
Abstract
Background and Purpose:
The forces needed to move the ureteroscope up and down the urinary tract may injure the ureter, but a method to measure these forces in patients is lacking. The purpose of the study was to develop and test a novel method for measuring the pushing and pulling forces exerted on a semirigid ureteroscope during ureteroscopy (URS) in a clinical setting.
Materials and Methods:
During 2010 to 2011, 20 patients planned for retrograde flexible URS or percutaneous lithotripsy for renal pelvic stones were recruited to a study measuring the forces exerted on a semirigid ureteroscope during retrograde URS. A coupling device was constructed to connect a digital force meter to a standard semirigid ureteroscope. The pushing and pulling forces, given in Newton (N), were measured at four defined locations in the ureter. The experiment was repeated twice to evaluate the reproducibility of the results. Paired-samples t test and Intraclass Correlation Coefficient (ICC) addressed the reproducibility of the results.
Results:
The force meter did not disturb the endoscopic procedure, and the force measurements were performed as intended. The results were reproducible at repeated measurements, with the ICC ranging from minimum 0.737 to maximum 0.812 at the different measuring locations in the ureter. The mean forces needed for insertion of the ureteroscope increased from 4.4 N (±3.6 N) at the distal part of the ureter to 9.7 N (±7.3 N) at the proximal part with large interpatient variation. Similar but smaller forces were found for retraction.
Conclusion:
The present method is proven to reliably measure forces exerted on the ureteroscope in a clinical setting. This opens the opportunity for further force studies on endoscopic procedures to make URS safer.
Introduction
The purpose of the present study has been to develop and test a novel method for measuring the pushing and pulling forces exerted on a semirigid ureteroscope during URS in a normal clinical setting.
Materials and Methods
Study population
Adult patients with renal pelvic stones planned for endoscopic treatment either with retrograde flexible URS or percutaneous lithotripsy at Haukeland University Hospital were recruited to this method study during 2010 to 2011. The inclusion criteria were normal renal function and assumed normal ureters. Patients with Double-J stents, ureteral stones, ureteral strictures, or other known ureteral pathology were excluded from enrollment. The patients were recruited consecutively. The candidates received verbal and written information about the study and signed a written consent before enrollment. Only one patient fulfilling the inclusion criteria refused enrollment. A total of 20 patients were enrolled in the study comprising 11 females and nine males, mean age 54 years (range 18–81 years). Force measurements were performed on the right side in four patients and on the left side in 16 according to the side of the renal pelvic stones.
This method study is the first part of a trial comparing the pushing and pulling forces during URS performed with and without a safety guidewire in the ureter. Results of that trial will be published later in a separate article.
Technical instruments
A standard semirigid ureteroscope with an 8.5F tapering shaft (Richard Wolf Medical Instruments Corporation, Vernon Hills, IL) was used for the force measurements during the URS procedures. A digital force meter (Dual Range Force Sensor, Fourier Systems Ltd., Rosh HÁayin, Israel) was mounted to the ureteroscope by means of an aluminum coupling device, which has been developed in collaboration with the department of medical technology at our institution (Fig. 1).
