
Abstract
Objectives:
To present the feasibility of laparoendoscopic single-site (LESS) nephron-sparing surgery (NSS) using new reusable umbilical single-port system and instruments.
Methods:
A prospective study was performed to evaluate operative data and patient outcomes after LESS-NSS with KeyPort®, a tri-channel single-port placed through a 2.5-cm umbilical incision, and specific DuoRotate® instruments. Patient characteristics, operative time, estimated blood loss (EBL), complications, visual analog pain scale (VAPS), and visual analogue wound satisfaction scale (VAWSS) scores were registered.
Results:
Six consecutive nonselected patients with indication of NSS and normal contralateral kidney were offered LESS-NSS. An accessory 3.5 mm port that facilitated renoraphy and unclamped technique was used in 4 (66.7%) cases each. Median tumor maximum size was 4.0 (1–7.5) cm; age 64 (31–76) years; body mass index 28.4 (22.1–39.3) kg/m2; operative time 233.5 (140–250) min; EBL 500 (200–500) mL; difference in hemoglobin 2.3 (0.1–4.6) g/dL. VAPS at day 2 was 0.7/10 and the median length of stay 3 (2–4) days. One case (16.7%) needed transfusion. None required conversion to standard laparoscopy or use of other additional ports. Postoperative complications occurred in 3 (50%) and major complications in 1 (16.7%). Incisions were totally hidden in the umbilicus. Pathology revealed angiomyolipoma (3), renal cell carcinoma (2), and chronic inflammation (1). Tumor margins were negative in all cases with malignancy. VAWSS at first month was 9.4 (8.1–10). At a median follow-up of 24 (10–32) weeks, no patient developed complications related to the approach.
Conclusions:
Umbilical LESS-NSS through a new single-port system of reusable nature, with or without the help of an accessory port and occasionally without clamping, can be effectively and very economically performed with minimum postoperative pain. Good candidates are patients with presumed benign renal masses that appreciate the cosmetic advantage of the approach.
Introduction
The kidney has become the organ of preference to investigate the advances of minimally invasive surgery and, particularly, laparoendoscopic single-site surgery (LESS), 4 which is the latest evolution of laparoscopy. LESS avoids multiple scars and diminishes port-related morbidity, thus minimizing patient discomfort and maximizing the cosmetic benefit of a small incision. 5,6 Therefore, it is not striking that LESS-NSS is being increasingly performed in recent years worldwide 7 and stands for 6%–34.5% of the procedures reported in large LESS series from individual institutions or collaborative groups, both laparoscopic and robotic. 7 –10
Despite the difficulty, laparoendoscopic single-site unclamped NSS has also been reported in highly selected patients with favorable tumor anatomic features and use of the harmonic scalpel or ligasure tissue sealing system. 11 –13 We describe our initial clinical experience with LESS partial nephrectomy using a novel umbilical single-port access device and Duo-rotate prebent instruments of reusable nature that diminish the need of additional trocars and also allow performance of unclamped surgery. Technique, results, and complications are described and data regarding historical control with laparoscopic partial nephrectomy (LPN) in our institution are provided for indirect comparison.
Materials and Methods
The KeyPort (Richard Wolf) was first experimented both in phantoms and in the porcine model following the regulations of the Autonomic Community of Madrid for animal care. Once 200 hours of training were individually achieved by two experienced surgeons with more than 300 previous laparoscopic procedures (PMC & FC), several low-risk human LESS surgeries (cryptorchidism, pyelolithectomy, and pyeloplasty) were performed before more complex retroperitoneal and pelvic surgeries were accomplished. Prospective data collection on the initial experience with this new system at our academic institution was stored since October 2011 to June 2012 in a patient-identified database in accordance with the institutional review board approval. The first NSS was performed with this system in January 2012.
