
Abstract
Purpose:
To report the clinical efficacy and intermediate-term functional outcome after laparoscopic anatrophic nephrolithotomy (LAN) as an alternative treatment modality for complete staghorn renal stone.
Patients and Methods:
The demographic and perioperative parameters as well as the intermediate outcome of 10 adults (9 men) who underwent transperitoneal LAN for complete staghorn renal stone were analyzed. Functional imaging studies consisted of intravenous urography (IVU) and technetium-99 dimercaptosuccinic acid scintigraphy (99Tc-DMSA) renal scan done before the operation and at the last follow-up visit.
Results:
Mean age of patients was 48.7 years (range 37–64 years). Mean stone size was 67.3 mm (50–90 mm). Mean operative time was 192 minutes (110–240 min), and mean warm ischemia time was 32.8 minutes (15–40 min). A few hours after laparoscopy, one patient underwent splenectomy because of significant hemorrhage from a splenic laceration (grade IIIb complication). During the follow-up period early after the operation, we detected an 8-mm lower caliceal stone and a 25-mm midcaliceal stone in one patient each (stone-free rate: 80%). After a mean follow-up of 11.9 months (6–19 mos), 85.5% of corresponding renal unit function was preserved; however, there was a significant mean decrease in 99Tc-DMSA uptake from 48.4%±8.83 before surgery to 41.4%±13.98 afterward (−7%±6.53; P=0.008). Nevertheless, renal units were completely functional at follow-up IVU with a significant improvement in obstruction in all patients.
Conclusion:
LAN is an alternative minimally invasive approach for one-session management of patients with complete staghorn renal stone. It offers an acceptable rate of stone clearance and operative complications but does incur a minimal loss of function in the affected kidney.
Introduction
In the past 2 decades. percutaneous nephrolithotomy (PCNL) and shockwave lithotripsy (SWL) revolutionized the treatment strategies for renal stones. Their minimally invasive nature and high stone-free rate reduced the use of open stone surgery (OSS) dramatically. 2 Unfortunately, not only because of a high stone burden, but for the morphometry of complete staghorn renal stones, the application of PCNL±SWL for their management may be suboptimal. 3
A global study recruiting more than 5300 patients who underwent PCNL conducted by the Clinical Research Office of the Endourological Society found that the stone-free rates were lower (59.9% vs 82.5%) and operation time, rate of complications, and hospital stay were significantly higher for staghorn renal stones than for nonstaghorn stones. 4
Because open anatrophic nephrolithotomy (AN), in contrast to PCNL, is not influenced by stone morphometry, many centers reserve it as a still appreciable procedure in patients with complete staghorn renal stones. 1,2,5
Performing AN for complete staghorn renal stone in a minimally invasive milieu of laparoscopy was recently introduced with acceptable early postoperative outcomes in small sample sizes. 6 –8 Despite promising early postoperative outcome of laparoscopic anatrophic nephrolithotomy (LAN), little is known about the impact of this procedure on the ultimate renal function during an intermediate or long-term follow-up period. This could be an important concern, because during LAN, the kidney is exposed to warm ischemia.
In the present study, we reported our experience with LAN as a new treatment modality for complete staghorn renal stone. We specifically focused on the clinical efficacy of this procedure as well as the outcome of renal function after an intermediate-term follow-up period.
Patients and Methods
Ethics
Approval was obtained from our Institutional Review Board, and informed consent was obtained from all patients. The benefits and risks of the laparoscopic approach with the possible need for open conversion were explained before the operation.
Patients
From March 2010 to December 2011, 10 adult patients with complete staghorn renal stones were candidates for LAN. The patients had no history of any abdominal surgery, including ipsilateral renal surgery. They also had no history of previous SWL.
Preoperative imaging studies consisted of abdominopelvic ultrasonography (US) and intravenous urography (IVU) to delineate the renal anatomy and stone size (largest diameter). The function of the target kidney was documented by technetium-99 dimercaptosuccinic acid (99Tc-DMSA) scintigraphy renal scan before the operation and was measured again at the last follow-up visit. The patients were admitted 1 day before the surgery and received a light bowel preparation and intravenous ceftriaxon. It was ensured that the urine was sterile before the operation. All procedures were performed by one surgeon (A.A).
Surgical technique
With the patient in the flank position, supported by adequate padding, four-port transperitoneal laparoscopy was performed. A 10-mm umbilical camera port as well as two 5-mm working ports were placed on the midclavicular line, subcostally, and midway between the umbilicus and anterior superior iliac spine, as well as a 10-mm port lateral to the rectus muscle at the umbilical level.