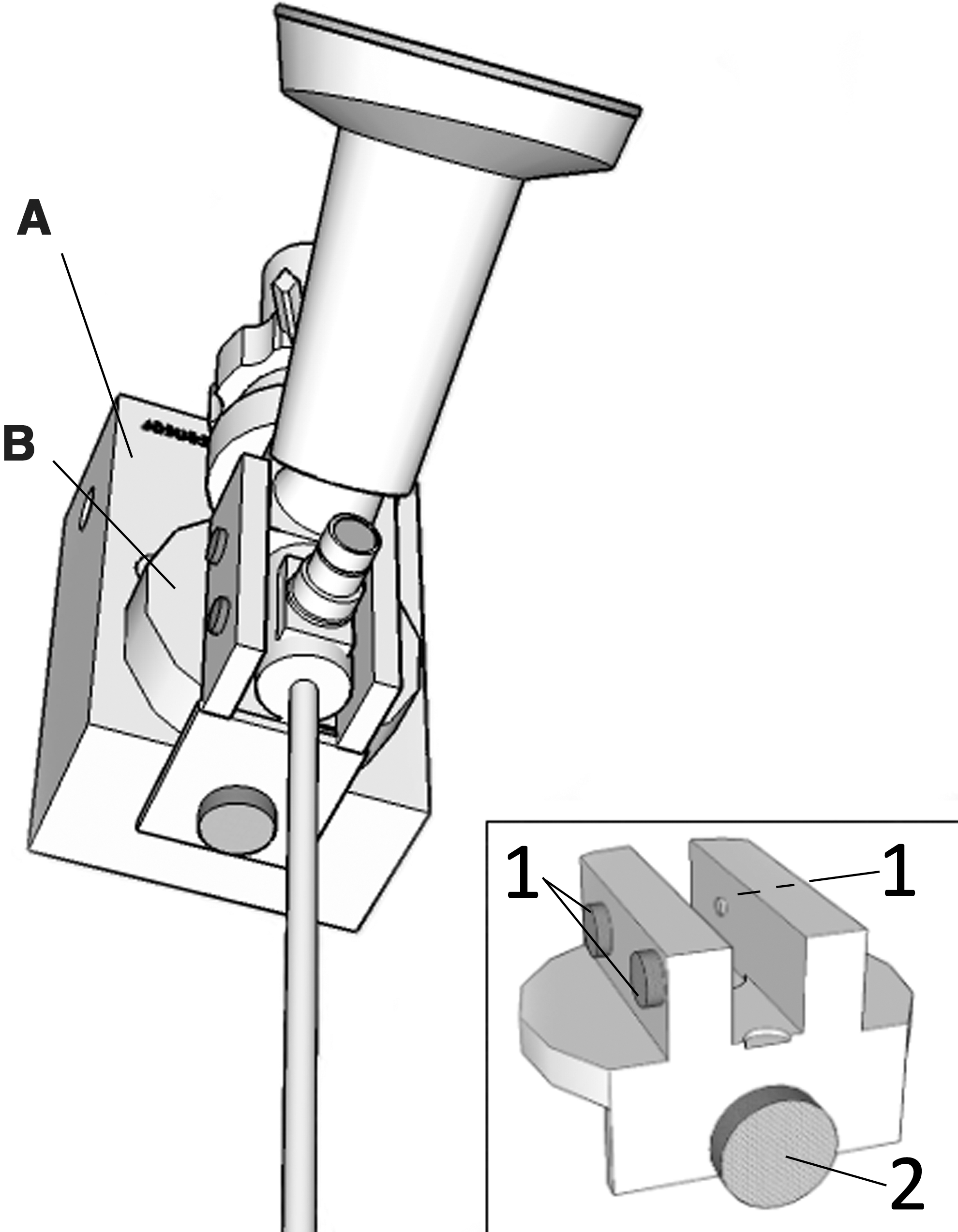
The semirigid ureteroscope mounted on a digital force meter
When moving the ureteroscope up and down the ureter, the urologist held a steady grip around the force meter without touching the ureteroscope itself. The pushing and pulling forces were thereby transferred from the urologist's hand to the force meter.
The force meter was connected to a computer, and a data program (MultiLab™ version 1.4.20, Fourier Systems Ltd., Rosh HÁayin, Israel) displayed the force measurements as line graphs on a screen simultaneously with the video vision from the endoscopy (Fig. 2).

The data program produces a continuous graph representing the pushing and pulling forces during insertion and retraction of the ureteroscope, in this case at the crossing iliac vessels. Video from the endoscopy is displayed in the upper right corner. See text for further details.
Measurements and data collection
Under regional anesthesia and under fluoroscopic guidance, a hydrophilic guidewire (Terumo Glidewire® 0.035", Terumo Medical Corporation, Somereset, NJ) was placed in the ureter during cystoscopy and secured to the sterile draping. The ureteroscope was then inserted in the ureter alongside the safety guidewire. A second guidewire was inserted through the working channel inside the ureteroscope.