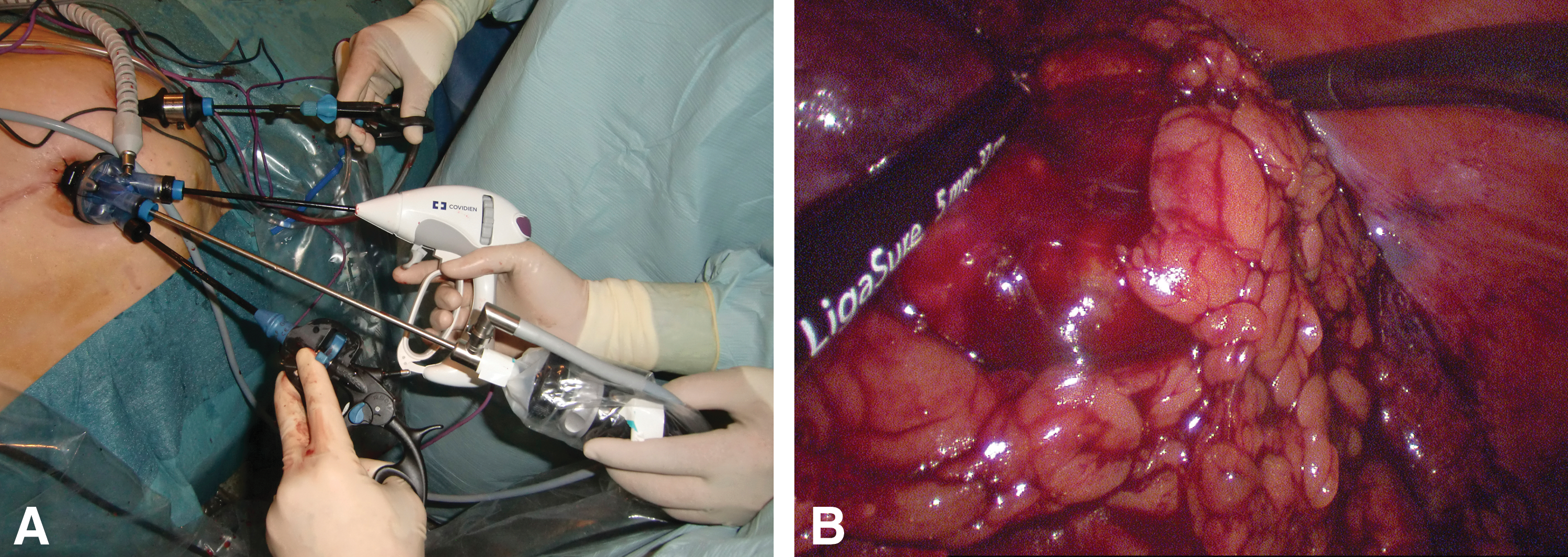
The patient was placed in the 45–60° modified flank position with the operating table minimally flexed. A reusable rigid trocar that fits a 2.5-cm umbilical opening without need of external or internal fixation was inserted in a screw-driven fashion (Fig. 1). The inner element was removed and the soft multichannel cover with three openings (5, 10, and 15 mm, respectively), was closed to insert curved instruments composed of inner sheath, outer element, and handle. Both KeyPort and inserts were entirely reusable. These elements incorporated a new Duo-rotate™ system (Richard Wolf) allowing precise 360° movement of the tips after alignment of the arms. A 5.3 mm wide, 45 cm long, 30° lens laparoscope and two operative curved instruments were used (mainly atraumatic prehension forceps and Metzenbaum scissors) in turns with a long suction reusable irrigation system and bipolar electrocautery (Richard Wolf), Force-triad (Covidien) (5 or 10 mm if desired) and Endopouch Retriever (Johnson & Johnson). Right-handed surgeons used the forceps grasper with the left hand (right side of the screen) and the scissors or Force-triad with the right hand (appears on the left) (Fig. 2).
