
Abstract
Purpose:
To compare the clinical outcomes of two-port laparoscopic donor nephrectomy (TPLDN) vs hand-assisted laparoscopic donor nephrectomy (HALDN).
Patients and Methods:
Between November 2010 and March 2012, 100 kidney donors scheduled for left nephrectomy were alternatively assigned to HALDN or TPLDN in a 1:1 fashion. All procedures were performed by the same laparoscopic surgeon. Demographic data and intraoperative and early postoperative data were collected prospectively and analyzed.
Results:
There was no difference in the operating time (133±12 vs 142±17 min, P=0.07), blood loss (55±46 vs 58±52 mL, P=0.84), complication rate (10% vs 12%, P=0.74), and length of hospital stay (3.8±0.8 vs 4.1±2.8 days, P=0.5) between the HALDN and TPLDN groups. The warm ischemia time was longer in the TPLDN group (2.2±0.7 vs 3.5±0.9 min, P<0.001). No statistically significant differences were found in the analgesic requirement and the visual analog pain scores. There was a trend toward quicker return to 100% recovery in the TPLDN group (60±46 vs 39±15 days, P=0.05). The TPLDN group had a significantly smaller surgical incision (8.2±0.6 vs 5.5±0.4 cm, P<0.001) and higher scar satisfaction score (7.8±1.5 vs 8.6±1.3, P=0.02) than the HALDN group. No differences were found in the recipient serum creatinine values or in the incidence of delayed graft function.
Conclusions:
In comparing TPLDN and HALDN, there was no significant difference in a majority of the operative and postoperative parameters. TPLDN might be associated with smaller surgical incision, improved cosmetic satisfaction, and equivalent recipient graft function.
Introduction
Recently, several institutions have reported their initial experience with LESS donor nephrectomy (LESS-DN), describing its feasibility and safety. 11 –18 Although results are promising, it is clear that the use of LESS in living kidney procurement offers a new set of challenges even to the experienced laparoscopic surgeon. Technical limitations, including a lack of triangulation, clashing of instruments both inside and outside the peritoneal cavity, and limited exposure, make it a technically challenging procedure.
In an attempt to overcome the aforementioned drawbacks of LESS, we developed a protocol for two-port laparoscopic donor nephrectomy (TPLDN). TPLDN is a novel modification that adds a single 12-mm port resulting in tiny scars, maintaining the basic laparoscopic principle of triangulation while not contributing to patient morbidity and not jeopardizing the cosmetic outcome. We present our early experience with TPLND and compare the outcomes with hand-assisted laparoscopic donor nephrectomy (HALDN).
Patients and Methods
Patient selection
Between November 2010 and March 2012, we prospectively recruited consecutive donors who were scheduled for left donor nephrectomy. Fifty donors had to be included in each arm to establish a significant mean scar satisfaction score difference of 1 with a standard deviation of 2, a power of 0.9, and an alpha of 0.05.
One hundred kidney donors were alternatively assigned to HALDN or TPLDN in a 1:1 fashion. All procedures in both groups were performed by the first author, who has experience in laparoscopic surgery. The Institutional Review Board of our hospital approved this study, and all the patients included in the study signed an informed consent.
All potential donors were evaluated by our multidisciplinary transplant team and met appropriate criteria for kidney donation. The preoperative evaluation for the donor consisted of taking a thorough history, a physical examination, assessing the serum creatinine level and performing intravenous urography and 99mTc-diethylenetriamine penta-acetic acid scan. Spiral CT with three-dimensional reconstruction was used to assess the renal parenchyma and vasculature.
Surgical procedures
All procedures in both groups were performed with the patient in a 45-degree flank position for transperitoneal surgery. Patients undergoing HALDN had a supraumbilical midline incision placed for the hand port, and a GelPort (Applied Medical, Rancho Santa Margarita, CA) was fitted through the incision. Two additional ports (11-mm port for the camera; 12-mm port for the operating instrument) were then created (Fig. 1A). For TPLDN procedures, a SILS-Port (Covidien, Norwalk, CT) was placed through an umbilical incision. Two 5-mm trocars were placed within the SILS-Port (one for the camera, another for the operating instrument).