Force measurements were performed during insertion and retraction of the endoscope with the tip of the ureteroscope at four defined locations in the ureter: In the intramural part of the ureter, at the crossing of the iliac vessels, at the iliac crest, and 5 cm distal to the ureteropelvic junction (UPJ). The position of the ureteroscope was verified by fluoroscopy. The ureteroscope was slowly advanced and retracted approximately 3 cm at each of the four locations during the force measurements with the endoscope kept in a horizontal position. The operating table was tilted as necessary to maintain a horizontal position of the ureteroscope during the measurements. Both the measurements of the insertion and retraction forces were performed at one location in the ureter before the endoscope was advanced further up to the next location. To evaluate the reproducibility of the results, the force measurements were repeated at the four locations during a second insertion of the ureteroscope.
The forces were given in Newton (N) as positive values for pushing and negative values for pulling forces. The force meter was set to register 10 measurements per second, giving a smooth continuous line graph. The maximum pushing and pulling forces were defined as the highest positive and lowest negative forces measured at each of the four locations in the ureter.
Figure 2 displays a graph representing the forces measured in one patient with the tip of the ureteroscope at the iliac crest. The first part of the graph is steep as the pushing force increases until reaching a maximum when the ureteroscope starts to move in the proximal direction. As the advancement of the endoscope is stopped, the force graph declines back to zero. A similar but negative graph shows the pulling forces exerted during retraction.
Statistics and approval
The insertion and retraction forces exerted on the ureteroscope were compared using paired-samples t tests. The maximum pushing and pulling forces at each of the four locations during the first and second URS were compared using paired-samples t tests and Intraclass Correlation Coefficient (ICC). ICC expresses the degree of agreement between the two sets of force measurements. ICC value 1 indicates perfect agreement and 0 indicates no agreement at all. 2 Comparison of the forces exerted on the ureteroscope in the right and left ureters, and comparison of the forces in males and females, were performed using independent samples t tests.
IBM SPSS Statistics 20 (IBM, Armonk, NY) was used for statistical analyses. A P value less than 0.05 determined statistical significance. Values are reported as means±standard deviation.
The experimental study project was approved by The National Committees for Research Ethics in Norway (ID-no: 102.09 REK) and Norwegian Social Science Data Services (ID-no: 21835 NSD), and has been registered in the clinical research database, ClinicalTrials.gov (ID: NCT01117701).
Results
With the force meter connected to the endoscope, the urologist could easily perform the URS with a steady grip around the force meter without touching the endoscope. This secured a complete transmission of the operator's hand movements to the endoscope via the force meter. As the force meter measured only the pushing and pulling forces along the long axis of the endoscope, forces that rotated the endoscope or moved it sideways could not be recorded. The mean extra operating time spent to complete the force measurements in each patient was 20 minutes (range 14–30 min). There was no need for balloon dilation of the ureteral orifice or lower ureter in any patient before the insertion of the ureteroscope.
The method worked as intended. The pushing and pulling forces could be measured in all patients, but complete recording of the forces could not be performed at all the four locations in three patients because of either computer recording failure or failure to advance the ureteroscope into the correct position for the measurements in the upper part of the ureter. As a mean for all patients, the forces needed for insertion of the ureteroscope increased from 4.4±3.6 N at the distal part in the intramural ureter to 9.7±7.3 N at the proximal part just below the UPJ. The mean forces for retraction were −3.3±2.8 N in the lower ureter and −7.5±5.1 N under the UPJ (Table 1).
Values are given as mean±standard deviation. P values refer to paired-samples t test comparing 1. and 2. Measurements.
N=Newton; ICC=Intraclass Correlation Coefficient.
As indicated by the large standard deviations from the means, the forces varied substantially from one patient to another. Thus, the pushing force at the level of the iliac crest ranged from a minimum 1.3 N in one patient to a maximum of 23.2 N in another. The extreme values were confirmed when repeating the measurements at the second insertion of the ureteroscope.