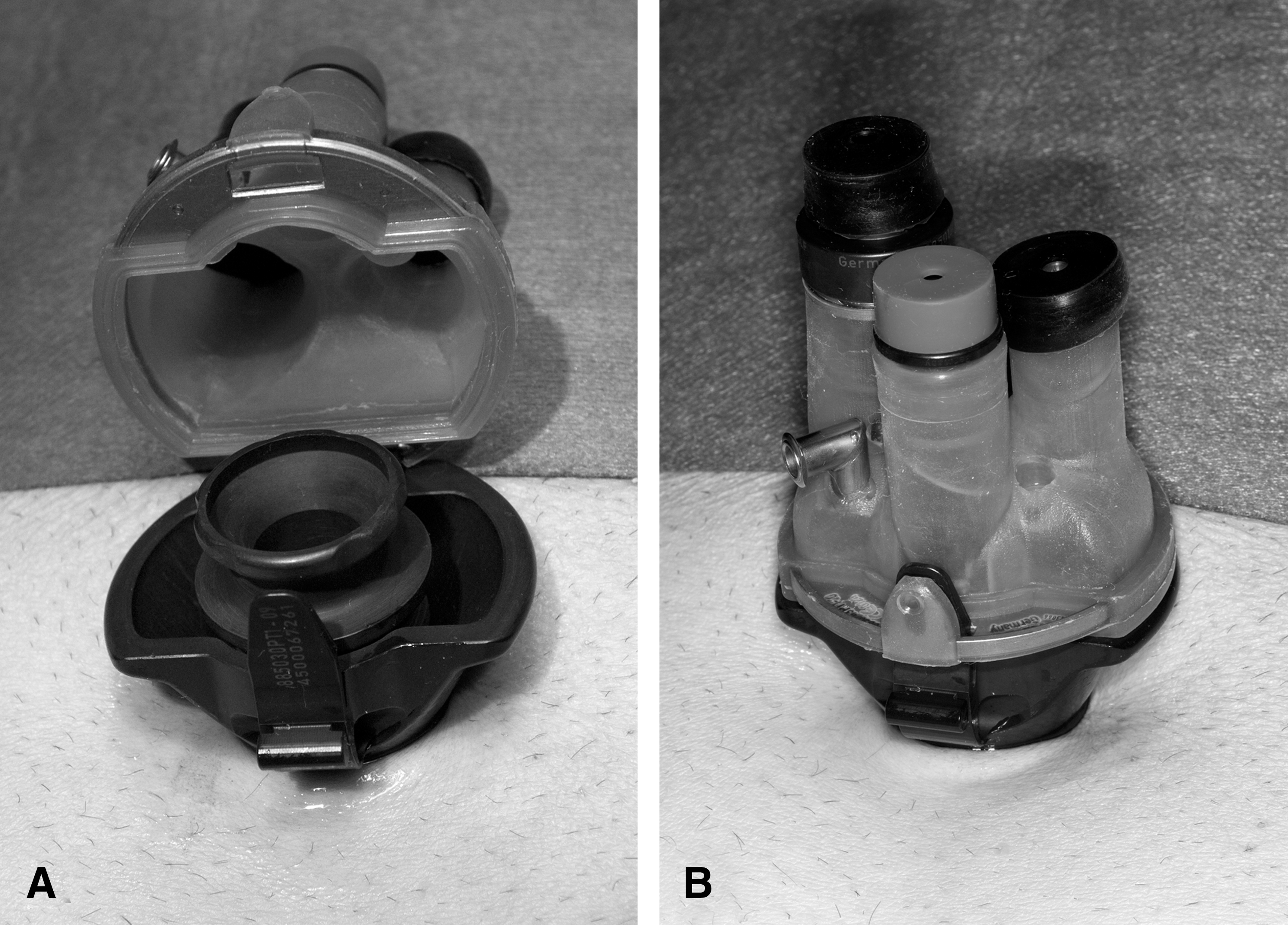
Reusable rigid trocar inserted in the umbilicus
External
Whenever a renal suture was planned, a 3.5-mm additional port was placed in the flank, or iliac fossa for lower pole tumors. Hepatic retraction was in a case facilitated with direct insertion of a needlescopic instrument. All the cases in these series were performed with one (or none) accessory port (Table 1). This access was used for suturing with a needle holder and also to extract the drainage far from the umbilicus to prevent hematoma formation or infection and also facilitated proper working angle and avoided clashing of the laparoscope with the instruments. The technique we describe can be interpreted as a hybrid LESS procedure (one or two port technique) with minimum accessory trocar dependence. The main surgeon used Duo-rotate instruments and applied Force-triad, Hem-o-lok or bulldog clamp with the right hand. The assistant held the camera and used the accessory port, if needed, to retract or aspirate.
BMI=body mass index; RCC=renal cell carcinoma.