After incising the white line of Toldt and medial mobilization of the colon, the renal pedicle was exposed. Then the renal artery and vein were fully dissected, the Gerota fascia was opened, and the kidney was completely mobilized. The renal artery was temporarily clamped with a bulldog clamp (Aesculap, Tuttlingen, Germany) or with a laparoscopic Satinsky instrument (Fig. 1A). At 30 minutes before renal artery clamping, a dose of mannitol (12.5 g) was infused, which was repeated after release of the clamp. Through a sharp incision over the Brodel line, the renal parenchyma and collecting system were opened, the staghorn stone was mobilized and retrieved en-masse (Fig. 1B). The collecting system was explored for any caliceal stones, irrigated, and then was closed together with parenchymal tissue with two rows of polyglactin 2-0 running sutures. The stitches were reinforced by applying Hem-o-lok clips (Weck closure systems, Research Triangle Park, NC) (Fig. 1C). The renal artery clamp was then released, the renal perfusion was observed, and the site of nephrotomy was checked for any hemorrhage. After closing the Gerota fascia, the stone was extracted from the site of the 10-mm trocar, a Penrose drain was placed in the retroperitoneum, and the trocar sites were closed (Fig. 1D).
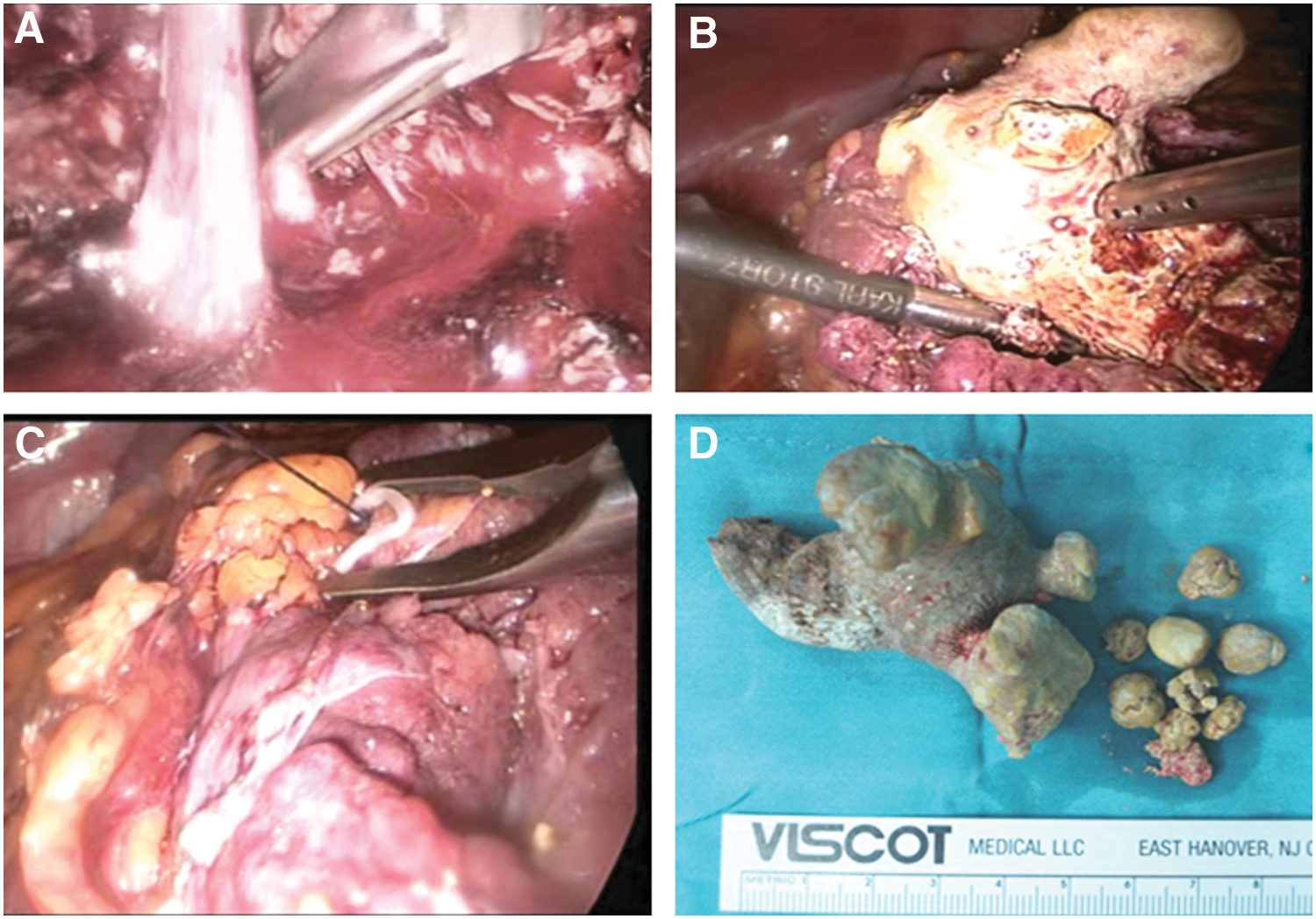
After complete dissection of the renal pedicle, the renal artery was temporary clamped by a bulldog clamp
Study outcome
The demographic data of all patients including stone size as well as the intraoperative data such as operative time and warm ischemia time (WIT) were recorded. Major postoperative complications (higher than grade 1 according to the Clavien classification 9 ), hospital stay, preoperative and 6-hour postoperative hematocrit and serum creatinine levels were also recorded. Any residual stones were detected by taking plain films and a thorough abdominopelvic US 1 month after discharge. The function of the target kidney and its collecting system anatomy were determined by IVU and 99Tc-DMSA renal scan performed at the last follow-up visit. The t, analysis of variance, and linear regression tests and SPSS® version 15.0 software were used for data analyses.
