=0.623 and P=0.261, respectively). Over the three cohorts, there were 5, 4, and 5 conversions, respectively, which were not statistically different (P=0.924).
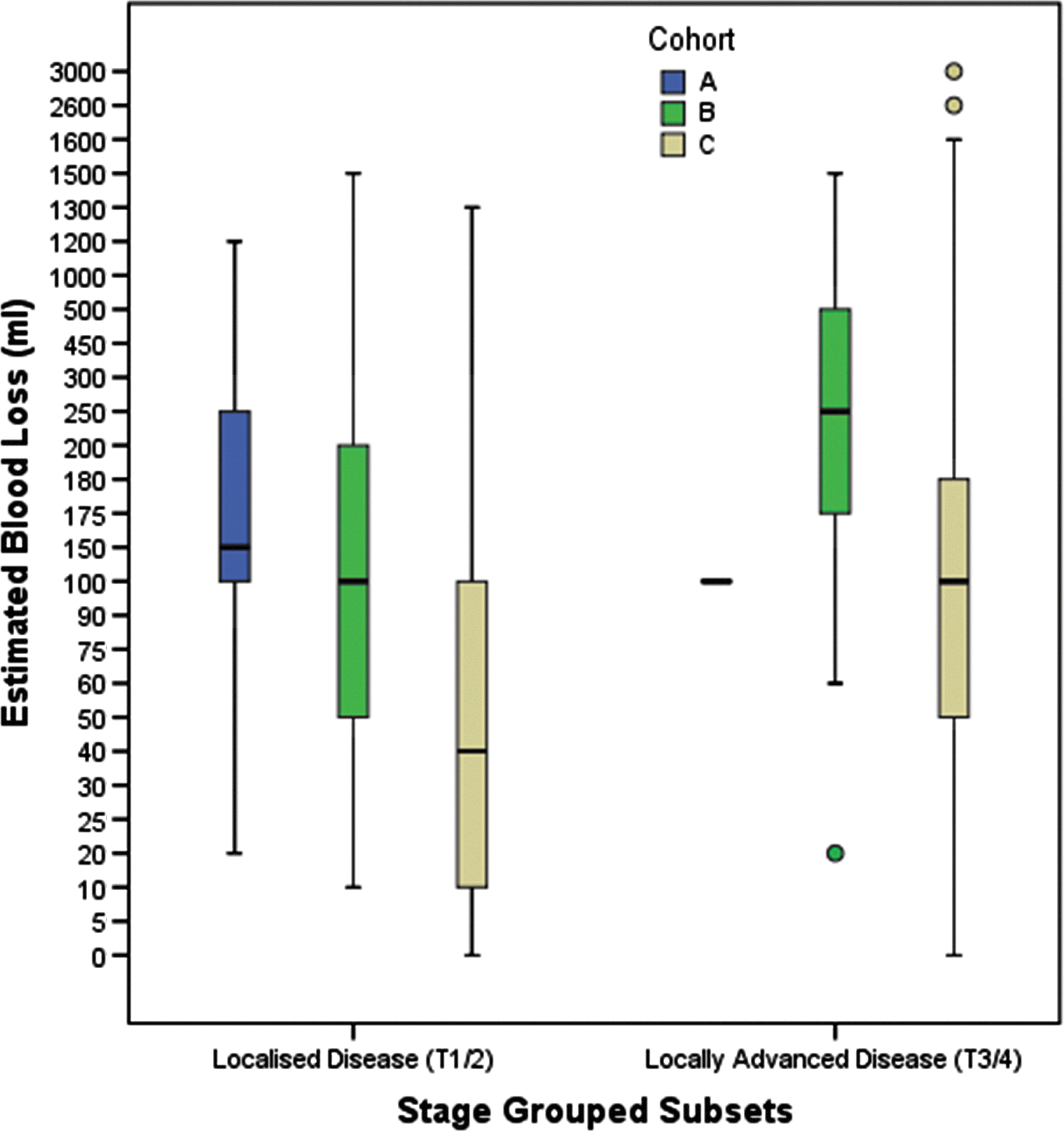
Estimated blood loss for laparoscopic radical nephrectomy for each cohort based on pathology (localized and locally advanced). There was a reduction in operative blood loss with accrued experience for localized disease, but not for locally advanced disease.
There was a significant increase in postoperative morbidity over the study periods (Table 4, P=0.006). This held true when localized and advanced cases were analyzed independently. These were classified by Clavien-Dindo Score and were mainly in classes I and II. Of those patients who experience complications, six were grade IV complications. The distribution can be seen in Table 4.
Acute severe renal failure in Patient 1 was managed conservatively, and septic shock developed in Patient 2 as a result of post-operative pneumonia.