The renal pedicle was prepared carefully in every case, even when unclamped. The lower pole was lifted by gentle traction to prepare the vessels. The renal vein and artery were identified and dissected. The tumor was localized and exposed. The renal artery first, and then the renal vein were clamped with separate bulldog clamps (Fig. 3). Excision under normal renal perfusion was performed in cases with favorable peripheral location, external growth, and presumed easy cleavage plane. The tumor size was not considered crucial to decide performing the unclamp technique.

Renal vein and artery are carefully dissected, even in unclamped technique
After excision of the neoplasm, parenchymal hemostasis was achieved by bipolar electrocautery, parenchymal stitches using a 0 polidiosanone violet monofilament synthetic absorbable bidirectional cut-in-two barbed suture Quill (Angiotech) tensioned by Hem-o-lok, and autologous fibrin sealant prepared with the Vivostat system and applied to the resection bed. The specimen was placed in an endoscopic bag and when used, the drain was extracted through the accessory port. Finally, KeyPort removal was followed by extraction of the pocketed specimen through the umbilicus.
Preoperative laboratory values 2 weeks before surgery and postoperative data on day 2 were registered. Renal functional outcomes as revealed by creatinine and eGFR were investigated at mo 1. The tumor size was assessed based on computerized tomography. Estimated blood loss, operative time, conversion to standard laparoscopy, intraoperative and postoperative complications, following Clavien-Dindo classification, hospital stay, and visual analog pain scale (VAPS) at day 2 from 0 to 10, were registered. Patient satisfaction in a visual analogue wound satisfaction scale (VAWSS) at 3–4 weeks from 0 to 10 was also investigated. This scale is provided by showing the patient the sketches of three different incisions (open incision in the form of lumbothomy, laparoscopy with five ports, and LESS with umbilical incision and one additional port) through which surgery could have been performed and immediately after asking him/her to define the scale he/she would give to his/her own incision in terms of satisfaction with the wound. 14 Patients were also specifically followed for evidence of local umbilical adverse events and for the cosmetic aspect of the wound, and patients with renal cell cancer were scheduled for long-term follow-up.
Results
Six patients (two male and four female) underwent transperitoneal LESS partial nephrectomy with KeyPort and Duo-rotate instruments (Table 1). The indication was solitary renal mass in 5 (3 of which were suspiciously malignant) and duplicated ectopic ureter with upper pole renal atrophy and recurrent urinary infection in another case. Patient characteristics were median age 64 years (range 31–76) and body mass index (BMI) 28.4 (22.1–39.3) kg/m2. Previous abdominal surgery had been performed in 50% of the cases. During the same time span, eight patients with RCC were intervened with umbilical LESS radical nephrectomy and four patients with urothelial malignancy and renal involvement received umbilical radical nephroureterectomy. Historical series of patients treated with LPN in our institution has already been presented. 15
Outcomes and complications
Unclamped KeyPort NSS was performed in 4 of 6 cases (66.7%) and warm ischemia time (WIT) in the remaining 2 was 27 and 28 minutes, respectively. Pathologic analysis revealed angiomyolipoma in 3 (preoperatively suspected in 2 of them for the presence of an adipose component), renal cell carcinoma (RCC) in 2 (chromophobe RCC and papillary RCC, respectively), and chronic inflammation in a case. The median tumor maximum size was 4 (1–7.5) cm. The largest lesions intervened were those with preoperative suspicion of angiomyolipoma (6.3 and 7.5 cm) (Fig. 4). Clamped NSS was performed in a RCC with R.E.N.A.L. nephrometry score 8 and in a epithelioid angiomyiolipoma (PEComa) with R.E.N.A.L. score 5 and profuse intraoperative bleeding (Table 1). Tumor margins in the patients with RCC and PEComa were negative.

Computerized tomography scan of patients with renal cell carcinoma
The ureteral catheter was placed intraoperatively for opening of the collecting system in two cases. Operative time was 233.5 (140–250) min, estimated blood loss 500 (200–500) mL, and difference of hemoglobin 2.25 (0.1–4.6) g/dL at day 2. Median length of hospital stay was 3 (2–4) days. VAPS at day 2 was 0.7 (0–2.7) of 10. Median creatinine and eGFR at mo 1 were 0.74 (0.49–1.02) mg/dL and 87.7 (71–110) mL/minute, respectively.