Results
The mean age of patients was 48.7 years (37–64 years); nine of them were men. Mean body mass index was 25.1 kg/m2. Mean stone size (largest dimension) was 67.3 mm (50–90 mm), and all were opaque or semiopaque complete staghorn renal stones. Table 1 summarizes the demographics as well as the intraoperative, early postoperative, and intermediate-term outcome of the patients. Mean operative time was 192 minutes (110–240 min), and mean WIT was 32.8 minutes (15–40 min). No blood transfusions were needed in any patient, but in patient #2, because of ongoing blood loss via the site of the Penrose drain, one bag of packed cells was transfused a few hours after laparoscopy before exploratory surgery. This patient underwent splenectomy because of a significant hemorrhage from a splenic laceration that could not be repaired. Other patients had an uneventful laparoscopy. No urine leakage was detected in any patients, and no ureteral stent placement was needed.
The largest dimension.
WIT=warm ischemia time.
Mean hematocrit drop 6 hours after the surgery was 4.2 (from 42.1 before to 37.9 after the operation), and mean hospital stay was 3.5 days (2–6 days). On the discharge day, we detected an 8-mm lower caliceal stone and a 25-mm midcaliceal stone in two patients (#2 and #3). They were treated with one successful session of SWL and PCNL, respectively, 6 to 8 months after their LAN. Mean residual stone burden was 3.3 mm (0–25 mm), and the stone-free rate was 80%. On average, 95.1% of stone burden was cleared by LAN.
After a mean follow-up of 11.9 months (6–19 mos), the target renal function improved in two and dropped in eight patients. Although during this period 85.5% of corresponding renal unit function had been preserved, there was a significant mean decrease in 99Tc-DMSA uptake from 48.4%±8.83 before surgery to 41.4%±13.98 afterward (−7%±6.53; P=0.008). This is despite renal units being completely functional at the follow-up IVU, with a significant improvement in obstruction in all patients (Figs. 2A, 2B). There was no correlation between the mean WIT and mean stone size and between these two parameters with postoperative renal function.