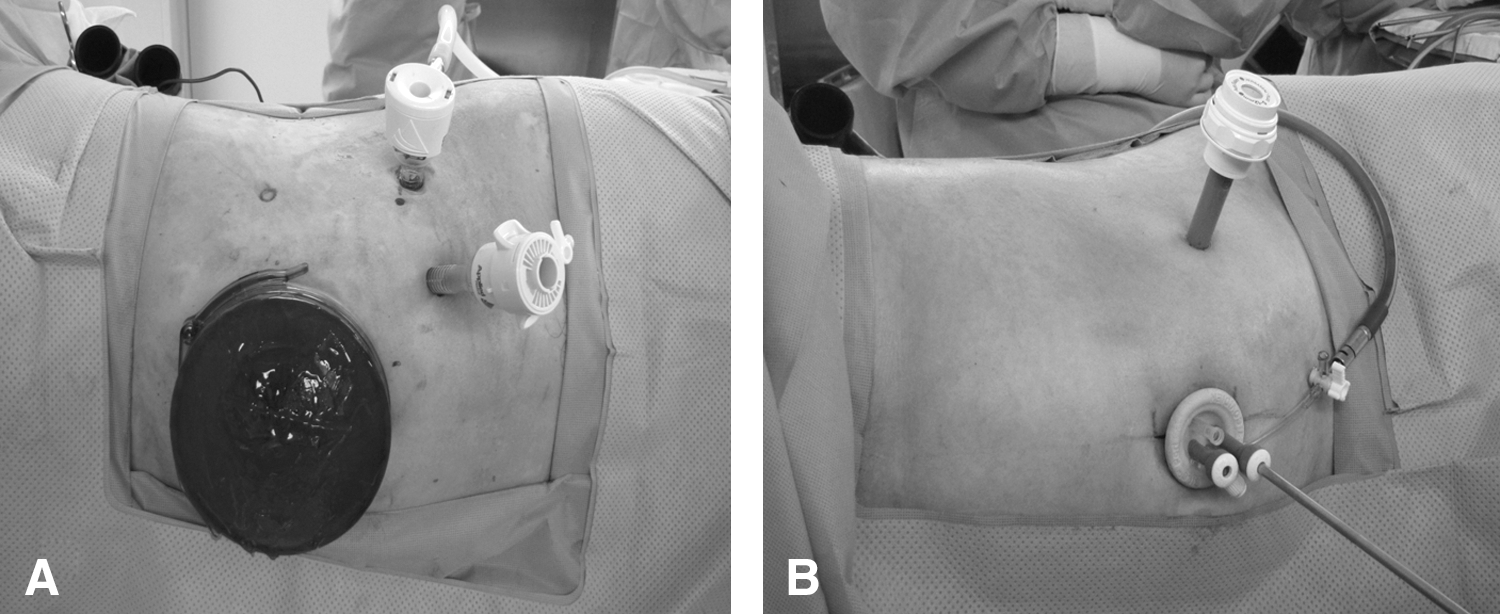
Port configuration in hand-assisted laparoscopic donor nephrectomy
After establishing pneumoperitoneum, a 12-mm trocar, for another operating channel, was inserted along the midclavicular line at the level of the umbilicus (Fig. 1B). During TPLDN procedures, conventional laparoscopic instruments were used, and no articulating or specialized laparoscopic instruments were needed. A standard 10-mm telescope was used in HALDN, whereas a 5-mm, 30-degree rigid telescope was used in TPLDN. In TPLDN procedures, two temporary sutures were used to provide traction to the kidney and to adjacent organs.
After port insertion, the surgical steps were similar in both groups. After dividing the renal vessels, the freed graft was retrieved by hand in the HALDN group. The graft was preplaced in a Lap bag (Sejong Medical, Seoul, Korea) before ligation of the renal hilum and after securing and dividing the vessels, it was extracted via the extended umbilical incision in the TPLDL group. The detailed surgical technique has been reported previously. 19
Operating time, warm ischemia time (WIT), estimated blood loss (EBL), complications, hospital stay, postoperative patient pain score, analgesia requirements, incision length, subjective scar satisfaction, convalescence data, and recipient allograft function were the main perioperative parameters evaluated to compare HALDN and TPLDN.
The visual analog scale (VAS) and the need for analgesic medications during postoperative care were used to evaluate postoperative pain. An independent physician assessed the pain score by using an analog pain scale (1 to 10) after the operation. A questionnaire was administered at 3 months postoperation to assess the surgical scar satisfaction score (0, unsatisfied; 10, very satisfied) and recovery time parameters. The assessment was made by an independent nursing staff whose members also did not know the type of surgery that the patient underwent.
Postoperative complications were recorded and graded using the modified Clavien system. 20 Allograft outcomes, including the incidence of delayed graft function defined as the need for hemodialysis posttransplantation, recipient creatinine at 1 week, 1 month, 3 months, and 6 months postoperation, were also analyzed.