Postoperative complications presented in 50% of the cases and included 1-day stay in the intensive care unit due to difficulties for extubation (IVa), pulmonary embolism diagnosed 15 days after discharge requiring readmission (IId), and cecal dilatation (I). The last one was clinically insignificant. Preventive measurements (heparin, graduated compression stockings, pneumatic compression, and early mobilization) had been used in the 31-year-old female patient who developed pulmonary embolism, readmitted for increased temperature 2 weeks after hospital discharge. She recovered without sequel.
Transfusion was needed intraoperatively in 1 case (16.7%) due to severe hemorrhage (Table 1). No patient required conversion to standard laparoscopy or open surgery. The procedure was performed without additional ports in two cases (33.3%), only one additional 3.5-mm trocar was used in 4 (66.7%), and no case required 2 or more extra ports. Incision was always hidden in the umbilicus, and in some patients, the scar produced by the additional port was also invisible (Fig. 5). VAWSS within the first month was 9.4 (8.1–10). Median follow-up was 24 (10–32) weeks. No patient developed umbilical hernia or late complications related to the approach. In one case, umbilical hernia was present before surgery and was simultaneously corrected.

Postoperative aspect: invisible umbilical and subxyphoid scars
Discussion
Since the original description of LESS to perform nephrectomy through the umbilicus, 16 this procedure has evolved to be safely and efficiently practiced by an increasing number of groups. Partial nephrectomy or NSS is a very interesting LESS urological surgery, 5,6 but still remains one of the most challenging procedures to be performed through a single port with somewhat more than a hundred cases reported worldwide, consistently renal tumors of mean size between 2.1 and 3.2 cm. 6,8,10 –13,17,18 Discussion whether LESS-NSS can be generalized is beyond our scope, but studying the feasibility of this technique with the new instruments may be a step to diminish the technical limitations of existing instrumentation. 8
Robotic LESS-NSS was initially described with the scope and a 5-mm trocar placed through a multichannel port (Triport, Advanced Surgical Concepts) and a second 5-mm trocar through the same skin incision alongside. 11 A large series of robotic LESS-NSS has been recently described in Korea with a homemade single-port device established by inserting two 12-mm trocars and two 8-mm trocars through the fingers of a surgical glove. 6,10 Possibly, future more precise manual systems will contribute to further improve this new field of surgery at a more reasonable cost.
The reusable KeyPort system that incorporates prebent instruments with double rotation is one of these recent developments to be placed preferentially inside the umbilicus. This surgery implies high patient satisfaction because the scar is easily concealed within the navel and appears feasible both for radical prostatectomy, cystoprostatectomy, and a number of reconstructive procedures. 14,19 –21 We describe our initial experience with KeyPort NSS, with special emphasis on the viability of the unclamp modality. A partial nephrectomy can be considered one of the ideal surgeries to promote a pure umbilical approach, because the size and consistence of the specimen makes the extraction through the navel an excellent alternative with cosmetic benefit and prompt repair. 6,9,18 Of course, limitations of the technique are the teaching curve and also the limited access from an umbilical approach for large renal masses in the upper pole and the adrenal field.
It is obvious that concentrating the incisions on a unique site characteristic of LESS implies a diminished motion range and impairs visualization. Nevertheless, the KeyPort incorporates a conceptual change as individual instruments have moved to a combined dual system of arms that avoids both external clushing and internal crossing by a combination of the curved nature of the instruments and the articulated rotation of their duo-rotate tip allowing precise movements without rigidity loss. Besides, the reusable nature of both instruments and port makes this alternative especially attractive. Also, the additional use of needlescopic material can be very beneficial without any cosmetics impact and facilitates the most critical steps of the procedure. 22
Certainly, cosmesis is not the top priority when performing a complex surgical procedure like a partial nephrectomy. Other possible benefits of LESS for major surgery under study are diminished postoperative pain, decreased analgesic use, shortened convalescence, and performance of a more careful surgery that could imply less estimated blood loss and also decreased hospital stay. 5,23 Besides, from an economical perspective, it should be stressed that a reusable port access system and materials are clearly advantageous. 14,24 Of course, this early experience should be consolidated in the future by more robust studies.