Patient 3 had an allergic reaction to gelofusin and left ventricular failure developed, which was managed in the intensive care unit.
The acute left ventricular failure that developed in Patient 4 was managed with nitrate infusion in the high dependency unit.
Cardiogenic shock developed in Patient 5 as a result of a myocardial infarction.
Severe sepsis, renal failure, and fluid overload developed in Patient 6, but the patient improved with medical management.
In one patient, 82 years old with Parkinson's disease who had a combined LRN and colectomy, pneumonia developed, and the patient died from respiratory failure.
The cytoreductive group was assessed independently and compared with the curative group. The mean age of the cytoreductive group was 65 (range 32–83) years with a male to female ratio of 24:19. The median operative time was 156 min (range 75–260), median blood loss 316 mL (range 10–2600), and median length of hospital stay was 7 days (range 3–57). There was a significant difference in the distribution of cases by pT stage between the cytoreductive and curative nephrectomy groups, with a reduction in pT1 cases and an increase in pT3 and pT4 cases (P=0.009, Table 5). There was no significant difference in the median operative time, EBL or median hospital stay between the two groups, when matched for pT stage (Table 5). There was no difference in overall complication rate between those undergoing cytoreductive nephrectomy and those undergoing a curative nephrectomy (41.9% and 35.6%, respectively, P=0.420). There was, however, significantly more grade IV complications and a trend toward higher grade III complications in the cytoreductive group (Table 5, P=0.009 and P=0.063, respectively).
LRN=laparoscopic radical nephrectomy.
Discussion
This study confirms that LRN is operatively safe for localized and selected advanced RCC with acceptable oncologic outcomes. We have also shown improved surgical outcomes for LRN performed for localized disease with experience. While outcomes for LRN in advanced disease are acceptable, there was no significant improvement with experience, highlighting their complexity. Finally, contrary to previous reports we have shown no significant difference in surgical outcomes for cytoreductive LRN compared with curative LRN.
There are a number of strengths to this study. To our knowledge this is the largest reported United Kingdom series of LNs. All cases were performed in a single center allowing for uniformity of follow-up and outcomes. Furthermore, all three consultant surgeons, as well as any juniors involved, were sequentially trained and mentored using a modular training approach, 7 ensuring standardization of the procedure. Databases were collated prospectively, with retrospective validation, ensuring good quality data capture. We do, however, accept the inherent weakness of retrospective follow-up data, and acknowledge the relatively short overall median follow-up of 26 months. It should also be highlighted that the results are based on pathologic tumor staging, rather than preoperative clinical staging, and this should be appreciated when interpreting outcomes.
This work supports the endorsement of LN as the standard of care in pT1 and pT2 renal cancer not amenable to partial nephrectomy (PN). Mean operative time has been previously reported at approximately 130 minutes for open nephrectomy. 8,9 Mean EBL ranged from 357 mL to 451 mL in these same open series. Postoperative stay was also much longer after open nephrectomy, ranging from 8.8 to 11 days. 8,9 Our case series has similar operative time, with more favorable blood loss, transfusion rates, and reduced hospital stay when compared to open series.
More recently, there has been increasing support for LRN in selected advanced (T3) disease when performed by experienced surgeons. 10 –12 As we have reported, 13 the present study has found similar operative time, blood loss, transfusion rates, and hospital stay to results of LRN for T3 disease published in the literature, which are favorable to those reported for open nephrectomy. This supports the operative safety of LRN nephrectomy for pT3 disease. We do, however, note that although there is no statistical difference in complication rate between LRN for T1–3, there is a trend for higher complication rate for T3 disease (mainly grades 1 and 2). This higher complication rate in advanced disease is supported by others, and this should be considered when counseling patients. 14
Importantly, as well as the operative safety of LRN in all pT1, pT2, and pT3 disease, we present similar oncologic outcomes compared with both open and other laparoscopic series. A 5-year OS rate between 68% and 84% has been shown by others, 15,16 with a 5-year CSS ranging from 83% to 98% 17 –20 after nephrectomy in T1 disease. Our reported 5-year OS and CSS rates of 82.4% and 99.5% compare well. Frank and associates 17 published oncologic outcomes in a large series of nephrectomies, with 5-year CSS of 70.5% for T2 disease and 53.4% and 43.8% for T3a and T3b, respectively. Our reported results of 83.6% and 66.5% 5-year CSS for pT2 and pT3 disease are favorable. It is possible that our superior results are because of selection bias. The data published do not allow for accurate comparison of other variables such as mean tumor size, histologic subtype, or Fuhrman grade, although these do appear broadly similar. Nonetheless, our survival data support the oncologic safety of LRN.