Statistical analysis
Data were presented as mean and standard deviation or as frequency and percentage for continuous and categorical variables, respectively. We used the chi-square test and Student t test to compare categorical and continuous variables, respectively. Statistically significant result was defined as P<0.05. All statistical calculations were performed using SPSS 15.0 software.
Results
The demographic data were comparable in both groups (Table 1). There was no difference in the EBL, transfusion rates, arterial vascular complexity, and length of hospital stay between the two groups (Table 2). Although the mean operating time did not differ between groups, WIT was longer in the TPLDN group (2.2±0.7 vs 3.5±0.9 minutes, P<0.001). The mean incision length was shorter in the TPLDN group (8.2±0.6 vs 5.5±0.4 cm, P<0.001).
HALDN=hand-assisted laparoscopic donor nephrectomy; TPLDN=two-port laparoscopic donor nephrectomy.
HALDN=hand-assisted laparoscopic donor nephrectomy; TPLDN=two-port laparoscopic donor nephrectomy; VAS=visual analog pain score; POD=postoperative day.
One case in the TPLDN group was converted to HALDN because of renal vein injury, which limited hilar dissection. Two patients in the TPLDN group needed insertion of an accessory 5-mm port. The accessory port was inserted during the steps of upper pole separation and of renal pedicle dissection, respectively.
The mean VAS pain score at discharge from the hospital and the length of hospital stay were not significantly different between the groups (Table 2). Also, there was no difference in terms of analgesia requirement among the two groups. Postoperative convalescence parameters were similar between groups with respect to the time to return to normal activities (Table 2). Although not statistically significant, there was a trend toward quicker return to 100% recovery in the TPLDN group (P=0.05). In regard to cosmetic outcomes, the surgical scar satisfaction score was significantly higher in the TPLDN group compared with the HALDN group (7.8±1.5 vs 8.6±1.3, P=0.02).
There was no statistically significant difference in the overall complication rate between the two groups (Table 3). In the HALDN group, there were five complications, including one intraoperatively and four postoperatively. During the creation of the hand port, a serosal bowel injury developed in one patient; it was repaired with a simple serosal suture. All postoperative complications were minor (Clavien grade I–II). One patient was readmitted with postoperative ileus, and the condition was managed conservatively.
HALDN=hand-assisted laparoscopic donor nephrectomy; TPLDN=two-port laparoscopic donor nephrectomy.
In the TPLDN group, there were six complications, including two intraoperatively and four postoperatively. One case was converted to hand-assisted laparoscopy because of renal vein injury. One graft had accidentally cut one of the small upper polar arteries, which resulted in ischemia to less than 5% of the renal parenchyma, but has since been maintained in good condition. The four postoperative complications included wound infection in one patient, necessitating only regular wound dressings, and chylous ascites in three patients, which resolved after dietary measures or therapy by total parenteral nutrition.
The recipient graft outcomes are listed in Table 4. Allograft function was comparable between the groups. No patient in either group experienced delayed graft function. Mean recipient serum creatinine levels at postoperative week 1 and at postoperative 1, 3, and 6 months were similar between the groups.
HALDN=hand-assisted laparoscopic donor nephrectomy; TPLDN=two-port laparoscopic donor nephrectomy; Cr=creatinine.
Discussion
In the last two decades, LDN has become the procedure of choice for harvesting kidneys. The potential minimal invasiveness and improved cosmetic effect without compromising outcomes of the recipient graft function have contributed to the general acceptance of this technique. 2 –6 LESS is a recent innovation of which the potential benefits include superior cosmesis, decreased pain and morbidity, and improved convalescence. LESS has gained great interest for kidney procurement. Gill and associates 11 first demonstrated the feasibility of LESS for donor nephrectomy in their initial report of four cases. The author reported a median operative duration of 3.3 hours, a median WIT of 6.2 minutes, and no intraoperative complications.
LESS-DN is certainly comparable or even preferable to conventional laparoscopic nephrectomy with respect to the subjective cosmetic results and to the objective surgical results. 13 –16 Technical limitations, however, including lack of triangulation and clashing of instruments, make it a technically challenging procedure. A limited number of access ports, as in the case of LESS-DN, may impair the surgeon's ability to achieve adequate retraction and dissection. Therefore, the use of an additional port is sometimes necessary. 13,14,17 Canes and colleagues 13 and Kurien and coworkers 14 each presented their results of LESS-DN. They used a 2-mm and a 3-mm port in all cases, respectively. Similarly, in 11 of their cases, Ganpule and colleagues 17 used either a 3- or 5-mm port for retraction.