A comparison with conventional LPN or robotic-assisted LPN is impossible because of the absence of prospective randomized studies. 25 Also, the series we present was not matched with a control group. However, historical data in our institution revealed 107.2 (50–185) minutes mean surgical time, 26.8 (18–40) mean BMI, and 3.1 (1.2–7)-cm mean tumor size. Besides, hilum clamping was almost routinely performed, with a WIT of 33 (0–70) minutes. The urinary tract was repaired in 53% of the cases. Intraoperative bleeding requiring transfusion occurred in 8.7%, and the transfusion rate during admission was 20%. Postoperative complications presented in 18.7% and 6.7% were Clavien III. No case was converted to open nephrectomy. Mean postoperative stay was 5 (3–29 days). The proportion of cases with benign histology was 16.6%. Local recurrence developed in 1.7% at 31 mo mean follow-up. 15
The umbilical approach allowed performance of the unclamped technique with an invisible scar in selected cases with longer operating time and shorter hospital stay. 15 When clamping was performed, WIT was not longer that in historical data. Transfusion rate was similar, but the complication rate appeared higher in LESS-NSS, although this may be due, in part, to good reporting of complications and also to the small numbers reported.
According to the standardized R.E.N.A.L. score system, 26 none of the consecutive cases we have intervened were of higher complexity. However, the mean tumor size in this series is higher than previous reports in the literature 6,8,10 –13,17,18 and morbidity associated to NSS is related to the size of the lesion. 27 Besides, if other preliminary series are studied in detail, significant complications can also be appreciated, including bleeding requiring transfusion 6,8,11 and sometimes conversion to laparoscopy 8,11,12 or open mini-incision, 6,10 pseudoaneurism requiring selective angioembolization, 17 cerebrovascular accident with hemiparesis, 12 pulmonary embolism 17 and bowel, ureter or renal vein injuries. 10 The reported transfusion rate is very variable and ranges between 0 and 78.6%. 6,8,11 –13,17,18
Whether umbilical LESS approach is advantageous to perform NSS in a patient with solitary renal mass compared to conventional laparoscopy remains to be proven. However, we confirm umbilical LESS partial nephrectomy using the KeyPort is feasible in a wide variety of clinical settings. It can be performed with very low postoperative pain, excellent satisfaction with the wound, no-clamping or nonprolonged regular WIT, and short hospital stay. Although it is not always possible to determine whether a solid renal mass is benign or not based on imaging studies, best candidates are in our opinion patients with benign renal masses needing surgery that appreciate the cosmetic advantage of the approach, especially large angiomyolipoma with good cleavage plane. This preliminary study does not allow reliable oncologic assessment, but appropriate tumor margins were achieved in patients with RCC and PEComa. As can be expected for an oncologic procedure of high complexity, umbilical LESS partial nephrectomy is not devoid of operative and postoperative complications that resemble those of laparoscopy 20 and are therefore linked more to the procedure than the approach. 28,29
Conclusion
Umbilical LPN through a single port developed by Richard Wolf (KeyPort) to be used with a 5.3 mm wide, 45 cm long, 30° lens laparoscope and two operative working curved instruments that incorporate a new system that allows precise 360° movement of the tips after alignment of the arms (Duo-rotate). Satisfactory operative parameters can be achieved, also with excellent cosmetic results and postoperative analgesia. In selected cases, the procedure can also be performed without clamping. The entire reusable nature of this device implies a very important economical advantage. This favorable early experience with the new device should be consolidated by more robust studies in the future.
Footnotes
Acknowledgments
The authors thank Mr. Jesús Arconada (Grupo Taper, Madrid), Mr. Stefan Gillé, Mr. Benjamin Seidenspinner, and Mr. Juergen Steinbeck (Richard Wolf GMBH, Knittlingen) for providing constant instrumental support and Mr. José Domínguez for photographic assistance.
Disclosure Statement
Authors (PMC, FC, AG, and JCA) have no commercial associations that might create a conflict of interest in connection with the submitted manuscript. JCA has received grants from Astellas and Pfizer and has given lectures for Astellas, Pfizer, and GSK. PMC, FC, and AG have nothing to disclose.