There were no significant differences between the force values found at the first compared with the second series of force measurements except for the retraction forces at the position just under the UPJ where significantly greater force was needed to extract the endoscope in the second series of measurements (−7.5±5.1 N vs −10.2±5.3 N, P=0.002).
The ICC for evaluating the agreement of the repeated measurements ranged from 0.737 to 0.812. The ICC values for each of the four locations in the ureter are given in Table 1.
A comparison of the insertion and retraction forces of the ureteroscope at different locations in the ureter is shown in Figure 3 with the retraction forces given as absolute values rather than negative values. The forces needed for retraction of the ureteroscope were significantly lower than those needed for insertion except at the level where the ureter crosses the iliac vessels.
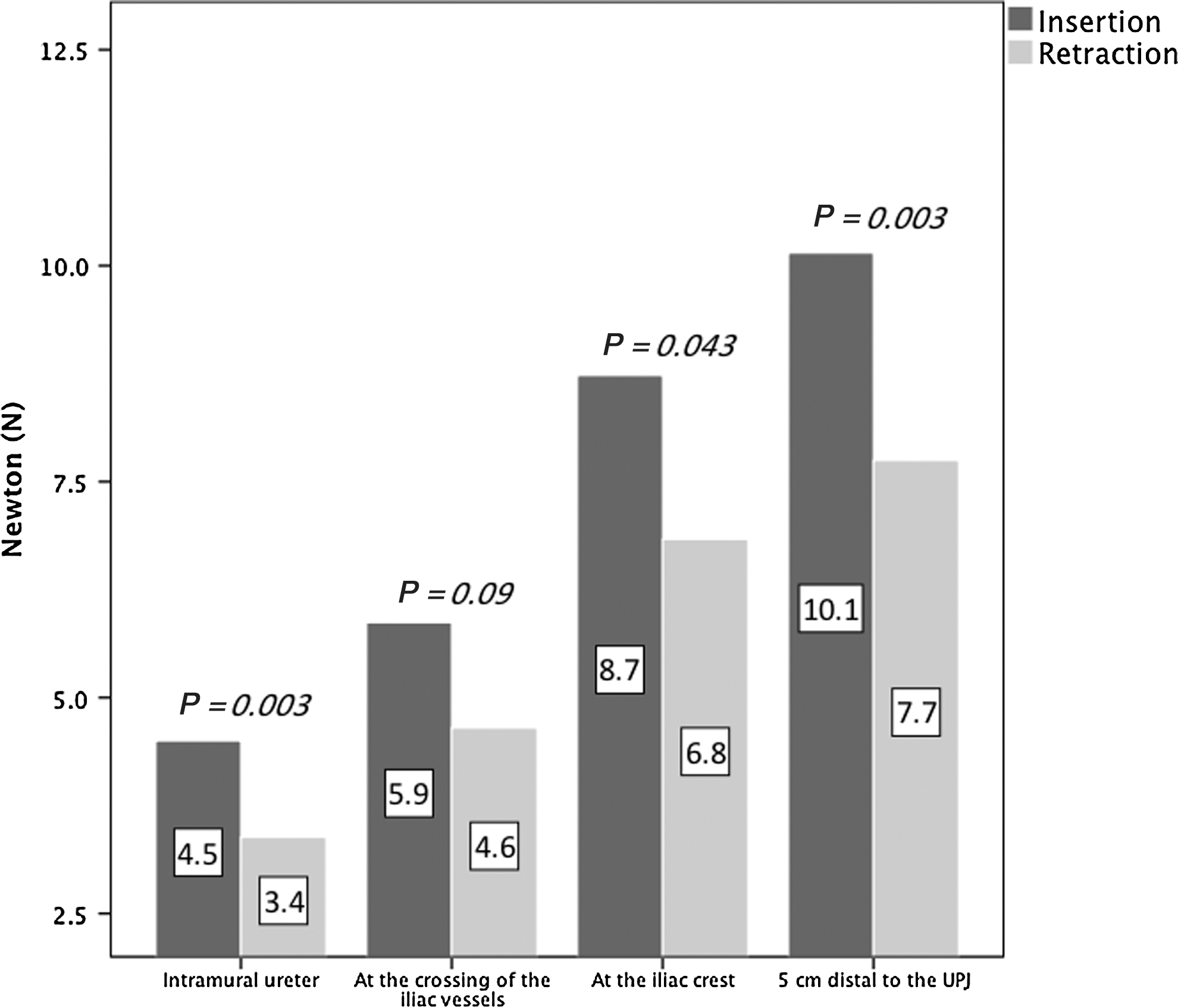
Comparison of the insertion and retraction forces of the ureteroscope at different localizations in the ureter. The P values refer to paired-samples t test comparing mean values of the insertion and retraction forces. UPJ=ureteropelvic junction.