Although the graft outcomes in recipients are comparable, several studies have shown that LESS-DN is associated with longer WIT. 13,17 In a series of 50 cases, Kurien and associates 14 reported that LESS-DN had a longer WIT compared with standard laparoscopic donor nephrectomy (7.15 vs 5.11 min). Ganpule and coworkers 17 noted a mean WIT of 6.79 minutes. In addition, several series have reported LESS-DN to be related to serious complications, including graft loss. 11 –13,21
Donor nephrectomy is unique in that the procedure affects an altruistic, completely healthy person. The safety of the donor and the retrieval of the graft in perfect condition are of utmost concern to the donor and the recipient. Therefore, each surgeon must use the technique with which he or she feels most comfortable. Considering the aforementioned drawbacks of LESS-DN, we decided to use an additional 12-mm port. In fact, it could be enough to add either a 3- or 5-mm additional port instead of 12 mm to overcome the technical limitations of LESS, but we believe using a 12-mm port at the midclavicular line facilitates faster operation with availability of larger instruments. Clipping and application of a stapler is much easier with the use of a 12-mm port at the midclavicular line.
To our knowledge, the present study is the first to demonstrate the advantages of TPLDN compared with traditional laparoscopic surgery. Because HALDN has become the standard technique for kidney procurement in our institution since 2000, TPLDN was compared with HALDN. We started our TPLDN program knowing that the first author has performed more than 100 conventional LDN operations.
In the TPLDN group, we aimed to appropriately perform nephrectomies with the minimally invasive approach and to overcome the technical limitations of LESS at the same time. The addition of a 12-mm port could make the surgery easier and more rapidly performed by restoring instrument triangulation and by providing an increased range of motion. Good exposure of the renal hilum is also very important when performing donor nephrectomy. In the TPLDN group, we developed a simple retraction technique with 3-0 polypropylene suture. 19 This technique was safely performed in all of our patients. This compensates for the lack of a port for retraction and eliminates any skin scarring at that site.
In this study, the demographic data and vascular complexity were similar between the two groups. We did not detect any significant differences in terms of operating time, WIT, EBL, pain score, postoperative analgesia requirement, or donor's length of hospital stay. While the overall complication rate was similar between the groups, there was one conversion to HALDN in the TPLDN cohort but no procedural conversions in the HALDN group. In the comparison of the first and second half of patients in the TPLDN group, there were no differences detected in operating time (144 vs 140 min, P=0.37). A learning curve virtually did not exist in TPLDN. These results suggest that the TPLDN technique was not difficult to master and could be safely performed by surgeons who have only modest experience with advanced laparoscopic surgical procedures.
Although the WIT was clearly longer in the TPLDN group, it was within an acceptable range and was comparable to conventional laparoscopy as reported in published data. 5 In terms of convalescence, there was a trend toward faster convalescence in the TPLDN group. The time to 100% recovery was sooner in the TPLDN group, although this was not statistically significant. The TPLDN group was characterized by shorter average incision lengths. In addition, when rating their overall surgical scar satisfaction, the TPLDN group gave significantly greater mean ratings than did the HALDN cohort. Most importantly, the recipient allograft outcomes on follow-up at postoperative week 1 and at postoperative 1, 3, and 6 months were equivalent between the two groups of patients.
There are some limitations in our study. This study was conducted at a single institution with a small sample size in each group. The learning curve of these two procedures is different. For TPLDN, it represents the surgeon's initial learning curve, compared with a more experienced starting point on the learning curve for HALDN. Moreover, a longer period of follow-up is necessary to evaluate the long-term complications and overall recipient outcomes. One of the underlying limitations of most studies comparing patient self-assessed cosmetic satisfaction with different surgical procedures is that the patients were only given the opportunity to rate the cosmetic benefit of their own abdominal scars. Especially, it is important to note that patients were not blinded to the procedure, which may have affected their perception of scars. Nevertheless, the strengths of the current study are that all procedures were performed by a single surgeon and that this study was prospectively designed with alternating assingnment with a 1:1 allocation ratio.
In this study, we showed that TPLDN is a feasible technique without notable differences when compared with conventional LDN, but it does have a higher degree of wound satisfaction. We believe that this minimally invasive technique appears to be a good compromise between a pure LESS procedure and a standard multitrocar laparoscopic approach.
Conclusions
We demonstrated that TPLDN, using single multichannel and 12-mm ancillary ports, is safe and has similar clinical outcomes as HALDN. Our early experience suggests a definitive cosmetic advantage, trend toward faster complete convalescence, and equivalent recipient graft function for TPLDN. TPLDN may be a viable alternative in the field of minimally invasive donor nephrectomy.
Footnotes
Disclosure Statement
No competing financial interests exist.