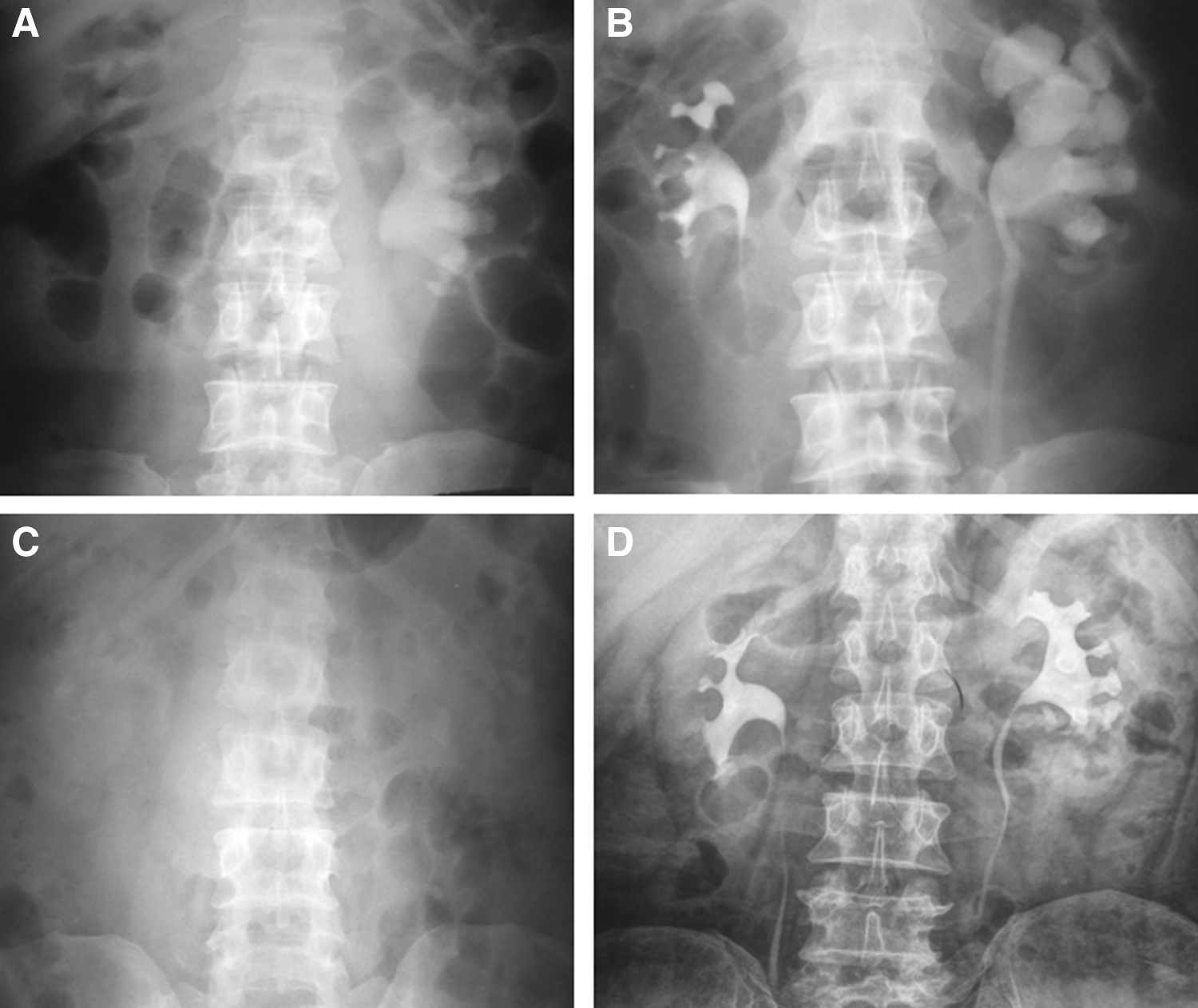
Preoperative plain radiography and intravenous urography (IVU)
Discussion
Despite tremendous improvements in endourologic procedures, management of complete staghorn renal stones remains challenging. Staghorn renal stone is a potential threat not only for the renal function, but it can also cause septic complications. Because of a high rate of recurrence, especially if associated with infection, the ultimate end point of their management should be complete clearance. 10 For complete staghorn renal stones, this is difficult to achieve, even after multiple sessions of endourologic procedures and SWL.
Mishra and associates 3 proposed a morphometric measurement tool for prediction of the success rate of one-session PCNL in those with staghorn renal stones. They showed that in those with complex, large burden staghorn stones, multiple tracts and multisessions of PCNL would be needed.
Desai and colleagues 11 showed the efficacy of “multiperc” PCNL for management of staghorn renal stones in 773 patients over a period of 17 years. They concluded that this procedure needs extensive experience and training. Although their stone-free rate after multisessions of interventions improved with time from 81% to 93%, complete clearance in one-session PCNL remained a challenge.
Akman and coworkers 12 addressed the long-term outcome of PCNL for staghorn renal stones in terms of renal function and stone recurrence rate. After a mean follow-up period of 37.3 months, they found that in about 80% of patients, the chronic kidney disease stage improved or remained stable and the immediate postoperative glomerular filtration rate was the most important predictor of renal function. Their stone-free rate after one session of PCNL was 76.5% with a stone recurrence or stone growth rate of 31.2% to 63.2%.