There were no significant differences comparing the mean forces measured in the right and left ureter. As an example, the mean values for pushing forces in the lower ureter were 5.9±4.9 N and 4.0±3.2 N on the right and left side respectively, P=0.34.
The differences in the insertion and retraction forces of the ureteroscope between males and females are given in Table 2.
The forces are measured in Newton (N). Values are given as mean±standard deviation or standard deviation of the difference. P values refer to independent samples t test comparing the measurements of male and female patients.
Discussion
This study describes and evaluates the usefulness of a novel method for measuring the mechanical pushing and pulling forces exerted on a semirigid ureteroscope during insertion and retraction of the ureteroscope in clinical situations. The equipment for measuring the forces is commercially available except for the coupling device connecting the force meter to the ureteroscope. The connector was constructed at our institution. The extra equipment did not disturb the handling of the endoscope.
Two series of force measurements at four locations in the ureter were performed in approximately 20 minutes. Successful measurements were achieved from all the 20 patients, although some of the data were lost in three patients because of technical failures or failure to advance the ureteroscope into the correct position for the measurements in the upper ureter. It can be concluded that the pushing and pulling forces exerted on a semirigid ureteroscope can be measured during ureteroscopy in realistic clinical situations. Until now, this has been doubted. 1
The calculated ICC values for evaluation of the agreement of the repeated measurements ranged from 0.737 to 0.812. ICC values 0.7 to 0.8 indicate strong agreement between repeated measurements, proving the reproducibility of the results at all four locations.
There was no statistically significant difference between the first and second series of measurements except for the retraction forces measured just under the UPJ, which were significantly larger at the second series of measurements. A possible reason for this may be the edema that always develops in the ureteral wall during and after ureteral instrumentation. It seems likely that the edema will be most marked in the lower ureter because of the greater mechanical trauma from the thickest part of the shaft of the ureteroscope in the narrowest part of the ureter. Gradually the edema will give less space for the thickest part of the conical instrument, resulting in larger pulling forces needed for retraction at the second measurement until the thickest part is out of the ureter.
Because the first and second series of measurements were performed within a short time, most of the edema may have developed after the measurements were completed. This may at least partly explain why the edema did not have any measurable impact on the forces needed to move the ureteroscope at the time of the second series of measurements at the more distally locations in the ureter. It should be admitted, however, that to our knowledge, it is not known how fast the ureteral edema may develop after ureteral instrumentation, although it has been known for a long time that such edema may give rise to transient ureteral obstruction. 3 In addition, complete avulsion of the ureter close to the bladder wall 4 may be attributed to extensive edema in the lower ureter fastening the endoscope to this part of the ureter.
The forces needed to advance and retract the ureteroscope were considerably larger in the upper ureter than in the lower. It is conceivable that the resistance between the ureteral wall and the ureteroscope will increase as the area of contact between them becomes larger during the advancement of the instrument. In addition, the lateral pressure of the ureteroscope against the ureteral wall will increase as the semirigid instrument straightens out the normal curves of the ureter. The conical shape of the ureteroscope may contribute even more to increase the resistance against insertion and retraction. The impact of the conical shape and the caliber of the shaft should be further evaluated in a separate study by measuring the force profiles for endoscopes with a cylindrical shaft with various sizes.