PN for selected T1 disease has been shown to have equivalent 5-year CSS to LRN with rates published between 94% to 98.3%. 21 –23 These are comparable to our results for T1 disease. Some studies comparing OS in PN and LRN have shown benefit with PN in both OS and risk of cardiovascular death, implicating the importance of nephron sparing. 15,23 –25 Our 5-year OS for pT1 RCC of 82.4% is marginally less than that reported in the literature for PN with a range of 85% to 87% 23,25 ; however, this is not adjusted for age, preoperative renal function, or comorbidities. Although not reported in these results, we have noted an increase in the utility of PNs in our center over the last 5 years, and this is likely to change the demographics of our LRN practice further in the future.
We thought it was important to review caseload and surgical outcomes over time to assess the importance of departmental experience. Over the three study periods, there was a significant increase in LNs for locally advanced disease or for cytoreduction in the context of metastatic disease. This is likely to reflect the increased skill and confidence of the surgeon with experience as well as changes in oncologic management. We demonstrate improved surgical outcomes in those undergoing nephrectomy for pT1/2 disease, with reduced operative time and blood loss, over the three periods. The median estimated blood loss over the three periods improved from 150 mL to 40 mL. This is comparable to results of LRN series published by others with median EBL of 100 to 280 mL for T1 disease 8,26 –28 and 200 to 245 mL for T2 disease. 28,29 There was no difference in transfusion rate over the three cohorts for localized disease, which was similar to other series, 14 because of the relatively small EBL experienced. Experience did result in a reduction in median operative time over the three periods, from 145 to 120 minutes, in this subgroup. Again, this is akin to published median operative time for LRN of 134 to 256 minutes. 8,26,28,29
These improvements in surgical outcomes over the three cohorts are likely to be in part related to the learning curve for LN. This principle of a learning curve is well accepted, and improved operative time and blood loss have been reported with individual experience. 27 This study may suggest that cumulative departmental or institutional experience is also important. This may be particularly true when sequential mentoring with modular training is in place, because this allows efficient and effective training, as we have reported. 7
Despite the improved surgical outcomes seen in LRN for localized disease, this was not mirrored with LRN for locally advanced disease. There was no significant difference in blood loss, transfusion rate, or operative time with increased experience. Our results were favorable when compared with other series, which report a mean EBL of 200 mL and operative time of 210 minutes. 11,30 The lack of improvement is likely to reflect the complexity of the procedure in which the challenges of laparoscopic surgery for advanced disease remain high, despite accrued experience. Even though there is an increased caseload of complex LRN, however, there was no increase in conversion rate, which remained static at 3%. This is broadly similar to that reported by others with a range of 1.5% to 4.8% 26,29 and below the 6% rate published in the 2011 British Association of Urological Surgeons (BAUS) national audit. 31
Our comparison between LRN with curative intent and cytoreductive LRN revealed no significant difference in surgical outcomes when matched for disease stage. This is contrary to the literature, which suggests cytoreductive nephrectomy has a higher blood loss, transfusion rate, complication rate, and in-hospital mortality compared with curative nephrectomy, although there was no control for tumor stage. 32 Nonetheless, we did note a higher rate of significant complications (grades III and IV) in the cytoreductive group, which is likely the result of the poorer functional reserve held by these patients rather than related to technical difficulty.
Overall, our reported morbidity of 37% is relatively high, being at the upper range of that reported in the literature (9.6%–38%). 27,33 –35 Our results are also much higher than that published in the BAUS national 2011 audit, 31 with a rate of 10.4%. In 26.3% of cases, however, no data were submitted for postoperative complication. We believe this apparent increase is because of more consistent and accurate reporting of minor complications (grades I/II) in our series. Furthermore, our overall rate of serious complications (grades III/IV) and death (grade V) are similar to that published by others. 31,36 We did notice an increase in grades I and II complications over the three study periods. This may also reflect more accurate reporting over time but may also be the result of increased caseload of LRN for cytoreduction and advanced disease with higher blood loss and operative time. Unfortunately, we do not have data on the patients' comorbidities, which may also be contributing to these findings.
Conclusion
We describe the largest reported series of LRN in the United Kingdom. Departmental experience has resulted in improved surgical outcomes for localized RCC, with expansion of practice in more complex advanced disease. LN is both operatively and oncologically safe in T1 and T2 disease, and although technically more demanding, it is also safe in selected T3 disease.
Footnotes
Acknowledgments
Thank you to The Royal College of Surgeons of Edinburgh's Robertson Trust, The Melville Trust for the care and cure of cancer, and the Medical Research Council Scottish Clinical Pharmacology and Pathology Programme, which supports the work of Mr. Alexander Laird, Clinical Research Fellow.
Disclosure Statement
No competing financial interests exist.