Although the rate of major complications including the need for large amounts of transfused blood after PCNL for staghorn renal stones could be as high as 18% to 27%, 1,13,14 the impact of both multiple tracts and single tract PCNL on the function of the corresponding renal unit seems promising. Of these kidneys, 84% to 100% showed stable or improved radionuclide uptake. 14 –16
Despite the fact that multiple access tracts may not pose a significant detrimental effect on renal function and help to improve the stone-free rate, a considerably higher rate of major complications would be expected in comparison with single tract PCNL (28.4% vs 13.9%). 17
Although the 2005 American Urological Association guidelines on the Management of Staghorn Calculi do not recommend AN as the first-line treatment for staghorn calculi, because of shortcomings of PCNL, many investigators consider OSS for management of complete staghorn renal stone as a reasonable alternative. 1,2,5 Several series have shown the superiority of one-session AN in terms of stone-free rate (80%–100%). 1,2,18 Some functional loss (7%–27%) after open AN, however, has been reported, which was considered clinically insignificant. 5,19,20 Improvements in renal function have also been observed because of the relief of obstruction after AN. Ramakrishnan and associates 21 recommended open AN as a valuable treatment option for those with complete staghorn renal stone with a stone-free rate of 85% on discharge day and renal function preservation rate of 87% 6 months after the operation. Esen and coworkers 18 compared the stone-free rate of open AN with combined PCNL+SWL for staghorn renal stones that was in favor of OSS (80% vs 50%). In a randomized clinical trial, Al-Kohlany and colleagues 22 compared the outcome of PCNL vs OSS for management of complete staghorn renal stone. Based on the stone complexity, they used single tract single session to multiaccess multisession PCNL procedures. Comparable outcome in terms of stone-free rate (49% for PCNL vs 66% for OSS) and preservation of the renal function (91% for PCNL vs 86.7% for OSS) were achieved. Obviously, those with PCNL had a smooth convalescence with an earlier recovery.
After Deger and associates 23 reported the first clinical case of LAN for a staghorn renal stone, three clinical series recruiting 24 patients 6 –8 showed the feasibility of this minimally invasive procedure. LAN duplicates the open AN but is performed in a minimally invasive milieu avoiding large flank incisions as a cause of significant postoperative morbidity. 1 As shown in Table 2, the perioperative outcome of our series is comparable to that of the previous reports.
WIT=warm ischemia time.
In the present study, we showed the intermediate-term outcome of LAN after a mean follow-up period of 11.9 months. We found that a mean function loss of 7% might occur in the affected kidney, which is comparable to open AN. 5,19 –22 This is also true for the stone-free rate of LAN. 1,2,18,21,22 Although LAN is a more invasive procedure than PCNL, the stone-free rate after one session of LAN seems to be higher than after one session of PCNL for patients with complete staghorn renal stones, and also the incidence of perioperative complications and the need for blood transfusion may be lower in centers with enough laparoscopic experience. The use of intraoperative laparoscopic US would be helpful to find any residual fragments.
Laparoscopic experience is also crucial with regard to keeping WIT in an acceptable range. Our mean WIT was 32.8 minutes, and we found no correlation between WIT and postoperative renal function status. We think that if these patients with such complex stone morphology had undergone endourologic procedures, frequent interventions would have been needed and probably a lower rate of stone clearance might have been achieved. Multiple procedures might result in significant morbidity and an overall higher treatment cost. On the other hand, warm ischemia remains a great concern in this procedure. Data from partial nephrectomy studies have demonstrated that every minute counts, and for each minute of warm ischemia, there is an increased risk of acute renal failure and long-term chronic kidney disease. 24 We used two rows of running sutures for closure of the renal parenchyma, others have shown that one layer closure, in favor of WIT, would be sufficient in this setting. 6 –8
Some limitations of this study, however, deserve mention. Our sample size was admittedly small. This was a result of our selection criteria to only enroll patients into the study with a giant staghorn renal stone without previous history of any interventions. Obviously, enrolling more patients would enhance the power of the study. We do not currently know the clinical significance of a mean 7% loss in function in the affected kidney in the long term. Although the function loss after LAN seems to be inconsistent with open AN, it would probably be higher than what may occur after a “complex” PCNL. A three-arm comparative study (LAN vs open AN vs PCNL) may provide answers to this issue. Although laparoscopy has a limited role in the urologists' armamentarium for stone management, LAN is a potential alternative to OSS for management of complete staghorn renal stones. Nonetheless, this is a demanding procedure and needs extensive laparoscopic experience.
Conclusion
In centers with enough laparoscopic experience, LAN is a feasible and promising alternative minimally invasive approach for one-session management of patients with complete staghorn renal stone. It offers acceptable rates of stone clearance and operative complications but has a minimal loss of function in the affected kidney during an intermediate-term follow-up period. Long-term significance of this functional loss is yet to be determined.
Footnotes
Acknowledgments
This work was supported by Shiraz University of Medical Sciences. We thank P. Waltl (AuthorAID in the Eastern Mediterranean) for improving the use of English in the manuscript. This report is based on research done in partial fulfillment of the requirements for the specialty degree in Urology (dissertation No. 89-01-01-2622) awarded to Dr. Hadian.
Disclosure Statement
No competing financial interests exist.