Much of the resistance against advancement of the ureteroscope may be located at the intramural distal ureter where the luminal diameter is small 5 and the functional ureteral wall is reinforced by the bladder wall. The effect of balloon dilation of the ureteral orifice before inserting the ureteroscope 6 may be evaluated by measurements of the pushing and pulling forces.
Interestingly, the forces needed for retraction of the ureteroscope were significantly smaller than the forces needed for insertion at all levels of the ureter, except at the level of the iliac vessels. The insertion of the ureteroscope dilates the ureter and may thereby facilitate the subsequent retraction. The postulated dilation effect must, however, be short-lived, because the second insertion of the ureteroscope necessitated pushing forces of the same magnitude as at the first insertion. Edema in the ureteral wall might have developed gradually and within some minutes counteracted the dilatation effect of the ureteroscope.
The forces needed to move the ureteroscope were significantly higher in males than in females in the lower parts of the ureter. This is most likely because of the longer urethra in men and the prostate. In the upper ureter, however, no significant force differences were found, although there was a trend toward higher force values in the male patients. The lack of statistical significance may be because of the limited number of patients. It should, however, be emphasized that the study was not primarily designed to investigate the role of sex.
There was a substantial interpatient variation in the measured force values, and extremely small or large values were found in some patients. This may be caused partly by local anatomic conditions such as the luminal diameter of the ureter and variation in ureteral muscular tone, although such were not particularly noticed during the endoscopy. It is likely that using thinner endoscopes will reduce the interpatient force variation.
In a report of the complications during 2735 retrograde semirigid ureteroscopic procedures, Geavlete and associates 7 emphasized the importance of avoiding forced maneuvers with the ureteroscope to prevent traumatic lesions of the ureter. The highest pushing and pulling forces measured in the present study may have put some of the patients at risk, but no lesions were observed during the URS. We believe that no definite figure for safe limit of forces allowable during URS can be defined. Even small forces may cause ureteral damage, although it is likely that the risk of injury increases with increasing forces. Therefore, studies of how the pushing and pulling forces during URS can be reduced should be rewarding. Visualization of the aperture of the ureter and tactile feedback of the resistance will still be important factors to prevent traumatic lesions of the ureter.
Jung and colleagues 8 have shown in a randomized controlled study that adding the β-agonist isoproterenol (ISO) at low concentrations to the irrigating saline reduces renal pelvic pressure significantly during URS. The authors suggest that ISO may facilitate ureteral access efficiently by relaxing the ureteral muscular wall. A similar effect may be achieved by leaving a Double-J stent indwelling for a few days before URS. 9,10 The ureteral relaxation effect may be confirmed by studying the forces exerted on the ureteroscope.
Measurements of the pulling forces during retraction of various urethral catheters from the bladder have contributed to the development of catheters with very low friction. 11 Similar improvements may be achieved by testing the pushing and pulling forces on ureteroscopes with various surface characteristics. In addition, the effect of several other factors such as lubricating gel in the upper urinary tract, size and design of the ureteroscopes, and the technics used by various urologists may be evaluated by measuring the forces exerted on the endoscope.
A limitation of this study is that the force measurements have been performed with a conical shaped semirigid 8.5F ureteroscope only. The results may be different for other types of semirigid and flexible endoscopes. We see no reason that such endoscopes could not be tested by the method described in the present study. The coupling device between the force meter and the endoscope has to be modified to measure the forces on flexible instruments.
Conclusions
The described method is proved to be useful in a clinical setting for measuring the pushing and pulling forces exerted on a semirigid ureteroscope during URS. The results were reproducible in repeated measurements. A remarkable finding was the great interpatient variation in the measured force values, with extremely high values in some patients. The new method can be used in experiments studying how the forces exerted on the ureteroscope can be reduced to a minimum and thus contribute to making URS a safer procedure.
Footnotes
Acknowledgement
The connector was developed in collaboration with Rune Økland, Department of Medical Technology, Haukeland University Hospital.
Disclosure Statement
No competing financial interests exist.